
Abstract
Background:
In recent years, there has been a trend toward more aggressive management of slipped capital femoral epiphysis (SCFE) with acute anatomical realignment; however, the literature is unclear with regard to the indications for this.
Questions/purposes:
To collect long-term patient-reported outcome scores on a group of SCFE patients using modern hip scores. The second aim was to determine whether there is a threshold level of deformity beyond which patients have predictably poor outcomes following in situ pinning.
Patients and methods:
Patients presenting with SCFE between 2000 and 2009 completed a survey consisting of three modern hip scores and were classified into poor, intermediate, and good outcome groups. The posterior slope angle (PSA) was used to measure slip deformity. We examined the relationship between patient characteristics and functional outcomes. The relationship between PSA score and overall outcome was examined using receiver operator curve (ROC) analysis.
Results:
The total study population was 63; 14% patients had poor, 29% had intermediate, and 57% had good functional outcomes. The mean Non-Arthritic Hip Scores (NAHSs) for those with poor outcomes was 51, 76 in the intermediate group, and 95 in the good group (p <0.001). PSA was significantly lower in those with good functional outcomes. ROC analysis demonstrated that a higher PSA was moderately predictive of a poor clinical outcome (area under the curve of 0.668). In both the poor and intermediate outcome groups, 50% of patients had a PSA of 40° or greater, whereas only 31% of those with good clinical outcomes had PSA of 40° or greater.
Conclusions:
A significant proportion of post-SCFE patients have ongoing suboptimal hip function after pinning in situ. Those with a PSA more than 40° have a higher chance of a poor outcome.
Introduction
Slipped capital femoral epiphysis (SCFE) is a condition affecting adolescent patients with the potential to significantly affect their quality of life (QOL) dependent on the degree of residual deformity resulting in subsequent pain and impairment in hip function. SCFE has traditionally been managed with in situ pinning, a safe, and reliable treatment, 1,2 with attempts to perform an acute closed reduction having poor results. 1,3 This results in a nonanatomical position of the epiphysis. In recent years, there has been a trend toward more aggressive management with acute anatomical correction being advocated by a number of surgeons with different techniques. 4 –9 This includes the modified Dunn technique developed by Ganz et al. 9–10 using a surgical hip dislocation through a trochanteric osteotomy. 11 They have shown good-to-excellent short-term outcomes 4 with normalization of anatomy and range of motion post-operatively. 11 However, this is a technically challenging procedure with a significant learning curve and the avascular necrosis (AVN) rates that have been quoted show significant variation. Experienced centers report AVN rates of 0%, 5,12,9 Madan et al. reported an AVN rate of 7.1% in a series of 28 patients, 13 whereas other centers have reported AVN rates up to 26%. 6,14 Difficulty replicating the excellent outcomes 14 has resulted in decreased enthusiasm for the procedure which is unforgiving if the technique is not adhered to meticulously. 10
Modern hip scores are designed to provide a more detailed analysis of hip function than arthritic scores, such as The Harris Hip score, which have been used previously in the SCFE literature. 15,16 The Non-Arthritic Hip Score (NAHS), the Copenhagen Hip and Groin Outcome Score (HAGOS), and the Hip Disability and Osteoarthritis Outcome Score (HOOS) have been validated in young adult hip literature 17,18 and reflect hip function rather than arthritic change and the need for total hip replacement. This is important in the post-SCFE population who may be functionally impaired without having symptoms severe enough to warrant arthroplasty. The aim of this retrospective cohort study was to collect long-term patient reported outcome measures (PROMs) on a group of SCFE patients using modern hip scores to improve our understanding of patient’s perceptions of post-SCFE outcomes. The secondary aim was to determine whether there is a threshold level of deformity beyond which patients have predictably poor outcomes following in situ pinning.
