
Abstract
Background:
The position of the acetabular cup is important to the outcome of total hip athroplasty (THA). We devised an instrument that uses the level indicator application of smartphone together with a mechanical alignment guide to improve the precision of cup placement. This study aims to determine the percentage of acetabular cups positioned in the Lewinnek safe zone comparing between the conventional technique (using a mechanical alignment guide alone) and the smartphone technique (using a mechanical alignment guide combined with the devised instrument and smartphone).
Methods:
A historical controlled trial was conducted among 82 patients who underwent primary THAs through a posterolateral approach. In the conventional group, 41 cups were placed during January 2013 and December 2014, whereas 41 cups in the smartphone group were placed during January 2015 and March 2016. Inclination and anteversion angles were measured in standardized pelvic radiographs. The cup orientation was compared between groups.
Results:
The inclination angle in the smartphone group was significantly lower than in the conventional group (40.9° (SD 3.8) vs. 46.3° (SD 6.7), p < 0.001), but the anteversion angle was higher (19.6° (SD 4.4) vs. 16.5° (SD 6.1), p = 0.010). The smartphone group had more cups positioned in the Lewinnek safe zone (90.2% vs. 56.1%, p = 0.001) and longer operative times (136 (SD 27) vs. 119 (SD 23) min, p = 0.011). No significant difference was found for blood loss (p== 0.384) or dislocation rate (p = 0.494).
Conclusion:
Using the computerized function of smartphone could improve the precision of cup positioning. Most cups were placed within a narrow margin inside the Lewinnek safe zone.
Introduction
The acetabular component positioning is highly important to the function and outcome of total hip arthroplasty (THA). Achieving the optimal inclination and anteversion could potentially improve the longevity and range of motion of a THA and decrease the dislocation rate. 1 –3 Lewinnek et al. advocated an inclination angle of 40°±10° and an anteversion angle of 15°±10° as the safe zone for cup orientation. 4 These goals have been the most widely used targets for several decades although there is controversy in the literature regarding the ideal orientation. The percentage of acceptably placed cups in the Lewinnek safe zone varies from 25.7% to 70.5% reported in the literature. 5 These outcomes resulted from the conventional method of cup placement that was guided by intraoperative anatomical landmarks (free hand technique) or using mechanical alignment guides. Computer navigation can increase the percentage of placements in the safe zone up to 81%. 6 This proven advantage must be weighed up against the argument of prolonged surgery times and higher costs. 7
A smartphone that combines features of a personal computer operating system with other features of a mobile phone is an interesting choice to assist in surgery. The intraoperative use of smartphone technology in THA for improving the accuracy of acetabular cup placement was reported both in cadaveric and in clinical studies. Peters et al. used the accelerometer and camera function of an iPhone in a level indicator and protractor application to improve cup placement in 50 prospective cases. 8 They found good results with all cups being placed within the Lewinnek safe zone. Kurosaka et al. confirmed this iPhone/iPad technique in five cadavers and could achieve acceptable performance in determining the cup alignment regardless of the surgeon’s expertise. 9 However, these two studies assumed that there are neither preoperative errors in pelvic positioning nor intraoperative pelvic motion before cup placement. These conditions are unlikely to be met during THA.
We developed a pelvic inclinometer that uses the function of an accelerometer sensor of a downloaded bubble-level application in a smartphone. This application shows real-time tilting degrees along two axes. When it is held in the phone holder and fixed to the pelvis, it can monitor pelvic motion and present it in a digital number. For measuring the cup inclination, we used another smartphone with a downloaded angle-meter application. This smartphone was placed on top of the cup positioner, and the alignment guide was pointed parallel to the pelvic inclinometer before final seating. We wanted to investigate whether this instrument could improve the precision of cup placement in the Lewinnek safe zone. This study aims to determine the percentage of acetabular cups that were correctly positioned in the Lewinnek safe zone, comparing between the conventional method (using a mechanical alignment guide alone) and our technique (using a mechanical alignment guide combined with the invented instrument and smartphone).
