
Abstract
Acromio-clavicular (AC) joint injuries are a common injury seen in athletes and represent 9% to 12% of all shoulder injuries. There is no clear consensus on treatment of grade 3 injuries. We conducted a survey among upper limb surgeons in the United Kingdom to review commonly accepted practise. We found that majority of surgeons never did stress view. Most surgeons favoured surgery only if needed but not first choice. There is no consensus on timing of surgery. There are many fixation options available for AC joint dislocation and we found that surgeon’s preferences were quiet wide for choosing fixation method. That is also evident from this questionnaire as there is no consensus in orthopaedic surgeons for ideal treatment of type 3 AC joint dislocations. Authors recommend randomized controlled trial to formulate definite treatment plan.
Keywords
Introduction
Acromio-clavicular (AC) joint injuries are a common injury seen in athletes and represent 9% to 12% of all shoulder injuries. 1 –5
These injuries are classified by Rockwood which is based on severity of soft tissue injury and AC joint displacement on Anteroposterior (AP) and axillary view. Treatment of grade 1 and 2 is conservative and grade 4–6 is mainly surgical. But there is no clear consensus on treatment of grade 3 injuries. AC joint injury mainly happens in younger patients. 6
Advocates of non-operative treatment suggest that patients often regain excellent clinical results and painless shoulder function; although for some there is the potential for chronic instability and pain. 7,8 Alternatively, operative treatment strategies are able to address these shortcomings but occasionally compromise shoulder function. 7,9
Korsten et al. in their systematic review observed a higher complication rate in the operative treatment group, which is an obvious consequence of the invasive procedure. In six surgically treated patients, a surgical revision or additional treatment was indicated, and therefore clinically relevant. In conclusion, this review showed no conclusive evidence for the treatment of Rockwood type III AC dislocations. Physically active young adults seem to have a slight advantage in outcome when treated operatively. 10
Therefore, we conducted a survey among upper limb surgeons in the United Kingdom to review commonly accepted practise.
Materials and methods
A questionnaire was made and six questions were asked.
Questions asked are as follows. Do you recommend stress view for diagnosis? When do you treat surgically? When do you do surgery? Preferred method of stabilization Do you do excision of lateral end of clavicle? Rehabilitation
Grade 3 AC joint disruption: Survey of opinion of shoulder consultants in the United Kingdom
Questionnaire
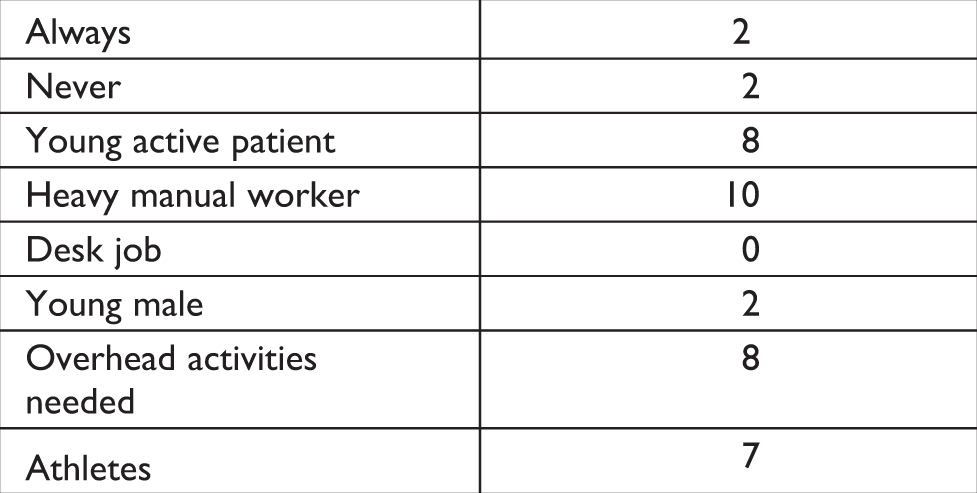
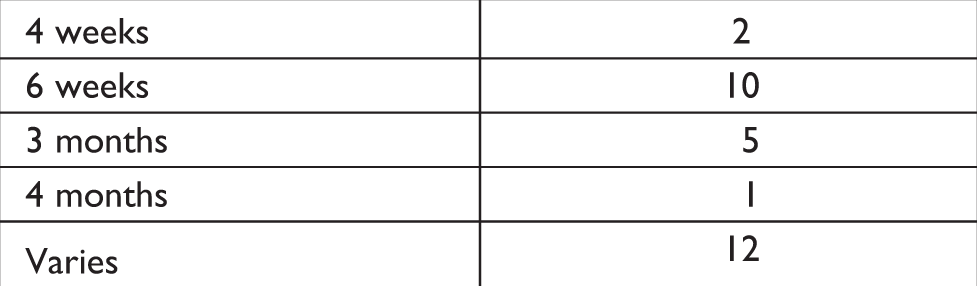
Do you recommend stress view for diagnosis? Always Never Sometimes When do you treat surgically? Always Never Young active patient Heavy manual worker Desk job Young male Overhead activities needed Athletes Other indications -------- When do you do surgery? ASAP Within 3 weeks Within 6 weeks Other -------- Preferred method of stabilization Surgilig Tightrope Modified Weaver Dunn K wires Screws Other -------- Do you do excision of lateral end of clavicle? Always Never Sometimes Rehabilitation Immobilize for -------- weeks Overhead activities allowed after -------- weeks Sports after -------- weeks/ months Other --------
Results
Do you recommend stress views for diagnosis?

