
Abstract
Introduction:
Medial patellofemoral ligament reconstruction (MPFLR) is regularly combined with a tibial tuberosity transfer (TTT) in cases of recurrent patellar instability with underlying structural deformity. However, these indications for a TTT have recently come into question. This study aimed to assess the traditional indications by comparing the outcomes of isolated and combined MPFLR for the treatment of recurrent lateral patellar dislocation.
Methods:
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Included studies were those which reported the outcomes of either isolated or combined or both MPFLR. Studies were required to report at least one of the following: redislocation rate, revision due to instability, or the Kujala score.
Results:
We found no difference between isolated and combined MPFLR in terms of redislocation (p = 0.48), revisions due to instability (p = 0.36), positive apprehension tests (p = 0.25), or the Kujala score (p = 0.58). Combined reconstruction presented more complications compared to isolated procedures (p = 0.05). Subgroup analysis revealed no significant difference between studies investigating isolated medial patellofemoral ligament reconstruction MPFLR performed in patients with normal tibial tuberosity–trochlear groove (TT-TG) distances only or in patients with both normal and elevated TT-TG distances.
Conclusions:
According to the published data, there is no difference in outcomes between isolated and combined MPFLR. Underlying structural deformity did not demonstrate any significant effect on the success of the isolated MPFLR. Although there are definite indications for combined reconstruction, the current evidence suggests that our inclusion criteria may not be entirely correct. Further study is required to clarify and refine the true indications for combined MPFLR.
Level of Evidence:
III, meta-analysis of nonrandomized studies.
Introduction
Recurrent patellar dislocation is a disabling condition commonly occurring in healthy, young, and active patients. Biomechanical studies have identified the medial patellofemoral ligament (MPFL) as the primary medial stabilizer of the patella, contributing up to 60% of the restraining force to prevent lateral dislocation. 1,2 Treatment options range from conservative measures to surgical procedures aimed at restoring the function and restraining force of the MPFL, such as the MPFL reconstruction (MPFLR), plication of the MPFL, or bony procedures such as the tibial tuberosity transfer (TTT). 3
Recurrent patellar dislocation is often associated with abnormal bony anatomy, particularly the position of the tibial tuberosity. This deformity manifests as an increased quadriceps (Q) angle or tibial tuberosity to trochlear groove (TT-TG) distance in cases of excessive lateralization. The Q-angle is an index of the lateralization of the tibial tubercle, measured clinically using a goniometer to measure the angle formed by the anterior superior iliac spine, center of the patella, and the tibial tubercle. 4 Earlier biomechanical studies have demonstrated that elevated Q-angles predispose patients to anterior knee pain, as well as increased instability through increased patellofemoral contact pressures. 5 However, the reported reliability of the Q-angle is variable 6 –8 and in many cases poor, with intraclass observer correlations reported as low as 0.14. 7 The Q-angle has been superseded by more reliable radiographic indices of tibial tubercle lateralization, such as the TT-TG distance.
The TT-TG distance is a radiographic measurement made using the computed tomography or magnetic resonance modalities to measure the lateral position of the patella tendon insertion on the tibia with regard to the trochlea groove, quantifying the lateral forces on the patella with Q contraction. Normal TT-TG distance is defined between 10 mm and 15 mm, with 20 mm normally set as the threshold for an increased risk of lateral patellofemoral instability. 9 Studies have shown that TT-TG in excess of these values confers an increased risk of recurrent lateral patellar instability following MPFLR. 10,11 Several authors have reported using MPFLR supplemented with bony procedures such as TTT to restore normal bony anatomy and therefore decrease the risk of recurrence in these cases of increased TT-TG distances. 12 –14 Patella alta can also confer an increased risk of instability (defined as an Insall–Salvati ratio above 1.7), 15 and it has been suggested that patients with this deformity also receive a TTT.
Recently, the need to perform concurrent TTT in patients with increased TT-TG distance undergoing MPFLR has been questioned. Several studies have reported no significant difference in recurrent instability or patient-reported outcome measures (PROMs) scores between patients with normal and elevated TT-TG treated with isolated MPFLR alone. 16 –18
Previously published reviews addressing MPFLR have investigated return-to-sport and activity, 19 common complications, 20 and risk factors for recurrent instability following MPFLR. 21 However, no such review has compared the outcomes of isolated MPFLR against MPFLR procedures combined with TTT.
