
Abstract
Purpose:
This study aimed to describe the reverse digital artery cross-finger flap (RDAC flap) in the treatment of failed finger replantation.
Methods:
This study retrospectively reviewed the records of patients who underwent modified RDAC flap reconstructions for failed finger replantation and assessed their outcomes. Of the patients who underwent soft tissue reconstructions for finger injuries between March 2011 and February 2015, we enrolled 11 patients in whom RDAC flap reconstruction procedures were performed to treat the failed replantations.
Results:
The flaps survived in all cases, with a mean static, two-point discrimination value of 5.3 mm (range, 4–7 mm) in the healed flaps. The sizes of the flaps ranged from 2 × 1 cm2 to 2.3 × 1.5 cm2.
Conclusion:
The RDAC flap was introduced by Lai et al., and it is a mixed form with the advantages of both cross-finger flap and heterodigital island flap. Our results suggest that it could provide reliable coverage of the sensate soft tissue of fingers with failed replantation.
Keywords
Introduction
With the advancement of equipment and techniques for microsurgery, finger replantation surgery now reports high success rates. 1,2 However, it is still a burden for physicians, as it is necessary to reconstruct the failed finger replantation. Severed fingers may result in various and irreversible functional, esthetic, and psychological problems, especially in children and young adults. 3 In addition, as patients who have suffered necrosis of a replanted finger are nervous and anxious about the results of consecutive reconstructions, reconstructive techniques that are simple and yield reliable results are required.
There are a few surgical options which can be considered, including amputation site revision, ray amputation, and reconstruction using a local or free flap. If a patient desires to preserve sensation or finger length for personal preference or to use finger prosthesis, reconstruction of the failed finger replantation site is required. This is especially true if the level of amputation is above the proximal interphalangeal joint; however, the use of flaps like the thenar flap, 4 reverse homodigital island flap, 5 or pedicle advancement flaps 6 is limited due to the inadequate length of the preserved finger and anatomical problems. A free flap, such as the partial toe free flap, 7 requires prolonged operative time and results in donor site damage if the flap fails. Therefore, for reconstructions at the site of a failed finger replantation, a simple but reliable reconstruction technique that enables restoration of sensation is necessary.
The reverse digital artery cross-finger flap (RDAC flap) was described by Lai et al., 8 and it is a mixed form with the advantages of both the reverse heterodigital island flap and the classical cross-finger flap. This study retrospectively reviewed patients who underwent RDAC flap reconstructions for failed finger replantations and assessed the outcomes of these procedures.
Patients and methods
Of the patients who had undergone soft tissue reconstruction of failed finger replantation between March 2011 and February 2015, 11 patients (7 men and 4 women) who underwent RDAC flap reconstruction were enrolled in this study. Institutional review board approval was obtained for this retrospective chart review. A static, two-point discrimination (s-2PD) test at flap site was performed, 6 months after surgery. Donor morbidity, including total range of motion, cold intolerance, neuroma, and scar contracture, was accessed at final follow-up.
Operative technique
Each surgery was performed under brachial plexus anesthesia. Prior to the flap procedure, a thorough debridement was performed to prevent infection (Figure 1). A digital Allen test was conducted on the donor digit to ascertain the patency of both proper digital arteries. The digital artery of the donor finger was identified using a fine Doppler probe. The flap was designed on the adjacent finger.

(a) A 28-year-old man presenting with necrosis of the left little finger after a failed finger replantation. (b) Meticulous debridement of the necrotic area was performed to prevent infection.
For reconstructions involving the little finger, the ulnar digital artery of the ring finger was used as the vascular pedicle. For index finger reconstructions, the radial side of a middle finger flap containing the radial digital artery was elevated (Figure 2). The size of the flap was matched to the region of the injured finger requiring coverage. A midlateral line of the donor finger was drawn, and a flap slightly larger than the size of the soft tissue defect was designed. A width of about 1.5 cm around the central axis was maintained and the length was about 5 mm longer than the size of the soft tissue defect. At this time, the flap was preferably positioned at the middle part of the phalanx. The distal pedicle of the flap was preferably positioned within about 5 mm of the amputated finger. Care was taken so that the distal pedicle does not cross the donor joint and to prevent donor joint stiffness.