Patients and methods
A total of 132 patients were seen and treated with SCFE between 2000 and 2009—a group previously described by Phillips et al. 19 Hospital records, the electoral roll of registered voters in New Zealand, and primary care information were utilized to contact the patients; 92 patients were able to be located, there were 23 nonresponders and 6 people declined to participate leaving a total of 63 who completed the survey (69%). Patients were contacted on multiple occasions with a total time of 6 months allowed for response. This left a total study population of 63 with a mean follow-up of 9.4 years (4.6–14.5, Table 1). Five cases (8%) were unstable, there were no cases of AVN and two patients had bilateral SCFE. This study was approved by the Northern B Health and Disability Ethics Committee of New Zealand. Informed consent was obtained from each participant prior to questionnaire completion.
Demographic characteristics of study population.

PSA: posterior slope angle.
Patients were asked to complete a Web-based survey through Survey Monkey (Palo Alto, USA) consisting of questions from the NAHS, HAGOS, and HOOS. Patients were offered the option of a paper-based postal questionnaire if they preferred or did not have access to a computer or the Internet. The survey responses were scored as per the instructions of each score to give an overall score for the NAHS and subgroup scores for the HAGOS and HOOS. 20,21 The posterior sloping angle (PSA) was used as the measure of slip deformity. 22 This was measured on the preoperative frog leg lateral X-ray (Figure 1) as described by Barrios et al. 23

Technique used to measure the PSA. The figure represents the X-ray of an 11-year-old girl with a left slipped capital femoral epiphysis showing the technique used to measure the posterior slope angle. A line from the centre of the femoral shaft through the center of the metaphysis represents the axis of the femur (A). A second line (B) is drawn from one edge of the physis to the other, representing the angle of the physis. Where lines A and B intersect, a third line (C) is drawn perpendicular to line A. The PSA is the angle formed by lines B and c as illustrated. PSA: posterior slope angle.
Inclusion criteria were SCFE managed with in situ pinning and a complete data set available for review including imaging. Patients were excluded if they had developed AVN. Patients with unstable SCFE who had not developed AVN were felt to be comparable in terms of outcome to patients with stable SCFE and so were included in the analysis. Patients who had undergone screw removal were included in the analysis as screw removal should not alter the residual deformity. Data collected included demographic data, stability (as defined by Loder et al. 24 ), and PSA (measured by author PP who was blinded to the outcome scores at the time of measurement).
The NAHS is a reliable and validated self-administered hip score designed for use in younger patients with higher demands and expectations than older patients with degenerative joint disease. 17 It was analysed as a cumulative total score. The HAGOS score is a validated and responsive score consisting of six separate subscales assessing pain, symptoms, function in activities of daily living, sport, participation in physical activities, and QOL (pain, symptoms, ADL, sport, participation, and QOL). It measures symptoms, activity limitations, participation restrictions, and QOL in physically active patients with groin pain. In each domain, a score between 0 and 100 is generated, with 0 corresponding to the lowest level of function and 100 the highest. Scores of 75–100 in each domain were considered to indicate a good functional outcome, scores of 40–74 an intermediate outcome, and scores <40 a poor functional outcome.
The HOOS is a similar score with five subscales (pain, symptoms, ADL, sport, and QOL) and has been shown to be particularly responsive is patients under 66 years of age. 18 Similar to HAGOS, each HOOS domain has a score between 0 and 100, and scores of 75–100 in each domain were considered to indicate a good functional outcome, scores of 40–74 an intermediate outcome, and scores <40 a poor functional outcome. The average functional outcome for each domain across the two schemes was calculated, with the HAGOS categories of sport and participation combined to correlate with the HOOS sport domain. Subjects who had good functional outcomes in three or more categories and no poor functional outcomes were considered to have a good outcome overall. Subjects with three intermediate outcomes or one poor outcome and no more than one intermediate outcome were considered to have an intermediate outcome, and subjects with more than one poor outcome or one poor outcome and more than one intermediate outcome were considered to have a poor outcome overall.
We examined the relationship between continuous variables and the functional outcomes using analysis of variance (ANOVA) and categorical variables and outcomes using χ2 tests. The relationship between PSA score and overall outcome was also examined using receiver operator curve (ROC) analysis. All statistical tests were performed using SPSS 20.0 (IBM, Armonk, NY, USA), and p values <0.05 were considered statistically significant.
