
Abstract
Purpose:
To investigate the change in incidence of referred carpal tunnel syndrome (CTS) and carpal tunnel release (CTR) surgery over time and regional variations.
Methods:
From the nationwide patient registry, we identified all adult individuals who had received first-time CTS diagnosis (International Classification of Diseases, 10th Revision code G560) at secondary or tertiary level and first-time CTR surgery during the period of 9 years.
Results:
From 2001 through 2009, the incidence (per 100,000 person-years) of CTS diagnosed at secondary or tertiary level increased from 216 to 243 in women and from 95 to 119 in men and of CTR from 117 to 168 in women and from 52 to 78 in men. The mean annual increase in first-time CTR (95% confidence interval) was 5.1% (4.7–5.4) in women and 6.2% (5.6–6.7) in men. The age-standardized 3-year (2007–2009) incidence varied significantly across Sweden’s 21 counties; compared to the county with the lowest incidence of CTR, the incidence rates in the other counties were higher by 6–152% (mean 60%) in women and by 20–182% (mean 85%) in men. The proportion of CTS-diagnosed individuals treated with surgery varied across counties from 53% to 81% in women and from 51% to 77% in men.
Conclusion:
The incidence of referred CTS and of CTR surgery increased over time in both sexes, with large regional variations found in the incidence rates and in the proportion of individuals treated with surgery.
Introduction
Carpal tunnel syndrome (CTS) is a common cause for patients to seek health care. 1 Reported risk factors for CTS are obesity, higher age, pregnancy, work activities demanding frequent use of force and of hand-held vibratory tools, and medical conditions, such as diabetes, rheumatoid disease, and thyroid disorders. 2 Although nonoperative treatments may be effective, many patients still need carpal tunnel release (CTR) surgery. There is strong evidence supporting that CTR is highly effective in relieving symptoms and improving function and quality of life 3 and that the benefit is durable. 4 Long-term efficacy of other treatments has not been established. 5,6 Despite the continuing research about various treatment methods in CTS, little is known about whether treatment trends have changed over time. For a common condition such as CTS, knowledge about whether and to what extent use of surgical treatment increases would be important for clinical practice and for health-care planners and providers.
Based on studies that have estimated incidence of CTS, there appears to be large differences between countries. 7 –11 However, little data exist on regional variations in the incidence of CTS within counties. A few studies from North America and Europe have shown substantial within-country regional variations in the incidence of CTR. 12 –15 However, these studies were limited to specific regions within a country rather than to a whole general population. Variations in the incidence of CTS and CTR between countries and between different regions could reflect true differences in incidence but may also reflect differences in the way doctors diagnose and treat patients with CTS. The aim of our study was to investigate the change in the nationwide sex- and age-specific incidence of referred CTS and of CTR surgery over time and regional variations.
Materials and methods
This is a retrospective population-based study. Data were retrieved from the patient registry managed by the Center for Epidemiology at the Swedish National Board for Health and Welfare. This nationwide registry covers all patient visits (outpatient and inpatient care) to a medical doctor at secondary- and tertiary-level health-care facilities (i.e. hospital or similar specialist health-care facility) and all medical interventions performed at these facilities. We identified all individuals aged ≥18 years who had consulted a medical doctor during a 9-year period (January 2001 through December 2009) and received the diagnosis CTS (International Classification of Diseases, 10th Revision (ICD-10) code G560). The registry does not specify how the diagnosis of CTS has been made by the physician (on clinical grounds only or in combination with nerve conduction tests). We also identified all individuals who had CTR surgery (received the code ACC51 according to the Swedish Classification of Healthcare Interventions) in conjunction with CTS diagnosis. Data collected included sex, age at the time of diagnosis or surgery, consultation dates, surgery dates, health-care facility, county of residence, type of visit (outpatient or inpatient), primary diagnosis and any other associated diagnoses (up to eight diagnoses were allowed), and surgical procedures and other interventions performed. Each individual was included in the analyses only once (first-time diagnosis and first-time surgery). The study was approved by the Regional Ethical Review Board.
Statistical analysis
We retrieved annual data on population statistics from Statistics Sweden. 16 For each study year, we used the population data on December 31 in the preceding year. We calculated the sex- and age-specific incidence rates of CTS and CTR surgery (overall rates and for the 21 counties) and 95% confidence intervals (CIs) using Poisson regression models. Analyses of incidence trends over time were performed. The at-risk population was standardized with weights from the 2013 European standard population. We used the county with the highest population as referent to obtain adequate number of individuals in all age-groups. For county comparisons, we used the incidence rates during the study’s last 3 years (2007–2009) to reflect the most recent data and calculated age-adjusted incidence rate ratios (IRR) and 95% CIs. Statistical significance was defined as a p-value of <0.05. All analyses were performed with STATA (STATA SE 14.2, StataCorp, College Station, Texas, USA).