Injured little finger with some loose tissue. A ring finger flap was designed at the ulnar site. Illustrations and pictures of the modified reverse heterodigital artery sensory local flap are shown. The flap was elevated under surgical loupe magnification to facilitate the dissection of the dorsal branch of digital nerve and digital artery from the ring finger. The proximal ulnar digital artery was ligated, and the dorsal branch of the digital nerve, which connects to the radial digital nerve of the little finger, was dissected, leaving at least a 0.5–1.0 cm nerve tail attached to the flap. (a: ring finger proximal ulnar digital artery; b: dorsal branch of the ring finger digital nerve; and c: little finger digital nerve). The flap also maintained tissue viability in the distal amputation site. The radial digital nerve of the little finger and the dorsal branch nerve of the ring finger were sutured together using 10-0 nylon sutures under magnification.
After drawing the flap, an incision was made along the path of the digital nerve on the donor finger to undermine the subcutaneous tissue, under surgical loupe magnification. The digital nerve was identified, as was the dorsal aspect of the dorsal branch of the proper digital nerve, and care was taken to spare the digital nerve. Next, the dorsal branch of the proper digital nerve was separated proximally, and a 0.5–1.0-cm nerve tail was left attached to the flap (Figure 3). The digital artery was identified and ligated proximally. An epineural neurorrhaphy was performed under an operating microscope, and two or three 10-0 nylon micro-sutures were placed to join the sensory nerve (the dorsal branch of the digital nerve) tails on the flap and the ends of the digital nerves on the recipient finger. Upon elevation of the donor flap, sufficient subcutaneous fat was included to ensure maximal cosmetic value. Also, the distal part of the flap was not completely separated, permitting innervation of the cross-finger flap.

Neurorrhaphy illustration. The stability of the distal flap was maintained by decreasing the pedicle movement and preventing venous congestion (d: digital artery of the ring finger).
Thus, the flap maintained stability at the distal part of the amputation site, while also decreasing the pedicle movement and preventing venous congestion. Vascular perfusion was assessed through the observation of blood oozing from the flap margin and capillary refilling. The flap readily covered the amputation site (Figure 4). The donor sites were closed primarily without skin grafts, because the flap widths were <1.5 cm. We bandaged the two fingers with gauze and applied a dorsal block splint for 2 weeks. After confirming flap viability, detachment was performed under local anesthesia, and rehabilitation began thereafter (Figure 5).
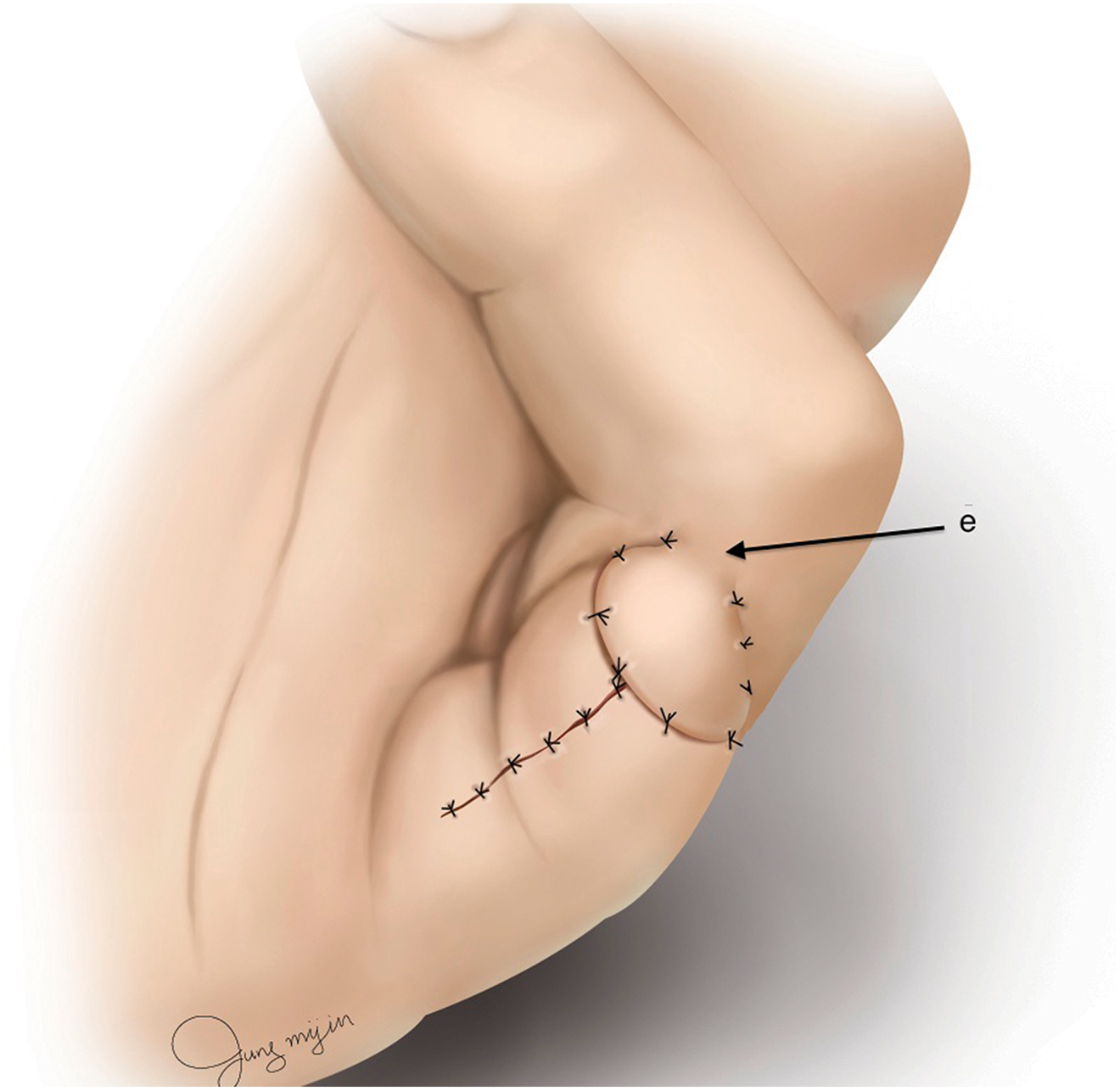
Illustration of flap fixation. The flap was not completely separated as in an innervated cross-finger flap (e: skin pedicle).

Finger with a satisfactory outcome, 6 months after surgery.
Results
The mean patient age was 41 years, and the mean follow-up period was 53 months (range, 41–63 months). The etiology of the injuries was failed replantation of the amputated fingers at the Proximal Interphalangeal (PIP)-joint level (nine cases) and near the Distal phalangeal (DIP) joint (two cases). The injuries involved either the index finger (four cases) or the little finger (seven cases).