Materials and methods
A prospective non-randomized, historical-controlled study was conducted among the adult patients who underwent cementless or hybrid THA from January 2013 to March 2016 through posterolateral approach by a single surgeon. These patients were divided into two groups. In the study group, 41 cups were prospectively placed during January 2015 and March 2016 using a mechanical alignment guide combined with our invented instrument and smartphone. In the historical-control group, 41 cups had been placed during January 2013 and December 2014 using a mechanical alignment guide alone. Exclusion criteria were patients with pelvic deformity or severe kyphoscoliosis.
Our pelvic inclinometer used a smartphone (Lenovo A390, China) and Smart Level application (version 1.0, androidboy1.blogspot.com). This program shows real-time tilting degrees of the smartphone along both the longitudinal and the transverse axes. The phone was enclosed in a zip bag (SunZip, Thailand) and placed in a holder that was made from a stretchable frame and adjustable adapter (Yunteng self picture monopod YT-188, China) with a stem made from an 11-mm diametered stainless tube (AO/ASIF, Switzerland). The base was a stainless steel frame with two screw holes at the lower end and a fixed standard clamp (AO/ASIF, Switzerland) at the upper end (Figure 1). This frame could be connected firmly and disconnected quickly during the surgery (Figure 2).

The pelvic inclinometer comprises (a) a smartphone (enclosed in a zip bag) and a plastic holder (stretchable frame and adjustable adapter) and (b) a stainless steel tube stem and base.

(a) The upper part of the stainless steel base was firmly connected to the lower part that was fixed into the iliac tubercle by two screws. (b) It could be disconnected quickly during the surgery.
There were three steps in the smartphone group:
Step 1. The pelvic inclinometer installation. After setting the operating table in neutral position, a skin staple was put over the tip of the coccyx as a radiographic marker. The patient was positioned in the lateral decubitus using two supports (posteriorly over the sacrum and anteriorly over the anterior superior iliac spine (ASIS)). The skin was prepared and partially draped. The inclinometer was securely fixed to the iliac tubercle by two self-drilling screws (No.12 × 2.5 inch, hex washer headed, zinc plated, Taiwan). The operative field was then covered with a sterile clear-plastic sheet.
Step 2. Standardization of the patient’s position. The pelvic position was verified using the cross-table fluoroscopy. A plumb was dangled on the image-reception screen and a long K-wire was taped on the screen to replace this plumb line (Figure 3(a)). The operating table was tilted so that the inter-teardrop line was parallel to the K-wire and the coccyx marker was in line with pubic symphysis. The C-arm was rotated horizontally until the positional relationship between the superior margin of pubic symphysis and the tip of coccyx on the fluoroscopic image was the same as the preoperative supine anteroposterior radiograph (Figure 3(b)). This plane was marked using a cross-line laser level (a tool commonly used for installing floor tiles) to touch the flat surface of the C-arm. It projected a laser line, perpendicular to the axis of the C-arm, on the border of the smartphone (Figure 4(a)). The thumb-screw knob of the smartphone holder was loosened and tightened again after the axis of the smartphone was adjusted horizontally parallel to the laser line (Figure 4(b)). The Smart Level application was calibrated to the relative position of the phone to 0° along both axes by touching the “calibrate” screen-icon (Figure 5). The inclinometer was then disconnected from its base and the surgeon finished draping (Figure 2(b)). For eliminating the positive effect of fluoroscopy, the operating table was tilted back to its initial position before starting the surgery.