Thus, we sought to systematically review the current literature to compare the reported outcomes of isolated MPFLR procedures against MPFLR combined with TTTs. We hypothesize that the difference between the two procedures will be nonsignificant, in accordance with the recent findings.
Methods
Literature search strategy
The present systematic review was a meta-analysis conducted according to the international Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 22,23 Electronic searches were performed using Ovid Medline, PubMed, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, ACP Journal Club, and Database of Abstracts of Review of Effectiveness during November 2015. Searches in these databases were carried out in accordance with Cochrane Collaboration, PRISMA guidelines. 24 To achieve the maximum sensitivity of the search strategy, we combined the terms medial patellofemoral ligament and reconstruction with their associated synonyms as either keywords or Medical Subject Headings terms. The reference lists of all retrieved articles were reviewed for further identification of potentially relevant studies and assessed using the inclusion and exclusion criteria.
Selection criteria
Eligible studies for this systematic review included English language studies published at any time which reported the outcomes of isolated MPFLR or MPFLR combined with TTT, or both. Included studies were required to report at least one outcome out of redislocation, revision due to redislocation, or patient-reported outcomes (the Kujala score) at the follow-up. Recurrence was defined in this review as any reported dislocation following surgery. If reported, positive apprehension tests were also recorded. Revision was reported as any repair following the primary survey due to recurrent instability. Only original data studies published at any time were used. Abstracts, case reports, conference presentations, editorials, reviews, and expert opinions were excluded. Studies with both isolated and combined procedures that did not clearly define the outcomes for these populations separately were excluded.
Because quality scoring is controversial in meta-analyses of observational studies, two reviewers independently appraised each article and met consensus on any disagreements on inclusion or exclusion. Strengthening the Reporting of Observational Studies in Epidemiology checklist was used to evaluate the structure of the studies. 25 An expert knee orthopedic surgeon was also consulted regarding the included references.
Data extraction
Data were extracted from the text, tables, and figures of all the included studies.
Statistical analysis
Relative risk was used as a summary statistic. In the present study, both fixed- and random-effects models were tested. In the fixed-effects model, it was assumed that treatment effect in each study was the same, whereas in a random-effects model, it was assumed that there were variations between studies. χ2 tests were used to study heterogeneity between trials. I 2 statistic was used to estimate the percentage of total variation across studies, owing to heterogeneity rather than chance, with values greater than 50% considered as substantial heterogeneity. I 2 can be calculated as follows: I 2 = 100% × (Q − df)/Q, with Q defined as Cochrane’s heterogeneity statistics and df defined as the degree of freedom. If there was substantial heterogeneity, the possible clinical and methodological reasons for this were explored qualitatively. In the present meta-analysis, the results using the random-effects model were presented to take into account the possible clinical diversity and methodological variation between studies. Specific analyses considering confounding factors were not possible because raw data were not available. All p-values were two-sided.
Results
Search results and paper quality
The search yielded 401 results. Following abstract and full-text screening, 38 studies were kept which pertained to the inclusion and exclusion criteria. Of these, 31 studies addressed isolated MPFLR, 3,16 –18,26 –52 three addressed combined MPFLR, 53 –55 and four papers addressed both. 12,13,56,57 Of the papers investigating isolated MPFLR, three studies did not impose any exclusion for patients with an elevated TT-TG distance or Q-angle, while the other 28 did. The studies were of limited quality, 33 scoring a level IV and 5 scoring a Level II on the National Health and Medical Research Council’s levels of evidence. The results of the search process are summarized in Figure 1.

Outline of the sequential inclusion and exclusion of studies from this systematic review.
Demographics
A total of 1422 knees were extracted from the included studies in this article. Of these, 1307 were isolated procedures, and 115 were combined procedures. The patient populations and surgical details of each included study are summarized in Appendix 1.