Results
In terms of outcomes from the scores of HAGOS and HOOS (Table 2, Figure 2), 2 of 63 (3%) had significant ongoing issues with respect to pain, 12 of 63 (19%) had moderate ongoing pain issues, and 49 of 63 (78%) had little or no ongoing pain issues. Symptoms were a significant ongoing concern for 6 of 63 (9%), 20 of 63 (32%) had moderate symptoms, and 37 of 63 (59%) had few or no ongoing symptoms. Activities of daily living were significantly impacted for 3 of 63 (5%), moderately impacted for 13 of 63 (21%), and 47 of 63 (75%) had few or no ongoing limitations. Sports and participation in physical activities were significantly limited for 15 of 63 (24%), moderately limited for 11 of 63 (17%), and little or not limited for 37 of 63 (58%). QOL was significantly impaired for 7 of 63 (11%) and moderately impaired for 20 of 63 (32%). If we then combine these and say that if you have two or more areas of significant concern you have poor outcomes, at least two areas of intermediate concern or one significant concern you have an intermediate outcome, and one or less intermediate concerns a good outcome, then 9 (14%) patients had poor, 18 (29%) had intermediate, and 36 (57%) had good functional outcomes.
Mean PROM scores and subscore analysis for HAGOS and HOOS.
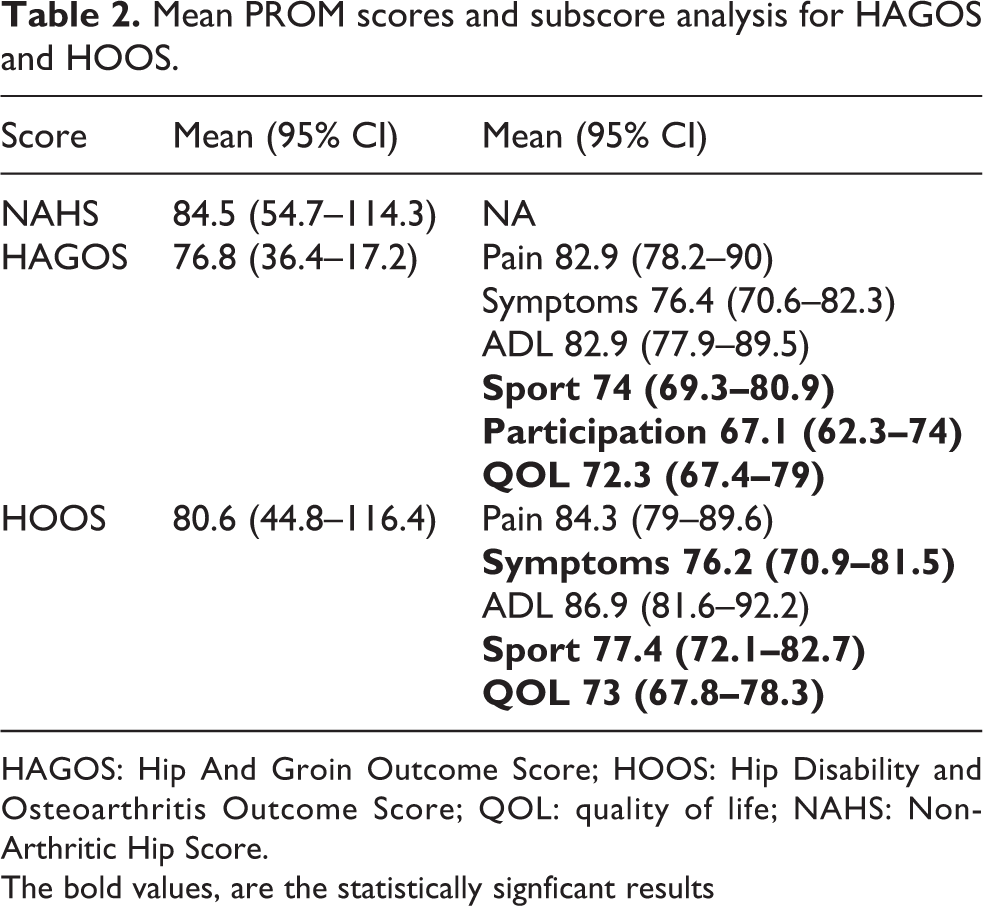
HAGOS: Hip And Groin Outcome Score; HOOS: Hip Disability and Osteoarthritis Outcome Score; QOL: quality of life; NAHS: Non-Arthritic Hip Score.