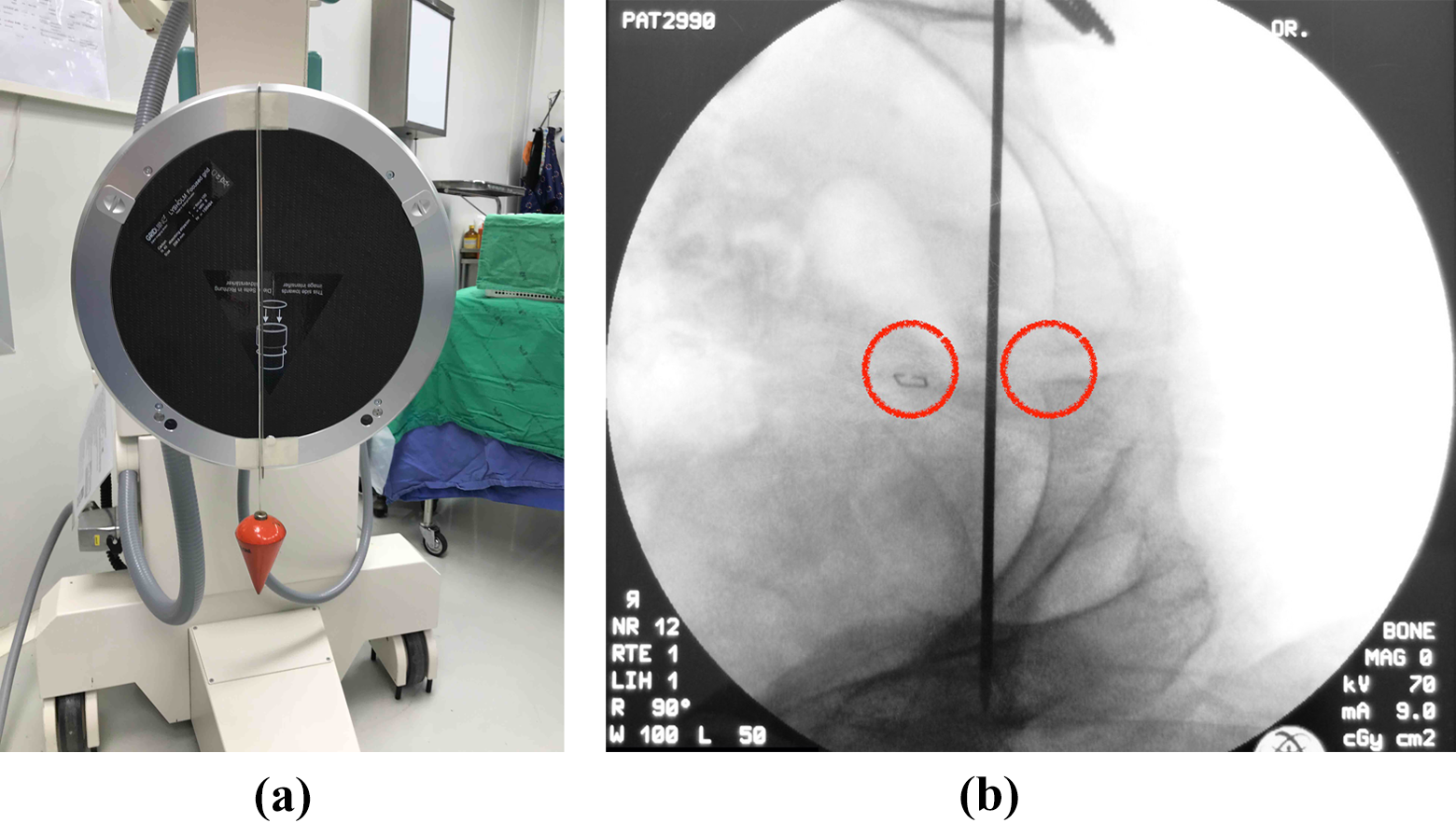
(a) A long K-wire was taped on the image-reception screen parallel to the plumb line. (b) Using cross-table fluoroscopy, the operating table was tilted until the inter-teardrop line was parallel to the K-wire, and the coccyx marker was in line with pubic symphysis. The C-arm was then rotated horizontally until the relative position of coccyx and pubic symphysis on the fluoroscopic image was similar to the pelvic radiograph.

(a) The pelvic tilt in sagittal plane of the patient was marked by placing a cross-line laser level on the flat surface of the C-arm. A laser line was projected beside the border of the smartphone. (b) The smartphone holder was adjusted horizontally until the axis of the smartphone was parallel to the laser line.

(a) The degree of pelvic tilt was shown in the Smart Level application. (b) It was calibrated to 0° along both axes by touching the “calibrate” screen-icon.