The summarized results of subgroup analysis comparing isolated or combined procedures and studies which used TT-TG/Q-angle as an exclusion criterion and those that did not are shown in Tables 1 and 2, respectively.
Meta-analysis of the outcomes following MPFLR when comparing isolated and combined procedures.

MPFLR: medial patellofemoral ligament reconstruction; CI: confidence interval; PROMs: patient-reported outcome measures.
Meta-analysis of the outcomes following MPFLR when comparing studies that used TT-TG/Q-angle as a criterion for exclusion and those that did not.
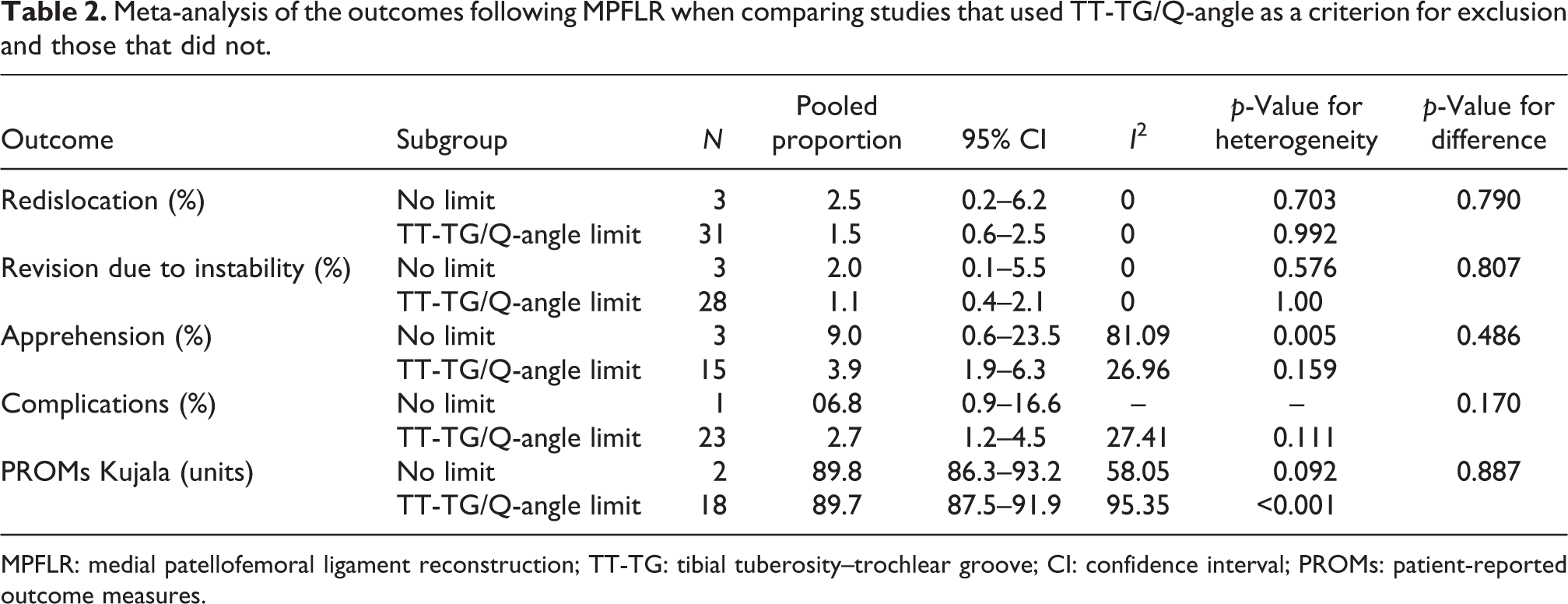
MPFLR: medial patellofemoral ligament reconstruction; TT-TG: tibial tuberosity–trochlear groove; CI: confidence interval; PROMs: patient-reported outcome measures.
