
Abstract
Background:
The goal of this study was to evaluate the clinical effect of Regan–Morrey type II comminuted coronoid process fracture treated with mini plate through the direct anterior approach (DAA).
Methods:
Ten patients who underwent open reduction and internal fixation (ORIF) with mini plate through the DAA between February 2013 and August 2016 was included. There were three women and seven men, with an average age of 34.4 ± 7.5 years. At the final follow-up, the Mayo Elbow Performance Index (MEPS), Visual Analogue Scale (VAS) score, Disability of the Arm, Shoulder, and Hand (DASH) score, and the elbow range of motion were noted.
Results:
The mean follow-up was 26.3 ± 2.2 (range 24–31) months. The mean elbow arc of motion was 118.5° with a mean arc of extension of 4° ± 5.2° and flexion of 122.5° ± 7.2°.The mean forearm pronation was 72° ± 7.2°, and the mean supination was 68° ± 6.3° with a mean forearm rotation arc of 140°. The average postoperative score according to the MEPS was 91 ± 5.7 points (range 80–100 points), and all patients achieved satisfactory scores (8 excellent and 2 good). The final average VAS score was 0.6 ± 1 (range 0–3). The final average DASH score was 4.0 ± 1.6 (range 2.3–7.4). None of the patients complained about elbow instability that required secondary surgery. No complications of infection, joint incongruency, fracture nonunion, median nerve palsy, or implant failure were reported.
Conclusions:
ORIF with mini plate through the DAA for the treatment of the type II comminuted coronoid process fractures can achieve satisfactory outcomes.
Keywords
Introduction
The coronoid process of the ulna represents a primary stabilizer of the elbow joint and loss of its integrity following fracture can lead to instability and subsequent post-traumatic osteoarthritis. 1 Fractures of the coronoid process of the ulna generally occur in relatively high-energy injuries and are most often associated with other bony and soft tissue injuries around the elbow. 2 Approximately 60% of the anteromedial facet of the coronoid process is unsupported by the proximal ulnar metaphysis, which makes it vulnerable to fracture. 3 –5 As the keystone to elbow stability, any injury to the coronoid, small or large, can almost be assumed to induce inherent instability to varying degrees. 6 Various approach and implants for coronoid fixation have been described. There is no universally accepted approach 7 and implant to the elbow for the fixation of coronoid process fractures. The type II comminuted coronoid process fracture usually appears as many small piece fragments. They are difficult to fix using wires, anchors, or screws through conventional approaches, so we use the mini plate for fixation through direct anterior approach (DAA). The purpose of the present retrospective study was to evaluate the clinical effect of mini plate for fixation of the type II comminuted coronoid process fracture through the DAA.
Materials and methods
After approval from the institutional review board, 10 patients of the type II comminuted coronoid process fractures underwent open reduction and internal fixation (ORIF) by mini plate through the DAA and was included in this retrospective study between February 2013 and August 2016. There were three women and seven men, with an average age of 34.4 ± 7.5 years (range 24–47) at the time of index operation. All the patients were closed fractures. Leading causes of the fractures were traffic accidents and fallen from height. At the emergency department, all fractures were evaluated by X-ray and three-dimensional computed tomography (CT). The fracture comminution was evaluated by three-dimensional CT. Patients with elbow dislocation (8 of 10) were initially treated in the emergency department with closed reduction and splinting (Figure 1). Intraoperatively, the presence of a collateral ligament injury was confirmed by C-arm X-ray fluoroscopy. Coronoid process fractures were classified according to Regan and Morrey classification and O’Driscoll classification. We complete the Mayo Elbow Performance Index (MEPS), 8 Visual Analogue Scale (VAS) scores, and Disability of the Arm, Shoulder, and Hand (DASH) 9 scores at the final follow-up. Detailed information about associated injuries, classification of fractures, month of follow-up, final elbow arc of motion, MEPS, VAS scores, DASH scores, and complication was collected (Table 1).