Step 3. Control cup positioner and alignment guide. Before the final cup placement, the inclinometer was reconnected to its base again, and the operating table was tilted back to return the pelvis to its standardized lateral decubitus position by obtain zero tilting degrees shown in both axes of the Smart Level application. The other smartphone (Lenovo A390, China) with the Clinometer application (www.plaincode.com) was placed on top and parallel to the cup positioner. To achieve the 40° target angle of radiographic inclination, the positioner was moved vertically together with the smartphone until 36° of operative inclination was shown in the application (Figure 6). The positioner was then moved horizontally until the mechanical alignment guide, set at 20° of operative anteversion, pointed 5° posterior to the border of the inclinometer smartphone by visual estimation before final cup seating.

To achieve 40° radiographic inclination, the positioner was moved vertically together with the other smartphone until 36° of operative inclination was shown in the Clinometer application.
In the control group, the patient was fixed in lateral decubitus using two supports after setting the operating table in neutral position as in the study group. No fluoroscopy was used to calibrate the pelvic position. Cup placement was performed using a mechanical alignment guide alone at the operative inclination about 40°. The guide, set at 20° anteversion, was pointed 5° posterior to the shoulder position of the patient to achieve 25° of operative anteversion.
In both groups, the posterior capsule and short external rotators were repaired. Antibiotic prophylaxis was intravenous cefazolin before skin incision and at 6-h intervals for 24–48 h. Two doses of tranexamic acid (500 mg) were given intravenously, one before skin incision and the other before closure.
The sample size was calculated to detect a significant difference in percentage of cup placement in Lewinnek’s safe zone. We hypothesized that the smartphone technique can achieve 81% in the safe zone, the same as with computer navigation, 6 whereas 52% of our previous THAs were positioned in the safe zone. With a two-sided type-I error level of 0.05 and an 80% statistical power of detection, the sample size was 41 hips in each group.
Preoperative demographic data included patient age, gender, body mass index, diagnosis, and cup type. Primary outcomes were radiographic inclination, radiographic anteversion, and percentage of cup placement in the safe zone. Pubic symphysis-centered pelvic anteroposterior radiographs were taken in the supine position at 6 weeks postoperatively. The inclination angle was measured between the inter-teardrop line and the long axis of the projected ellipse. The cup anteversion angle was measured and calculated using the Widmer method (Figure 7). 10

Radiograph demonstrating the inclination measurement and the Widmer method for measuring anteversion (anteversion = 48.05 × (2S/TL) − 0.3).
All radiographic measurements were performed by two orthopedic residents who were not involved with the surgery and repeated again 2 weeks later. The average of four measurements was used for data analysis. The intra-class correlation coefficients (ICCs) were calculated for intra-observer and interobserver reliability. We used the two-way random-effects model and absolute agreement for ICC calculation. The exact probability test was used to compare categorical data, whereas t-test was used to analyze continuous data, with a p-value of 0.05 being regarded as significant. This study was approved by our institutional review board and registered in the Thai Clinical Trials Registry. Informed consent was obtained from all patients who participated in the study
Results
There were 41 patients in each group enrolled in the study. The patients’ baseline characteristics were not significantly different between the two groups (Table 1). Plasmafit cups (Aesculap, Germany) were used in 50 cases (61%) and Trilogy cups (Zimmer, Warsaw, Indiana, USA) were used in 32 cases (39%). The mean inclination angle in the smartphone group was significantly lower than in the conventional group (40.9° (SD 3.8) vs. 46.3° (SD 6.7), p < 0.001). The mean anteversion angle in the smartphone group was significantly higher (19.6° (SD 4.4) vs. 16.5° (SD 6.1), p = 0.010; Table 2). The smartphone group had more cup placements in the Lewinnek safe zone than the conventional group (90.2% vs. 56.1%, p = 0.001; Figure 8). The ICC for intra- and interobserver reliability of inclination measurements was 0.97 (95% CI 0.95–0.98) and 0.93 (95% CI 0.91–0.95), respectively. The ICC for intra- and interobserver reliability of anteversion measurements was 0.84 (95% CI: 0.78–0.89) and 0.82 (95% CI: 0.75–0.87), respectively. The mean operative time was significantly longer in the smartphone group (136 (SD 27) vs. 119 (SD 23) minutes, p = 0.011).