Redislocation
Redislocation was reported as an outcome in 38 papers, with a total of 1268 isolated patients and 95 combined patients. Their respective rates of redislocation in isolated and combined patients were 1.4% (I 2 = 0%, p = 0.99) and 1.1% (I 2 = 0%, p = 0.81), with no significant heterogeneity detected in the literature. There was no significant difference between the two rates (p = 0.48). The subgroup analysis of papers investigating isolated MPFLR performed in patients with a nonelevated Q-angle or TT-TG only (n = 1029) versus papers in which isolated MPFLR was performed irrespective of Q-angle or TT-TG (n = 133) demonstrated a significant difference in terms of redislocation, with rates of 1.5% (I 2 = 0%, p = 0.992) and 2.5% (I 2 = 0%, p = 0.703), respectively (p = 0.79), with no significant heterogeneity detected.
Revision due to instability
Revision due to instability was reported as an outcome in 30 papers, with a total of 1083 isolated patients and 25 combined patients. The respective rates of revision due to instability were 1.2% (I 2 = 0%, p = 1.00) and 2.3% (I 2 = 0%, p = 0.52), with no significant heterogeneity reported. There was no statistically significant difference between isolated and combined procedures in terms of revision rate (p = 0.36). The subgroup analysis of papers investigating isolated MPFLR performed in patients with low Q-angle or TT-TG only (n = 950) versus papers which did not use Q-angle or TT-TG (n = 133) as a contraindication showed no significant heterogeneity or significant difference in terms of revision, with rates of 1.1% (I 2 = 0%, p = 1.00) and 2.0% (I 2 = 0%, p = 0.576), respectively (p = 0.81).
Apprehension test
Positive apprehension test was reported as an outcome in 22 papers, in a total of 698 isolated patients and 55 combined patients. The respective incidences for positive apprehension tests were 5.1% (I 2 = 54.2%, p = 0.003) and 8.5% (I 2 = 27.0%, p = 0.25), with significant heterogeneity detected in the isolated cohort. There was no statistically significant difference between isolated and combined procedures in terms of positive apprehension test incidences (p = 0.41). The subgroup analysis of papers investigating isolated MPFLR performed in patients with low Q-angle or TT-TG only (n = 558) versus papers which did not use Q-angle or TT-TG (n = 133) as a contraindication showed no significant difference in the rates of positive apprehension test, with rates of 3.9% (I 2 = 27.0%, p = 0.159) and 9.0% (I 2 = 81.1%, p = 0.005), respectively (p = 0.49). However, significant heterogeneity was detected in studies with no limit to Q-angle or TT-TG.
Patient-reported outcomes (the Kujala score)
Patient-reported outcomes were reported using the Kujala score in 23 papers, in a total of 698 isolated patients and 55 combined patients. The respective mean Kujala scores were 88.8 (I 2 = 95.1%, p < 0.001) and 86.5 (I 2 = 92.2%, p < 0.001), with significant heterogeneity detected in both cohorts. There was no statistically significant difference between isolated and combined procedures in terms of the Kujala score (p = 0.578).
Complications
Twenty-seven papers reported complications requiring reoperation as an outcome, in a total of 842 patients receiving isolated MPFLR and 51 patients receiving combined MPFLR procedures. The respective rates of complication were 2.8% (I 2 = 23.8%, p = 0.141) and 10.2% (I 2 = 0%, p = 0.482). Combined procedures demonstrated a statistically significantly higher rate of complication compared to isolated procedures (p = 0.05). The most common cause of complication in the isolated cohort was patellar fracture in the postoperative period due to trauma sustained to the knee, while combined procedures were most commonly complicated by the reduced range of motion requiring manipulation under anesthetic.
Discussion
The goal of patellar stabilization surgery was to confer stability to the patellofemoral joint while improving patient pain and confidence to allow for return to function. Recent evidence has demonstrated that surgery is superior to nonsurgical measures by reducing redislocation rates postoperatively. 58,59 The decision to supplement the MPFLR with adjunct procedures such as TTT remains a topic of debate, particularly in the context of patients with an increased Q-angle or TT-TG distance. The meta-analysis of the previously published studies found that there is no significant difference in redislocation, revision rates, or the incidence of positive apprehension tests between isolated MPFLRs and those supplemented with TTT. There was also no significant difference between the two in terms of the postoperative Kujala score. However, MPFLR with TTT conferred a significantly greater risk of postoperative complication requiring reoperation when compared to isolated MPFLR. There was no heterogeneity detected in any of the above findings, except with regard to the PROMs score, suggesting that the findings of the included studies were in agreement with each other and are reliable. The results of this meta-analysis suggest that while there are definitely particular indications for a TTT in MPFLR, the current criteria may not be entirely correct due to a lack of difference in outcomes between combined and isolated procedures.