If chronically symptomatic after conservative treatment for 6/12,
After full and frank discussion,
Failure to progress with non-operative treatment, women,
Only rarely even then, if the patient is symptomatic of scapular instability, persisting pain/discomfort at rest or activity related,
Discuss with these patients, when conservative Rx fails, if still problematic after 3–4 months,
If symptomatic at 3 months,
Down to patient to decide,
If anterior deltoid origin clinically ruptured,
Do you mean acutely or delayed – not clear.
Answer = rarely acutely, if still symptomatic after 6 weeks,
Regardless of patient characteristics if they remain symptomatic, depends on degree of clinical displacement and patient needs, women.

After 6/12, or before if patient chooses, as required,
When the external skin wound, if any, has healed, usually after 6 weeks,
Within 4 weeks, as above,
After 3–4 months or ASAP if associated fracture,
3 months,
If symptomatic after 1 year,
Most cases late,
After trial of conservative Rx unless deltoid origin ruptured, rarely acutely,
Any time, 6 weeks onwards.

LARS for chronic, Surgilig for acute,
Dog bone, combination or tightrope on its own,
Hook plate,
Twin-tail tightrope, combination, defined by the pathology of the injury – which varies, or dog bone,
LARS ligament,
Hook plate,
Hook plate, with neo-ligament sleeve round coracoid,
LARS ligament or hamstrings,
LARS ligament.
For many years I did the Weaver Dunn but the requirement to remove the screw plus the failure rate mainly in non-compliant young men forced me to change to hook plate.



Discussion
The results of our survey truly reflect the controversy regarding appropriateness of any single treatment of grade 3 AC joint dislocations. These are injuries, which are commonest in males in the second or third decade, with the incidence steadily declining with age thereafter. 6
Only 2 surgeons always asked for stress view, 13 did sometimes but majority of surgeons never did stress view. This reflects the findings of Bossart et al. He found that in only three cases (4%) did weights cause the injured Coracoclavicular (CC) distance to increase and thereby unmask a grade 3 injury not evident on plain films. Further evidence that weights may not reliably elucidate the degree of AC joint injury is suggested by the fact that in several cases the weights actually caused the injured and uninjured CC distance to decrease. They concluded that the use of weighted radiographs lacked efficacy in unmasking grade 3 AC sprains on radiograph and recommended not to use this technique routinely. 11
In our series, only two surgeons always treated these injuries surgically and most surgeons showed preference mainly according to demands on shoulder. Most surgeons favoured surgery only if needed but not first choice. Nissen and colleagues surveyed 577 American Orthopaedic Society for Sports Medicine members, and 81% indicated they preferred non-operative treatment for uncomplicated type 3 injuries. When performing surgery for type 3 injuries, 69% recommended reconstruction of the coraco-clavicular ligaments. 12
This opinion is further supported by the survey of McFarland et al. McFarland and co-workers surveyed 42 orthopaedic surgeons who were team physicians for major league baseball athletes with type 3 AC joint injuries. The survey presented a hypothetical scenario of a starting pitcher who sustained a grade 3 AC joint injury. Among the physicians, 69% stated they would treat non-operatively and 31% operatively. There were 25 physicians who had actually treated a pitcher with a type 3 injury in the throwing arm. They reported that among the non-operative patients, 80% had normal function, no pain, and 90% return of normal range of motion. 13
There is no consensus on timing of surgery. Majority 6 of surgeons preferred to do operation within 3 weeks and with six surgeons as soon as possible. But only one surgeon showed willingness to do it within 6 weeks. In the study of Angelo et al., the mean interval between injury and operation was 7 days (range 0–15 days). 14
There are many fixation options available for AC joint dislocation and we found that surgeon’s preferences were quiet wide for choosing fixation method. But Surgilig, Tightrope and Weaver Dunn were among widely used methods in our questionnaire.
It clearly reflects paucity of good randomized controlled trial’s in literature to compare results of different fixations. Jong et al. results showed that internal fixation using a hook plate and synthetic ligament reconstruction yielded comparable clinical results in patients with acute unstable dislocation of the AC joint. 15
There is conflicting evidence in literature for treatment options and ideal fixation device for these injuries. That is also evident from this questionnaire as there is no consensus in orthopaedic surgeons for ideal treatment of type 3 AC joint dislocations. We think that good RCT can only be able to solve this puzzle, which unfortunately is not available till now.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.