Comparison of the baseline characteristics and prosthesis data of patients between the two groups.

BMI: body mass index; SD: standard deviation; ONFH: osteonecrosis of femoral head; DDH: developmental dysplasia of hip.
Comparison of radiographic measurements and percentage in the Lewinnek safe zone between the two groups.

SD: standard deviation.

Comparison of cup positions relative to the Lewinnek safe zone between the two groups.
Postoperatively, no significant differences were observed in total blood loss (p = 0.384), dislocation rate (p = 0.494), or surgical site infection (p = 1.000). The duration of follow-up was at least 2 years in all cases. Posterior dislocation occurred in two hips in the conventional group (Table 3). All of these had a cup orientation outside the safe zone. One hip in the smartphone group had superficial wound infection and was treated by local debridement.
Comparison of secondary outcomes between the two groups.

SD: standard deviation.
Discussion
The acetabular component positioning is one of the most important outcome measurements in THA. The cup orientation without regard to the safe zone is associated with poor outcomes, such as instability, accelerated wear, adverse local tissue reactions, tendinitis pain, and restricted range of motion. 11 Various definitions of safe zones have been advocated by both clinical and biomechanical studies. These safe zones vary between 20° and 55° inclination and 0° and 40° anteversion. 12 Among these, the most acceptable target was described by Lewinnek et al. 4 Argument whether this zone is ideal remains controversial. In a retrospective study by Abdel et al., the cup orientations in the majority of dislocated THAs were within the Lewinnek safe zone. 13 Similarly, a systematic review found that the Lewinnek safe zone is not suitable with respect to the risk of dislocation. Most articles assessing cup placement within the Lewinnek safe zone did not show a statistically significant reduction in dislocation rate. 14 Nevertheless, Elkins et al. conducted a finite-element analysis model and proposed the optimal landing zone to maximize stability and minimize wear. 12 In general, their ideal cup orientation is 42.5° ± 5.5° inclination and 17° ± 5° anteversion. Similar to a recent large cohort study, Danoff et al. redefined the posterior approach safe zone to be 30°–50° inclination and 10°–25° anteversion. 15 Their sweet spot safe zone (without dislocation) is 41.4° ± 4.3° inclination and 17.1° ± 4.3° anteversion. The optimal zones in both studies are narrower but remain within the Lewinnek safe zone.
There are three major causes of acetabular component malposition, namely, preoperative errors in the pelvic positioning, intraoperative changes in the pelvic tilt, and intraoperative errors in the manual operation. 16 The first cause can be solved using cross-table fluoroscopy to verify the pelvic position in lateral decubitus. The operative table is tilted in the coronal (abduction and adduction) and transverse planes (anteversion and retroversion) of the patient until the pelvic fluoroscopic image is symmetrical and perpendicular to the floor. For the sagittal plane (flexion and extension), the C-arm is rotated horizontally until the positional relationship between the pubic symphysis and coccyx on the fluoroscopic image is similar to the preoperative radiograph. This plane can be marked by adjusting the lateral border of the smartphone to be parallel to the laser line, projecting perpendicularly from the C-arm as in our technique, or by marking the C-arm orientation on the floor with tape so that it can be seen clearly during the surgery as described by Nishikubo et al. 16 They used this technique to correct the errors of pelvic tilt through repositioning of the operating table using fluoroscopy before surgery and could place the acetabular component within an adequate zone (inclination 30°–50° and anteversion 10°–30°) in 84.3% of hips.