Preoperative radiographs of a 31-year-old man with type II comminuted coronoid process fracture with posterior dislocation of the elbow and MCL injury (a and b) and preoperative radiographs and three-dimensional CT of closed reduction of elbow (c to f). MCL: medial collateral ligament; CT: computed tomography.
Data of patients.

M: Male; F: Female; MCL: medial collateral ligament; LCL: lateral collateral ligament; D: dislocation; R & M: Regan and Morrey; RHF: radial head fracture; MEPS: Mayo Elbow Performance Score; VAS: visual analog scale; DASH: disability of the Arm, Shoulder, and Hand.
Operative technique
Under general anesthesia, the patient was placed in the supine position and the injured upper limb was placed on a radiolucent operating table, with a tourniquet around the proximal arm. A longitudinal skin incision before the coronoid process was made from the elbow flexion crease to about 5 cm distal to the flexion crease (Figure 2). Bicipital aponeurosis is exposed underneath of the subcutaneous tissue and incised perpendicular to the aponeurotic fibers. After bicipital aponeurosis is incised, the nerve and vessels are exposed by blunt dissection slowly and carefully. Brachial artery and median nerve should be identified and protected. The brachial artery is retracted laterally, whereas the median nerve is retracted medially (Figure 3(a) to (c)) providing the best exposure of the brachial muscle with the elbow in 20–30° of flexion. A longitudinal muscle split and retraction provided good visualization of the anterior capsule, ulnar coronoid fracture fragment, and base of the coronoid process. The reduction of the comminuted coronoid process fracture is performed under direct visualization, followed by fixation with a mini plate (Stryker GmbH, VariAx Hand Non-locking Plating System, Freiburg, Germany; Figure 4). Associated radial head fracture and lateral collateral ligament (LCL) injury were repaired using a lateral incision. Associated medial collateral ligament (MCL) injury was repaired using a medial incision. Following rigid fixation of fracture and ligament, stability of elbow is assessed again under fluoroscopy.
Photograph of a surgical incision.
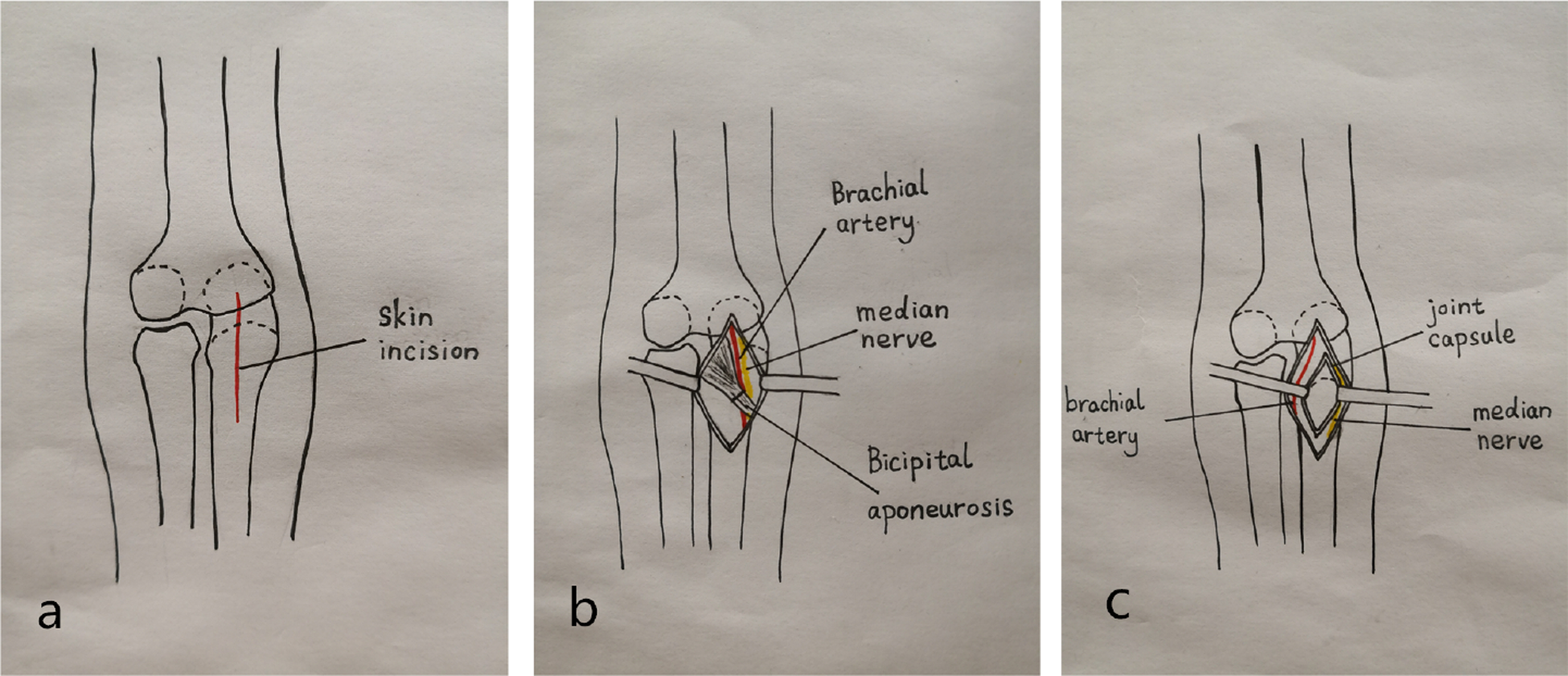
Illustration depicting the DAA to the coronoid process fracture fragment. DAA: direct anterior approach.

Postoperative radiographs of ORIF with mini plate through the DAA. ORIF: open reduction and internal fixation; DAA: direct anterior approach.
Postoperative management