The pooled rate of redislocation reported in this study (1.1% for isolated MPFLR and 1.4% for combined MPFLR) is lower than the rate of 3.7% published in a systematic review by Shah et al. 20 This discrepancy is most likely due to the fact that Shah et al. included subluxations in their analysis with dislocations. It follows that supplementing MPFLR with TTT would superimpose the inherent complication risks (reported at up to 5.9% 60 ) associated with the bony procedure on this baseline rate of complication.
Avoiding performing an additional TTT in patients with elevated Q-angle or TT-TG could be advantageous as it would decrease the risk of complication, while also theoretically decreasing operative time. The postoperative recovery would be faster after MPFLR without the need for a period of non-weight-bearing, faster return to preinjury function and without the need for hardware removal, which is common after a TTT. 60,61
TTT will result in altered load distribution across the patella. In some cases, this could be advantageous and indeed an indication for the procedure. In other cases, however, it can be a drawback. The two most common tubercle realignment procedures are the Elmslie–Trillat medialization and the Fulkerson anteromedialization procedures. As the Elmslie–Trillat can increase medial patella facet contact pressures by overmedializing the patella, it is not recommended in the presence of medial patellofemoral degenerative changes. 62,63 The Fulkerson anteromedialization tends to distribute contact pressures more evenly medially and proximally and to unload the lateral facet. Patients with arthrosis of the patella medially and proximally are less suitable for this type of procedure. Many patients complain of pain from the subcutaneous hardware and wish to have it removed once healing is complete. 61
Trochlear dysplasia is another bony deformity which may influence redislocation following MPFLR. Biomechanical studies have demonstrated that trochlear dysplasia creates a more lateral resting position of the patella when compared to a knee with normal bony anatomy, with a significant reduction in stability, 64 especially at 20 degrees of flexion. 65 Clinically, severe trochlear dysplasia (Dejour’s Grade C or D) has been identified in several case series as an independent risk factor for recurrence following MPFLR, 18,66 and therefore, it has been recommended by some authors that this subset of patients are treated with adjunct trochleoplasty or TTT. 67 Trochleoplasty is a challenging operation with potentially high complication rate and is rarely seen outside of Europe. 68 As it is the case for the TT-TG distance, the need for trochleoplasty has been called into question, with Steiner et al. reporting no redislocations and no effect of trochlear dysplasia on patient-reported outcomes when treated with isolated MPFLR. 50 Once again, as it is the case with the present study, the findings of these previous papers are limited by their low quality of evidence and small sample sizes and warrant further detailed investigation using randomized controlled trials. Trochlear dysplasia and its effects on the outcomes of this present study could not be adequately quantified, as the reporting of dysplasia in the included case series was inconsistent and thus could not be analyzed.
Like trochlear dysplasia, patella alta is a risk factor for the recurrent dislocation of the patellofemoral joint and is defined by radiographic indices such as an Insall–Salvati ratio of >1.7. 15 Due to the relatively high position of the patella with regard to the trochlear groove, the flexion of the knee joint results in a delayed engagement of the patella within the trochlear groove and contact with the lateral sulcus, during which there is no bony resistance against lateral displacement of the patella. 69 –71 This theoretical relationship has been verified, with patella alta as a confirmed risk factor for recurrent dislocation. 72 Similar to trochlear dysplasia, the proportion of patients with significant patella alta in this study could not be adequately analyzed due to inconsistent reporting and should be an issue of focus in future studies.