The second cause of cup malposition can be solved by our pelvic inclinometer. After the patient position is standardized in lateral decubitus, this position is memorized in the smartphone application by calibration to 0°. Intraoperative pelvic motion can be assessed by the level application, and the pelvis can be repositioned to 0° of tilting before cup placement, by turning the operating table. This is the same principle as the gravity-assisted guidance system studied by Echeverri et al. 17 and the pelvic tilt goniometer used by Asayama et al. 18 Echeverri et al. used a bull’s-eye bubble level fixed to a Shanz pin and placed in the iliac crest. It acts as a reference, identifying the initial yaw and roll positions throughout the operation. 17 However, the mechanical bubble level does not show a degree of tilting and could not be calibrated to 0° at any position of the device. Asayama et al. used a specially devised goniometer to measure pelvic motion in real time during surgery. The device incorporated a digital compass with two goniometers as well as a pendulum and target apparatus. It was fixed to a threaded Steinmann pin that inserted into the ASIS. 18 They suggested that the surgeon was better able to accurately achieve the desired cup placement with the real-time visual feedback about the pelvic orientation and motion. Nevertheless, their pelvic tilt goniometer is more complicated, larger, and heavier than our invented inclinometer. Fixation to the pelvis with only one threaded pin might be weaker than with two screws. Our device can be disconnected and does not interfere with the operative field during surgical exposure.
The intraoperative errors in the manual operation can be solved by our technique that uses a smartphone combined with an alignment guide. The smartphone is placed parallel to the cup positioner, and inclination measurement can be done following the previously described method. 8,9 Peters et al. advocated the operative inclination at 40° from their surgical experience, 8 while Kurosaka et al. recommended 38° following the Murray’s equation and cadaveric study with the Orthopilot navigation system. 9,19 Both studies aimed the 15° target of radiographic anteversion. Our technique aimed 36° operative inclination and 25°operative anteversion following the Murray’s equation to achieve the targets of 40° radiographic inclination and 20° radiographic anteversion. 9 It provided an average of 40.9° inclination and 19.6° anteversion in postoperative radiographs of this study.
The percentage of acetabular cups positioned in the Lewinnek safe zone was significantly higher in the smartphone group. The scatterplots showed less scattered distribution of cup orientation than in the conventional group. These improved inclination and anteversion angles came from the use of both smartphones because the positive effect of fluoroscopy for pelvic standardization was eliminated by the return of operating table to its initial position before starting the surgery. It could be assumed that the pelvic position at the time of skin incision was not different between groups. Two hips in the conventional group had posterior dislocation. One of them had anteversion of 1° and the other had inclination of 54°. We found no significant difference in dislocation and infection rates between the two groups, and this might be from the inadequate sample size. The calculated sample sizes with 80% power to compare the dislocation and infection outcomes at the same rates require 194 and 410 hips in each group, respectively. Nevertheless, this study has a power of 95.1% (type I error 5%) to detect the outcome of safe zone outliers.
There are some limitations in this study. Firstly, it was not a concurrent study and so might be biased by the period effect especially from surgeon experience. However, those THAs in the conventional group were performed by the same surgeon who had passed the learning curve of such operations more than 10 years previously. Secondly, our technique had some complexity that needed a learning curve for fluoroscopic control and instrument installation. The outcome might be better if the surgeon is familiar with them. Thirdly, we measured radiographic anteversion angles using the Widmer method, 10 which might have variation in each measurement. Currently, reformatted CT scan is considered to be the gold standard for cup anteversion measurement, 20 but it needs special software that is not available in our hospital. However, measurements using the Widmer method are the most similar to those using reformatted CT, with a mean difference of −0.9°. 20 The ICC for reliability of anteversion measurements in this study was also at a good level. To the best of our knowledge, this is the first clinical study that uses a smartphone as a pelvic tilt goniometer. Moreover, our method is a novel technique for cup orientation in the Lewinnek safe zone and capable of solving three major causes of cup malposition.
Conclusion
Using the computerized function of smartphone could improve the precision of cup positioning in THA. It can be used with different cup positioners of different companies in the lateral decubitus position. Most acetabular cups were placed within a narrow margin inside the Lewinnek safe zone.
Footnotes
Acknowledgment
The authors would like to thank Andrew Sherratt for his help in approving the English language use.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.