Postoperatively, elbow was immobilized in a long arm splint with 90° of flexion and neutral forearm rotation for 1 week. The patients were requested to take nonsteroidal anti-inflammatory drugs 1 week after surgery for reducing the probability of heterotopic ossification. As pain and swelling gradually subsided after 1 week, the patient was allowed to practice gentle passive and active elbow motion. The allowed range of active motion was gradually increased. However, abduction of the shoulder was strictly avoided for 1 month 10,11
Follow-up and functional evaluation
All patients were regularly followed up at 4 weeks, 8 weeks, 12 weeks, 6 months, 12 months, and yearly thereafter. At the final follow-up, the elbow range of motion, including arc of motion (extension/flexion) and forearm rotation (pronation/supination), was measured with a goniometer. Postoperative scores according to the MEPS, VAS, and DASH were evaluated at the final follow-up. Radiographs were reviewed for signs of arthrosis with the use of scale of Broberg and Morrey. 12 The postoperative complications, including mild pain and osteoarthritis, were tabulated.
Ethics approval
Our study involving human participants was approved by the institutional review board of each participating hospital. No animals were used in the study.
Results
Follow-up was at least 24 months for all patients (mean 26.3 ± 2.2 months, range 24–31 months). The mean elbow arc of motion was 118.5° with a mean arc of extension of 4° ± 5.2° and flexion of 122.5° ± 7.2°. The mean forearm pronation was 72° ± 7.2°, and the mean supination was 68° ± 6.3° with a mean forearm rotation arc of 140°. A typical case is shown in Figure 5. The average postoperative score according to the MEPS was 91 ± 5.7 points (range 80–100 points), and all patients achieved satisfactory scores (8 excellent and 2 good). The final average VAS score was 0.6 ± 1 (range 0–3). The final average DASH score was 4.0 ± 1.6 (range 2.3–7.4). All 10 fractures were united, and no joint incongruity, dislocation, or subluxation of the injured elbow was observed. One patient had mild arthritic changes on the final follow-up radiographs. One patient reported mild pain during repeated exertion and forceful use of the arm. None of the patients complained about elbow instability that required secondary surgery. No complications of infection, joint incongruency, fracture nonunion, median nerve palsy, or implant failure were reported.

Good function was achieved at the 3-month follow-up.