The bold values, are the statistically signficant results

Domain subscores for HAGOS and HOOS in poor, intermediate, and good outcome groups. HAGOS: Hip and Groin Outcome Score; HOOS: Hip Disability and Osteoarthritis Outcome Score; QOL: quality of life.
The mean NAHS scores for those with poor outcomes was 51 (20–70), compared to 76 (56–86) in the intermediate group, and 95 (81–100) in the good functional group (p < 0.001, ANOVA). Poor functional outcomes were not related to age at presentation, ethnicity, sex, length of follow-up, or whether the SCFE was stable or unstable at presentation.
PSA was significantly lower in those with good functional outcomes (mean 32.9°, 8–70°) compared to those with intermediate (mean 41.3°, 18–66°) or poor outcomes (mean 42.2°, 24–81°, p = 0.03). Consistent with this, ROC analysis demonstrated that a higher PSA was moderately predictive of a poor clinical outcome, with an area under the curve of 0.668 (95% CI 0.535–0.801, p = 0.023; Figure 3). In both the poor and intermediate outcome groups, 50% of patients had a PSA of 40° or greater, while only 31% of those with good clinical outcomes had PSA of 40° or greater.

ROC analysis of outcome group versus PSA at presentation. PSA: posterior slope angle; ROC: receiver operator curve.
Discussion
It is known that patients with SCFE are likely to need total hip arthroplasty (THA) sooner, with 45% of SCFE patients needing THA by age 50. 25 These patients are believed to have accelerated joint degeneration due to residual deformity, AVN, and chondrolysis. 25 A study by Ziebarth et al. showed that 89% of SCFE patients had acteabular cartilage damage at the time of the slip, the severity of which was not related to the higher slip angles. 26 Patients with SCFE deformities develop cam lesions that alter the normal biomechanics of the hip resulting in impingement type pain. 27 Suboptimal hip function prior to the onset of osteoarthritis is believed to be secondary to impingement and thus has similar symptomatology to patients with femoral acetabular impingement (FAI). However, the extent of remodeling post-SCFE is unknown and may explain why some patients with severe slips and deformity do well functionally following in situ pinning. Increasing recognition of the functional impairment associated with FAI has led to reassessment of the goals in the treatment of SCFE where the risks associated with more complex and invasive procedures may be justifiable to obtain superior functional outcomes. 11
PROMs are lacking in the SCFE literature. In recent publications, Poorter et al. 28 and Escott et al. 29 looked at long-term outcomes in these patients but have come to different conclusions regarding the relationship of slip severity and outcome. This article builds on the aforementioned two, to provide more information to aid surgical decision-making and improve our understanding of the difficulties post-SCFE patients’ experience. In our cohort, just over half (57%) of patients had a good functional outcome. A small group (14%) had poor outcomes and a reasonably sized group (29%) had intermediate outcomes. The intermediate group reported ongoing concerns with pain, symptoms, and activities of daily living, which reflects the fact that patients post-SCFE do not have “normal” hip function. The NAHS scores were lower in those with poorer outcomes as assessed by the HAGOS and HOOS scores, with a good correlation across the three scores. We found that a lower PSA at presentation was a modest predictor of good functional outcomes. Therefore, PSA as a measure of slip severity is related to the long-term outcome, although there are undoubtedly other factors that influence hip function such as remodeling and chondrolysis. In addition, Escott et al. 29 showed that poorer outcomes were related to increased body mass index (BMI).