Limitations
The findings of this study should be interpreted in the light of the limitations of both the studies analyzed and the overall meta-analysis as a whole. First, due to the relatively low incidence of increased TT-TG or Q-angle, there was a much smaller number of patients in the combined group compared to the isolated group, which limits the sensitivity of the combined group in detecting outcomes. Additionally, the majority of studies investigating isolated MPFL used increased TT-TG distance as relative contraindications, which creates a selection bias, as in theory the patients in the isolated cohort would inherently be less likely to redislocate. Specifically, the patients selected for combined MPFLR could have elevated TT-TG distances or incidences of trochlear dysplasia or patella alta. The subgroup analysis, however, revealed no significant difference between isolated studies with and without TT-TG/Q-angle limitation, as well as no difference overall between isolated and combined MPFLR, suggesting that modification of the TT-TG/Q-angle may not be necessary, even in patients with increased distances. Furthermore, due to inconsistencies in reporting, the degree of trochlea dysplasia or patella alta could not be quantified. Patellofemoral instability is influenced by a large number of factors, which complicates our analysis. Other factors potentially affecting stability, such as ligamentous laxity, rotational profile, and patellar height, were unable to be considered in this review due to a lack of consistency of reporting in the literature and may have confounded our results. Additionally, in focusing on the TT-TG distance or the Q-angle as a surgical indication, this study did not assess the efficacy of MPFLR combined with trochleoplasty in the context of severe trochlear dysplasia, which has also been identified as a risk factor for recurrence. 18 However, as discussed above, the specific thresholds for when these deformities become significant remain unclear, and whether they require specific targeted treatment is also unclear. Nonetheless, the impact and management of trochlear dysplasia should be further investigated in future studies and subsequent systematic reviews. The validity of using the TT-TG distance or Q-angle as relative indications for additional bony procedures is limited by the inherent reliability of these measurements. Limitations in interobserver/intraobserver reliability has been demonstrated, with error reported at up to 1.81–3.2 mm. 73,74 It has also been demonstrated that TT-TG may be correlated with patient height 75 and individual joint size, 76 and therefore, the absolute distance must be interpreted in the context of variation in anthropometry.
It is recommended that isolated and combined MPFLR should be compared in future randomized controlled trials with patient cohorts matched in terms of TT-TG distance, trochlear dysplasia, and patella alta to better examine the differences between the two procedures. Furthermore, these patient cohorts should be matched for the degree of patella alta and trochlear dysplasia present.
Our systematic review suggests that the TT-TG/Q-angle alone may not be an absolute indication for an MPFLR supplemented with a TTT and need to be clarified and refined via future studies. Avoidance of the TTT procedure in select patients may also confer a lower risk of complications requiring reoperation. However, this issue requires further investigation in the form of high-quality comparative studies.
Conclusion
This meta-analysis found no significant difference in outcomes between isolated and combined MPFLR, except that combined MPFLR confers an increased risk of complication requiring reoperation. There was also no difference between studies investigating the efficacy of isolated MPFLR in patients with normal TT-TG distances or Q-angles only and patients with both normal and abnormal Q-angles or TT-TG distances. The results suggest that although there are definite indications for TTT in MPFLR, the current inclusion criteria may need to be further clarified. However, these conclusions are limited by the low quality of studies and the low number of cases involving combined MPFLR. Future studies should further compare isolated and combined MPFLR with prospectively collected data and appropriate randomization and blinding protocols.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix 1 Patient populations and surgical details of each included study