Results
Incidence of referred CTS
During the 9-year study period, 75,799 women and 32,900 men were diagnosed with CTS at a secondary- or tertiary-level health-care facility. The incidence (95% CI) of first-time CTS per 100,000 person-year was 232 (230–233) in women and 104 (103–105) in men. The incidence of first-time CTS diagnosis increased over time; the mean increase (95% CI) per year in women was 1.8% (1.5–2.1, p < 0.01) and in men was 3.9% (3.5–4.4, p < 0.01). The incidence peaked in ages 50–54 years in women and 75–79 years in men (Figure 1); this was consistent across the country. Compared to the referent age-group (≥85 years), the IRR for first-time CTS ranged from 0.05 to 1.74 in women and from 0.04 to 1.97 in men (Supplementary Table S1).

Sex-specific incidence of first-time carpal tunnel syndrome diagnosed at secondary or tertiary level and of first-time carpal tunnel release surgery 2001–2009.
The crude regional incidence of CTS diagnosis during the 3-year period 2007–2009 ranged from 199 to 324 per 100,000 person-year in women and from 85 to 187 per 100,000 person-year in men, with significant regional variations shown in the age-standardized incidence (Figure 2(a)). Compared to the referent county, the age-standardized incidence rates of CTS diagnosis in the other counties were higher by 7–63% (mean 37%) in women and by 18–126% (mean 59%) in men (Supplementary Table S2).
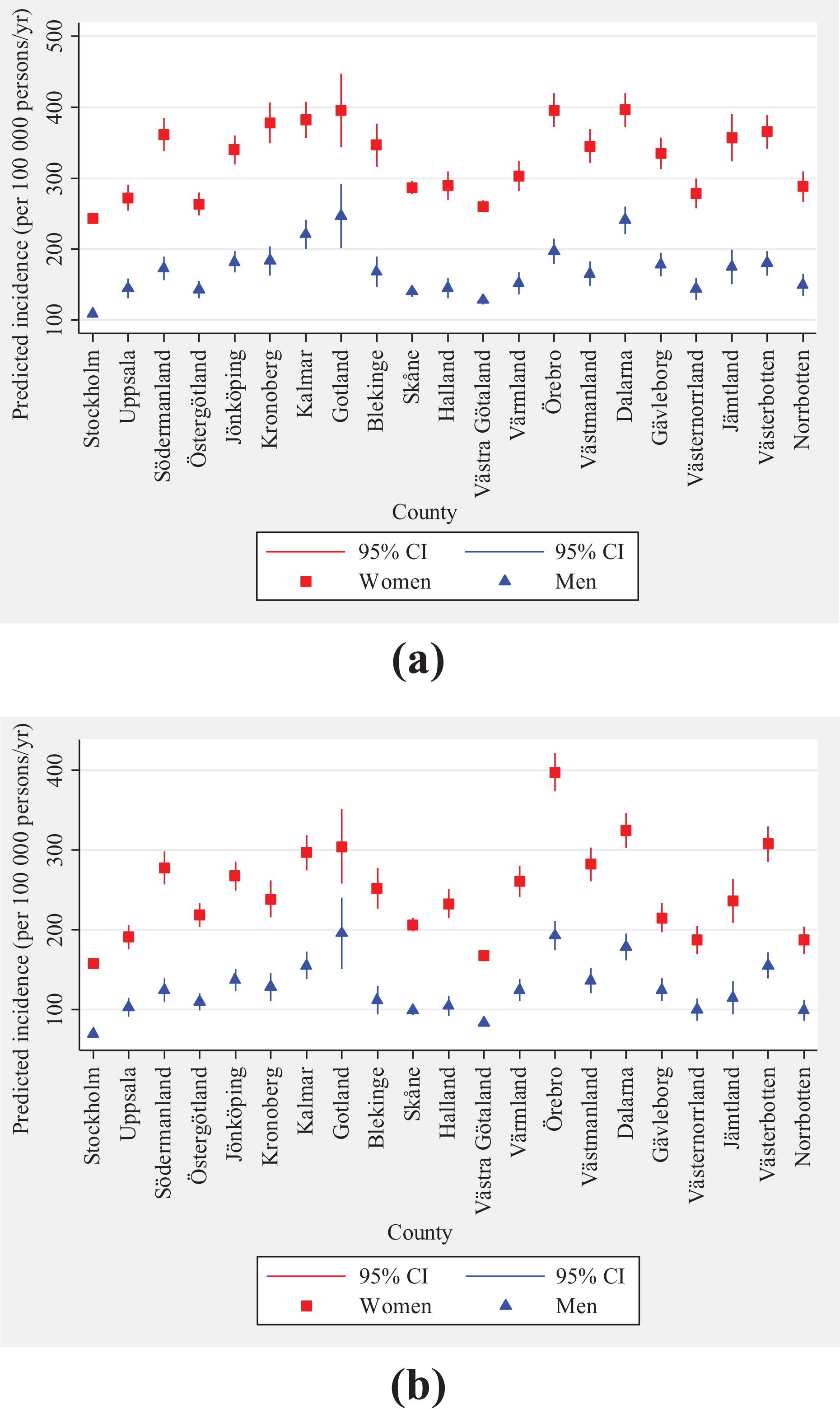
Regional variation in the age-standardized incidence of (a) first-time carpal tunnel syndrome diagnosed at secondary or tertiary level and (b) first-time carpal tunnel release surgery 2007–2009.