The long-term outcome of SCFE managed with in situ pinning has previously been considered acceptable with Boyer reporting excellent outcomes in a group of 121 patients in 1981 using the Iowa hip rating 1 and Castaneda also reporting good outcome scores with the Harris hip score at 20 years of follow-up. However, they reported a high rate of pistol-grip deformity which correlates with the presence of osteoarthritis (OA) in early adulthood. 30 Carney et al. reported follow-up of 182 hips for 41 years using the Iowa hip rating and concluded that the natural history of mild slips was favourable. 15 These data are difficult to extrapolate to our current patients, who may have higher expectations of what constitutes “acceptable” hip function. These papers utilize older surgical techniques that are not currently employed and arthritic hip scores rather than modern PROMs. FAI, and the associated symptom complex, is an increasingly recognized consequence of post-SCFE deformity. 31 Scores such as the NAHS, HOOS, and HAGOS are able to assess hip function from the patient’s perspective in more detail than the arthritic hip scores. 32,20,21
Two other studies have looked at this cohort using modern PROMs. Escott et al. 29 reported on the long-term health status and QOL in a group of 64 patients at a mean follow-up of 19.4 years. They concluded that these patients had lower University of California at Los Angeles (UCLA) activity scores with higher rates of diabetes and mortality than the general population. In their study, post-SCFE patients were at a high risk of weight gain, which was associated with a poorer outcome. They concluded that there was no association between higher slip angle and poor outcome. Poorter et al. 28 looked more specifically at hip function in a group of 61 patients with a mean follow-up of 18.4 years. Their cohort reported lower scores for QOL and sports activities. They concluded that there was a correlation between slip severity and outcome. Mild-to-moderate slips had a good outcome, and they concluded that there was no indication for open realignment procedures in these patients. Our study agrees with the Poorter paper in that we have found a relationship between slip severity and hip function, although as the Escott paper alludes to, there are likely to be other factors that influence the overall outcome for individual patients. We found no association between PROMs and gender which differs from the findings of Escott et al.
This study along with the papers by Poorter and Escott provide clinicians with enhanced detail and knowledge regarding long-term outcomes after in situ pinning of SCFE. The literature is beginning to clarify the indications for realignment procedures. From our data, a PSA above 40° is associated with a higher chance of poor functional outcome and the risks of primary anatomical realignment may be acceptable in this group. As shown by the ROC analysis, a firm threshold level of deformity is not present above which hip function clearly declines. The data also show that some patients with large PSAs do well, which adds evidence to the theory that proximal femoral remodeling occurs post-SCFE. Remodeling potential is thought to be higher with mild slips and relative skeletal immaturity. 33 The results of the article can be compared in future to the long-term outcomes of realignment procedures once these are available.
Weaknesses of this study include a relatively high loss to follow-up. This is a notoriously difficult population to follow which is very mobile with low socioeconomic status. This cohort represents a relatively large group in comparison to other SCFE papers in the literature. Follow-up in this study is comparable to the study by Poorter et al. 28 (67%) and higher than Escott et al. 29 (32%). It is difficult to know which group the nonresponders would fall into and whether they would sway the outcome data. Current radiological and clinical examination findings would be of interest to assess the effect of remodeling and the relationship between PROMs and objective measurements. This is something we endeavor to achieve in the future with this cohort. BMI has been shown to impact outcome, and because of the retrospective nature of the study, we did not have these data available for all patients at the time of presentation. Similarly, we did not collect data on the current height and weight of the patients.
Conclusion
A significant proportion of post-SCFE patients have ongoing suboptimal hip function after pinning in situ, and there is a relationship between slip severity and long-term hip function. Those with a PSA over 40° have a higher chance of a poor outcome, although other factors undoubtedly play a role in the overall hip function and QOL. The risks of primary anatomical realignment may be acceptable in some patients; however, the decision to proceed with acute realignment surgery requires discussion with patients and family on a case-by-case basis.
Footnotes
Authors’ note
The present study was conducted at Waikato Hospital, Pembroke St, Hamilton, New Zealand.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.