| Authors | Year | Isolated/combined/both procedures | TT-TG threshold | Design | LoE | MPFL technique |
|---|---|---|---|---|---|---|
| Cossey and Paterson 53 | 2005 | Combined | N/A | Retrospective case series | IV | Medial retinaculum graft |
| Deie et al. 30 | 2005 | Isolated | NR | Retrospective case series | IV | Semitendinosus autograft |
| Schottle et al. 30 | 2005 | Both | 15 | Retrospective case series | IV | Semitendinosus autograft |
| Mikashima et al. 45 | 2006 | Isolated | NR | Retrospective case series | IV | Semitendinosus autograft |
| Steiner et al. 50 | 2006 | Isolated | NR | Retrospective case series | IV | Adductor autograft |
| Christiansen et al. 56 | 2008 | Both | NR | Prospective case series | IV | Gracilis tendon autograft |
| Dopirak et al. 31 | 2008 | Isolated | NR | Retrospective case series | IV | Partial thickness quadriceps tendon autograft |
| Gomes 36 | 2008 | Isolated | NR | Controlled trial | II | Static and dynamic |
| Ronga et al. 48 | 2009 | Isolated | NR | Retrospective case series | IV | Hamstring tendon double-patellar tunnel |
| Matthews and Schranz 44 | 2010 | Isolated | 15 | Retrospective case series | IV | Semitendinosus autograft |
| Deie et al. 29 | 2011 | Isolated | NR | Retrospective case series | IV | Grafted semitendinosus tendon with bone plug |
| Han et al. 34 | 2011 | Isolated | NR | Prospective case series | IV | Double-tunnel semitendinosus tendon |
| Panni et al. 46 | 2011 | Isolated | 20 | Prospective case series | IV | Two-tunnel semitendinosus Autograft |
| Bitar et al. 3 | 2012 | Isolated | NR | Randomized controlled trial | II | Patellar tendon graft |
| Raghuveer and Mishra 47 | 2012 | Isolated | 20 | Retrospective case series | IV | Gracilis and semitendinosus autograft |
| Goyal 33 | 2013 | Isolated | NR | Retrospective case series | IV | Superficial quadriceps technique |
| Hinterwimmer et al. 35 | 2013 | Isolated | 20 | Retrospective case series | IV | Two-bundle gracilis tendon autograft |
| Kang et al. 37 | 2013 | Isolated | 20 | Randomized controlled trial | II | Static and dynamic semitendinosus autograft |
| Kohn et al. 57 | 2013 | Both | NR | Retrospective case series | IV | NR |
| Ma et al. 43 | 2013 | Isolated | 15 | Randomized controlled trial | II | Semitendinosus autograft |
| Wagner et al. 18 | 2013 | Isolated | None | Prospective case series | IV | Gracilis autograft |
| Wang et al. 52 | 2013 | Isolated | 15 | Retrospective comparative | IV | Double- and single-bundle semitendinosus autograft |
| Becher et al. 27 | 2014 | Isolated | 20 | Retrospective case series | IV | Static/dynamic gracilis autograft |
| Csintalan et al. 28 | 2014 | Isolated | NR | Retrospective case series | IV | Semitendinosus autograft |
| Elias et al. 54 | 2014 | Combined | N/A | Prospective comparative study | IV | Semitendinosus autograft |
| Fink et al. 32 | 2014 | Isolated | 20 | Prospective case series | IV | Quadriceps tendon graft |
| Kang et al 38 | 2014 | Isolated | 20 | Prospective case series | IV | Y-shape semitendinosus autograft |
| Krishna Kumar et al. 39 | 2014 | Isolated | 20 | Retrospective case series | IV | Gracilis tendon autograft |
| Li et al. 40 | 2014 | Isolated | 20 | Retrospective case series | IV | Tibialis anterior allograft |
| Lippacher et al. 42 | 2014 | Isolated | 22 | Retrospective case series | IV | Dual-tunnel gracilis tendon autograft |
| Matsushita et al. 16 | 2014 | Isolated | None | Retrospective case–control | IV | Semitendinosus autograft |
| Song et al. 49 | 2014 | Isolated | 20 | Prospective case series | IV | Semitendinosus or gracilis tendon |
| Astur et al. 26 | 2015 | Isolated | 15 | Randomized controlled trial | II | Gracilis autograft |
| Kita et al. 17 | 2015 | Isolated | None | Retrospective case–control | IV | Dual-tunnel semitendinosus autograft |
| Lin et al. 41 | 2015 | Isolated | 20 | Prospective case series | IV | Double-pulley semitendinosus autograft |
| Moitrel et al. 55 | 2015 | Combined | N/A | Retrospective case–control | IV | NR |
| Mulliez and Lambrecht 12 | 2015 | Both | 20 | Prospective comparative study | IV | Autologous gracilis graft |
| Vavalle and Capozzi 51 | 2015 | Isolated | 20 | Retrospective case series | IV | Superficial quadriceps tendon autograft |
LoE: level of evidence; TT-TG: tibial tuberosity–trochlear groove; MPFL: medial patellofemoral ligament; N/A: not applicable; NR: Not reported.