Incidence of first-time CTR surgery
Of the 108,699 individuals with CTS diagnosis, 70,120 (65%) had CTR surgery, of them 49,440 (65%) were women and 20,680 (63%) were men. The incidence (95% CI) of first-time CTR surgery per 100,000 person-year was 151 (150–152) in women and 65 (64–66) in men. The incidence of CTR surgery increased over time both in women and in men; the mean increase (95% CI) per year was 5.1% (4.7–5.4, p < 0.01) in women and 6.2% (5.6–6.7, p < 0.01) in men. The incidence of CTR surgery peaked in ages 50–54 years in women and 75–84 years in men (Figure 1); this was consistent across the country. Compared to the referent age-group (≥85 years), the IRR for CTR surgery ranged from 0.03 to 1.74 in women and from 0.02 to 2.03 in men (Supplementary Table S1).
The crude regional incidence of first-time CTR surgery during the 3-year period 2007–2009 ranged from 126 to 316 per 100,000 person-year in women and from 52 to 142 per 100,000 person-year in men, with significant regional variations shown in the age-standardized incidence (Figure 2(b)). Compared to the referent county (county with the lowest incidence), the age-standardized incidence rates of first-time CTR in the other counties were higher by 6–152% (mean 60%) in women and by 20– 182% (mean 85%) in men (Supplementary Table S2).
Proportion treated with surgery
The proportion of individuals with CTS who had CTR surgery was the lowest in the ages 18–29 years (women 52%, men 52%) and highest in the age ≥80 years (women 69%, men 73%). The proportion across counties ranged from 53% to 81% in women (<60% in 3 counties, 60–70% in 11 counties, and >70% in 7 counties) and from 51% to 77% in men (<60% in 5 counties, 60–70% in 15 counties, and >70% in 1 county).
Discussion
Our study shows that CTS diagnosis and CTR surgery are common in the general population, more common in women than in men, and increase with age. The incidence rates of CTS and of CTR surgery peak at ages 50–59 years in women, but in men they continue to increase with age, up to 85 years. However, the proportion of CTS-diagnosed persons treated surgically is similar in women and men in all age-groups. An interesting feature was the bimodal incidence of presentation and surgery present in both women and men with peaks at around 50–60 years and 75–84 years and a dip at 65–69 years (Figure 1). Although it is well established that CTS affects women more than it affects men the higher incidence of diagnosis may also be influenced by whether more women than men seek health care. However, data regarding ulnar nerve decompression for cubital tunnel syndrome in Sweden during 2005–2016 show that, unlike CTR, the incidence in men and women was similar (ranging from 15 to 18 per 100,000 adults per year). 17
Similar to our results, other studies have generally shown a trend for increasing incidence of CTS over time. 7,8,18 Possible explanations are higher prevalence of risk factors, such as obesity and diabetes, in the general population of Sweden over time, 19,20 general increase in the life span, improved public health leading to better recognition of CTS by medical professionals and patients, and increased use of nerve conduction tests leading to increased CTS diagnoses.
Also similar to our results, other studies have shown a trend for increasing incidence of CTR surgery over time. 18,21 In our study, the incidence of CTR surgery per 100,000 person-year was 151 in women and 65 in men. In a previous study that compared the incidence in Sweden and the United States during 1999–2008, 1 the annual incidence of CTR surgery per 100,000 persons (standardized to US population) in women was 166 in Sweden and 171 in the United States, and in men was 58 and 96, respectively. As the incidence of CTS diagnosis increases, it is also reasonable that the incidence of surgery increases. However, the proportion of individuals with CTS who had surgery has also increased over time. Reasons for this increase could be the increasing evidence supporting the effectiveness of CTR 3 and durability of the benefit 4 as well as possibly improved access to day surgery. Our study shows that surgery has on average increased by 5–6% annually. This should have implications for clinical practice and for health-care providers and planners.