All 11 flaps survived, and the flap sizes ranged from 2 × 1 cm2 to 2.3 × 1.5 cm2. S-2PD testing of the healed flaps yielded a mean value of 5.3 mm (range, 4–7 mm). Well-known complications associated with finger flap procedures, such as dysesthesia and cold intolerance, were not observed. The mean of total range of motion of donor site was 163° (range, 155–170°). Scar contracture at donor site was observed in two patients, but no patient required an additional procedure (Table 1).
Summary of patient data and clinical results.

aDIP: Distal Inter-Phalangeal.
bPIP: Proximal Inter-Phalangeal.
cTROM: Total Range Of Motion.
Discussion
When finger necrosis occurs after a failed replantation, the treatment options need to be carefully weighed. The factors to be considered in choosing an appropriate treatment option include patient preference, etiology of the finger injury, and the length of the remaining finger. When the patient desires to preserve finger length, a replantation method with low complexity and high success rate is needed. Except in cases where there is an inevitable loss, maximal finger length should be preserved to facilitate the use of a finger prosthesis. 3,9 A minimum residual length of 15 mm from the interdigital web to the residual tip is required for a secure-fitting prosthesis, because it is held in position on the stump via a vacuum “suction-cup” effect. 10
A free flap approach requires long operative times. 11 In our experience, patients with a replantation failure tend to be reluctant to undergo a free flap procedure. For patients with tissue necrosis after failed replantation, a relatively simple local flap is the preferred surgical option. However, a local flap often cannot cover the area of amputation, because the remaining stump is usually too short to be adequately covered by a thenar flap or reverse homodigital island flap. Thus, there are only few methods available for reconstruction.
The classical cross-finger flap is a reliable option to maintain the finger length. Moreover, the procedure is easy to perform, results in less morbidity of the donor site, yields good skin texture, and has a low failure rate. Occasionally, depending on the cutting pattern of the injured finger, the flap is barely suitable for covering the stump and maintaining flap and finger positions. As a result, the donor site of a cross-finger flap suffers from reduced range of motion and pinch grip power. Poor sensation, disfiguration, cold intolerance, and donor site pain are other problems associated with the classical cross-finger flap procedure. 12
The heterodigital island flap is used to cover large, acute, and chronic defects in the middle and distal phalanges that cannot be covered with other local digital sensory flaps. The dorsal branch of the digital nerve is useful for innervating heterodigital island flaps in such cases. 13 The dorsal branch originates from the base of the proximal phalanx, runs obliquely across the dorsal proximal phalanx, and terminates on the ipsilateral dorsum of the middle phalanx. 14 Thus, a heterodigital island flap can restore digital sensation with good color matching and allows for early finger motion. 15 The disadvantages of this procedure are that it requires a two-stage operation, includes loose skin wrapping around the exposed vascular pedicle, 16 and involves an unstable pedicle. 17 Additionally, consistent care is required to prevent the vascular pedicle from drying out or becoming compressed.