Discussion
The coronoid process is critical to elbow stability and is vulnerable during injury. 11 The coronoid process extends both anteriorly and medially from the ulnar metaphysis, making it relatively thin and susceptible to injury in these areas. 3,6 The coronoid process has four important soft tissue insertions such as the anterior joint capsule of the elbow, the brachialis muscle, and the anterior band of MCL and LCL. 13 Fractures of the coronoid process of the ulna generally occur in relatively high-energy injuries. Above all, the fracture of coronoid process usually appears as comminuted fracture and requires sufficient fixation to allow for early rehabilitation.
Because of the special anatomical and biomechanical features of the coronoid process, a fracture, especially combined with elbow dislocation and collateral ligament injury, requires surgical treatment. The optimal management of the coronoid fracture remains controversial, including approach 7 and implant.
Repair of coronoid fractures has been usually described from medial, 14,15 lateral, 15 and posterior approaches 6,15 as well as a combination of these. All the above approaches are used under a certain condition and have defects. Approach from the medial side is generally recommended for the isolated coronoid fracture. But through the medial approach, it is hard to expose the anterior and anterolateral part of the coronoid process, and it needs relatively long incision and more soft tissue dissection such as flexor carpi ulnaris and flexor–pronator mass. 16 In addition, ulnar nerve palsy and idiopathic ulnar neuropathy can occur as a result of a medial approach. 11 Approach from the lateral side under the condition of the radial head fracture is comminuted, and prosthetic replacement is planned. Analogously, it is hard to expose the anterior and anteromedial part of the coronoid process. 15 Approach from posterior should be preferentially utilized when the olecranon is fractured. The coronoid fracture can be exposed through the olecranon fracture site. 6 However, exposure and fixation of the coronoid are prone to difficulties as well. 17 The above incisions fail to provide the greatest exposure of a coronoid process fracture.
The anterior approach to the elbow has been reported by Henry 18 and Urbaniak et al. 19 in early years. Recent studies 17,20 –23 have reported modified anterior approach for the treatment of coronoid process fracture. We further modified the approach on this basis and chose the DAA below the antecubital fossa for its unique advantages, including minimal soft tissue dissection, wide and clear operation field, direct vision for the open reduction, strong fixation caused by vertical compression of the fracture fragment, and early functional exercises. 17
In recent studies, the operative management of the coronoid fracture remains challenging. Options include a suture lasso technique, 14 suture anchors, 14,17 lag screws, 14,17,24,25 or plates. 5,7,14,15,26 Garrigues et al. 14 reported that a retrospective chart review performed at three tertiary care centers identified 40 consecutive patients treated for terrible triad injuries of the elbow with a minimum follow-up of 18 months. They found that suture lasso fixation of the coronoid fracture leads to fewer complications and improved outcomes compared with screw or suture anchor fixation techniques. ORIF was associated with a higher prevalence of implant failure, and suture anchors were associated with a higher prevalence of malunion and nonunion. For comminuted coronoid process fracture, small coronoid fracture fragments associated with complete elbow dislocation are often too small to be secured with screws. Most of these fractures are best repaired with a suture or suture anchor. 26 But suture or suture anchor alone is not capable to hold the small pieces together and cannot provide sufficient fixation for multifragment fractures. The use of anchors or suture anchor can easily lead to complications such as wire cutting, loosening, and refracture. Plate fixation for comminuted coronoid process fracture is controversial. This technique can also allow for early rehabilitation of the elbow.
The present study had several limitations, including the lack of a comparison group, the small sample size, and short follow-up time. A randomized controlled trial is needed.
Conclusion
The DAA with mini plate fixation could be an alternative surgical treatment for Regan–Morrey type II comminuted coronoid process fracture. It has the benefits of safety, minimal invasion, excellent operation field, direct vision for the open reduction, strong fixation caused by vertical compression of the fracture fragment, and satisfactory prognosis.
Footnotes
Authors’ note
Jian-Jian Shen and Qing-Mi Qiu are co-first authors of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.