Our study shows substantial regional variations in the proportion of persons diagnosed with CTS (at specialist health-care facilities) who are treated with surgery. The findings suggest differences in CTS diagnosis and treatment across different regions in Sweden. Regional variations have also been shown in other countries. A previous study from the United States has shown large regional variation in the incidence of surgery for CTS, ranging from 82 to 287 per 100,000 persons in 1993. 12 A study from Italy reported rates from 50 to 132 per 100,000 person-year from 1997 to 2002. 14 A study from Catalonia, Spain, reported CTR rates ranging from 76 to 172 between 1995 and 2000, while another study from Valencia reported rates from 11 to 128 per 100,000 persons in 2006. 15 To the best of our knowledge, our study is the first to be based on data from an entire country over a time period of 3 years (2007–2009). Regional variations in diagnosis and treatment may be influenced by occupational factors. However, based on the population characteristics in the counties, the large variations shown cannot be explained only by demographic or occupational factors. Access to specialist care and the ability to diagnose and treat may be important factors.
The CTS incidence rates in our study apply to referred CTS diagnosed at secondary and tertiary levels because the patient registry does not cover primary care. Little has been known previously about the incidence of CTS diagnosed beyond primary care (i.e. patients who had not responded to treatment or the diagnosis was uncertain at primary care and therefore referred to specialist care). In a previous population-based study in Skåne county in southern Sweden, the incidence (2006–2008) of doctor-diagnosed CTS (including in primary care) per 100,000 person-year was 428 (95% CI: 416–440) in women and 182 (95% CI: 174–190) in men. 1 Our results for Skåne county showed the incidence of referred CTS was 250 (95% CI: 245–255) in women and 113 (95% CI: 110–117) in men, which is lower because it did not include patients exclusively managed at primary care. This suggests that about 60% of patients who are diagnosed with CTS in primary care are referred for specialist evaluation.
The incidence of CTR surgery estimated in our study represents the incidence of the procedure in the general population because almost all health-care facilities where CTR surgery is performed report to the registry. It is possible that some procedures performed in small individual private practices may not have been registered, but the majority of surgical procedures in Sweden are performed in public hospitals. Also, a large proportion of surgeries performed in private practice are done in health-care facilities that report to the registry. A possible limitation of our study is that the regional variation could be influenced by the completeness and accuracy of reporting diagnosis and intervention codes. However, for analysis of regional variations, we used data from the last 3 years of the 9-year study and CTR, being a common surgical procedure, is expected to be well registered. The patient registry contains only the diagnosis of CTS with no details on how it was established. The diagnosis could have been made on clinical grounds only or also confirmed with nerve conduction tests, but for a nationwide registry-based study, it is not possible to access patients’ individual medical records for further information.
Conclusion
Our study shows that during the years 2001–2009, the incidence of CTS diagnosis and of CTR surgery in the general population of Sweden increased over time among both women and men; the mean annual increase in CTS diagnosis was 2–4% and of surgery was 5–6%. Women are approximately twice as likely as men to present, but the rate of surgery is similar in women and men, at approximately two-thirds. It also shows substantial regional variations in the incidence of CTS and of CTR as well as in the proportion of CTS-diagnosed persons who receive surgical treatment. Awareness of these regional variations in both diagnosis and surgery would stimulate clinicians to consider how they manage patients with CTS and may reduce unexplained variation in health care for this condition.
Supplemental material
Supplementary_material - Incidence of referred carpal tunnel syndrome and carpal tunnel release surgery in the general population: Increase over time and regional variations
Supplementary_material for Incidence of referred carpal tunnel syndrome and carpal tunnel release surgery in the general population: Increase over time and regional variations by Kamelia Tadjerbashi, Anna Åkesson, and Isam Atroshi in Journal of Orthopaedic Surgery
Footnotes
Author contributions
Isam Atroshi contributed to conception and design of the study; Kamelia Tadjerbashi and Isam Atroshi contributed to data acquisition; Kamelia Tadjerbashi, Anna Åkesson and Isam Atroshi performed data analysis and data interpretation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported and partially funded by Hässleholm Hospital. The funder had no role in the design, the collection, analysis and interpretation of data, the writing of the manuscript or the decision to submit the manuscript for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.