The RDAC flap is a modified cross-finger flap with the merits of the heterodigital island flap. This approach also converts the direction of the flap elevation to a right angle, in contrast to the classical cross-finger flap method (Table 2). The RDAC flap anatomy is similar to that of the reverse heterodigital artery sensory flap. The RDAC flap includes the digital artery opposite to the pedicle and distal arch as the communicating branch. However, the sensory nerve is harvested from the terminal dorsal branch of the proper digital nerve. The advantage of this is that the vascular pedicle is attached to the skin of the flap and does not require any special protection. In case of an RDAC flap, the digital artery is located in the skin pedicle and is not exposed. Therefore, it has a firm soft tissue and holds it stable. The skin connection helps to maintain the flap’s distal viability, while decreasing the pedicle movement and preventing venous congestion (Table 2). The complications associated with the RDAC flap include the possibility of decreased skin sensation over the dorsal middle phalanx due to utilization of dorsal branches of the proper digital nerve. Fortunately, this morbidity is minimal because sensation in that area is not functionally important. 18 Although resection of the dorsal branch of the digital nerve or dorsal digital nerve may result in hypersensitivity or symptomatic neuroma, such complications were not observed in our study. Two cases of mild donor site scar contracture were observed, but they did not result in any serious sequelae.
Comparison with reconstruction using the other method.

Primary closure at the digital level is generally not favorable because of the risk of ischemia or secondary venous stasis. Therefore, the lateral aspect of the middle phalanx is commonly incised and the turnover vascular pedicle is put in place and covered with a skin graft. 19 However, in our series, the donor sites were closed primarily without skin grafts, as the flap widths were <1.5 cm. In the authors’ experience, the largest flap size was 2.3 × 1.5 cm2. A larger flap is possible with a donor skin graft. However, in the absence of a donor skin graft, the flap size should be less than 2.3 × 1.5 cm2.
The authors introduced a method called “modified innervated sensory cross-finger flap,” which showed good sensory recovery when the initial case was published. 20 We analyzed cases of patients who had undergone the same operation. At the last follow-up, neuroma occurred in one patient and mild scar contracture in two patients. The mean range of motion of the donor finger was 165°. Because the number of samples was small, it is difficult to analyze the complications. However, complications that commonly occur in cross-finger flaps, such as cold intolerance, lack of sensation, and decreased range of motion, may occur with this similar procedure. We also believe that the frequency of complications is not significantly different from that observed in the cross-finger flap. In the case of Lee’s innervated cross-finger flap, which is similar to that of the present technique, excellent results of about 4 mm in two-point discrimination were reported. In addition, long-term follow-up of cross-finger flap technique reported very good sensory recovery. 21,22 When two-point discrimination results were compared between the innervated flap and the reverse island flap, the neurovascular island flap was superior at the initial stage, but there was no difference at the end of follow-up. Rabarin et al. reported a long-term follow-up of 19.7 years with no pain at the donor site, especially in the fingertip, and no neuralgia, necrosis, or wound abnormality. 21 These results can be further supported in applying the current methods to patients.
The advantages of the RDAC flap include (1) reliable blood supply and a stable pedicle construct, (2) maximal preservation of digital length, (3) retention of similar glabrous skin texture and color, (4) restoration of flap sensation, (5) improved cosmetics, (6) minimal donor site damage, and (7) primary donor site closure when the width is <1.5 cm. The disadvantages of this technique include (1) a need for a two-stage operation, (2) difficult dissection of the dorsal branch of the digital nerve, (3) the requirement of microsurgical techniques, (4) sacrifice of the normal digital artery, and (5) limited flap size.
The contraindication is the same as that for cross-finger flaps and includes patients older than 50 years of age, rheumatoid arthritis, multiple injured digits, vasospastic disorders including Buerger’s disease, Raynaud’s phenomenon, and young children because of lack of compliance and as simpler methods are usually adequate. Therefore, it is recommended to perform a ray amputation in case of injuries above the PIP joint.
This study was limited by its small sample size and a non-comparative study design. As this was a short-term follow-up study, future studies with longer follow-up duration are needed.
Limited reconstructive options exist after failed finger replantation. In such cases, a simple but successful surgical technique is desirable. Given the characteristics of this procedure, the RDAC flap can be considered when the amputation or crushing injury occurs near the PIP joint, sensation in the flap is necessary, or use of finger prosthesis is anticipated. The RDA cross-finger flap provides reliable coverage of the sensate soft tissues for the repair of such finger injuries.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.