
Abstract
Background:
While various implants are currently used for the treatment of femoral trochanteric fractures in Japan, ‘mismatches’ have been known to occur between patient and implant type. The purpose of this study is to identify morphological characteristics of elderly Japanese females, both in terms of the shape of proximal femur and its anterior curvature in order to evaluate the suitability of implants for treatment of femoral trochanteric fractures using 3D-computed tomography (CT) scanning.
Methods:
This study used CT scan data taken from 50 elderly females (aged 70 years or older). Neck–shaft (NS) angle and height of the greater trochanter (GT) were measured under defined conditions (TPI: theoretical plane to place implant). Anterior curvature of the femoral shaft was also measured.
Results:
On average, the NS angle was found to be 128.1° and GT height was 62.4 mm. Average curvature radius was 1040 mm. As for the NS angle, the centrum-collum-diaphysis angles of existing implants (125° or 130°) are reasonable. In elderly Japanese patients, the proximal femur shows specific characteristics. As GT height is very short, the implant may easily interfere with the lateral cortex. Additionally, the curvature radius calculated (1040 mm) was smaller than that of past reports, indicating strong curvature in the Japanese elderly.
Conclusion:
Our measurement results are potentially useful in the avoidance of intraoperative trouble caused by mismatch of implants.
Introduction
Various implants are currently used for the treatment of femoral trochanteric fractures in Japan; however, it has been recognized that as many of these implants are “foreign manufactured”, a ‘mismatch’ between patient and implant type may occur when used to treat the smaller Japanese elderly.
The purpose of this study is to identify morphological characteristics of elderly Japanese women, both in terms of the shape of proximal femur and its degree of curvature, through the use of 3D-computed tomography (CT), in order to evaluate implant suitability for treatment of femoral trochanteric fractures.
Materials and methods
3D-CT volume data of the whole femur were obtained from 50 cases of women treated at our institution for hip fracture. All patients were aged 70 or older and had no deformities or surgical history on the unaffected side.
This study was approved by the institutional review board of the first author’s institution. We obtained consent from all patients, complying with the principles laid down in the Declaration of Helsinki. Our reporting of patients is completely anonymous, protecting the privacy and dignity of all patients.
Morphological evaluation of the proximal femur
Measurement was performed using the image display software Zio-station®. Firstly, the anterior–posterior axis of the femur is determined with reference to the posterior condyles. Currently, the use of implants of 170 mm is mainstream, the axis connecting the medullary canal center of lesser trochanter level and 150 mm distal from tip of the greater trochanter (GT), is defined as the “proximal shaft axis.” Figure 1(a) shows how, viewed from the head side (proximal), images taken in this manner display the medullary cavity in the proximal femur as almost vertical. Using this image, the anteversion angle between the line connecting the posterior condyles and the neck is measured (Figure 1(b)).

Measurement method. (a, b) Proximal bone axis and anteversion; (c, d) match the neck axis and the proximal bone axis.
Internally rotating the lateral view with reference to the posterior condyle (Figure 1(c)) by the measured angle of anteversion produces the image seen in Figure 1(d); the femoral head center and the proximal shaft axis appear almost in line. This image is closer to a “True Lateral View.”
Figure 2(a) shows a cross section of the femur cut along the straight line shown in Figure 1(d). This plane contains the center of the femoral head and proximal shaft axis. This is “the plane on which the central axis of the implant should be placed theoretically” and is defined as the “theoretical plane to place implant (TPI)”.
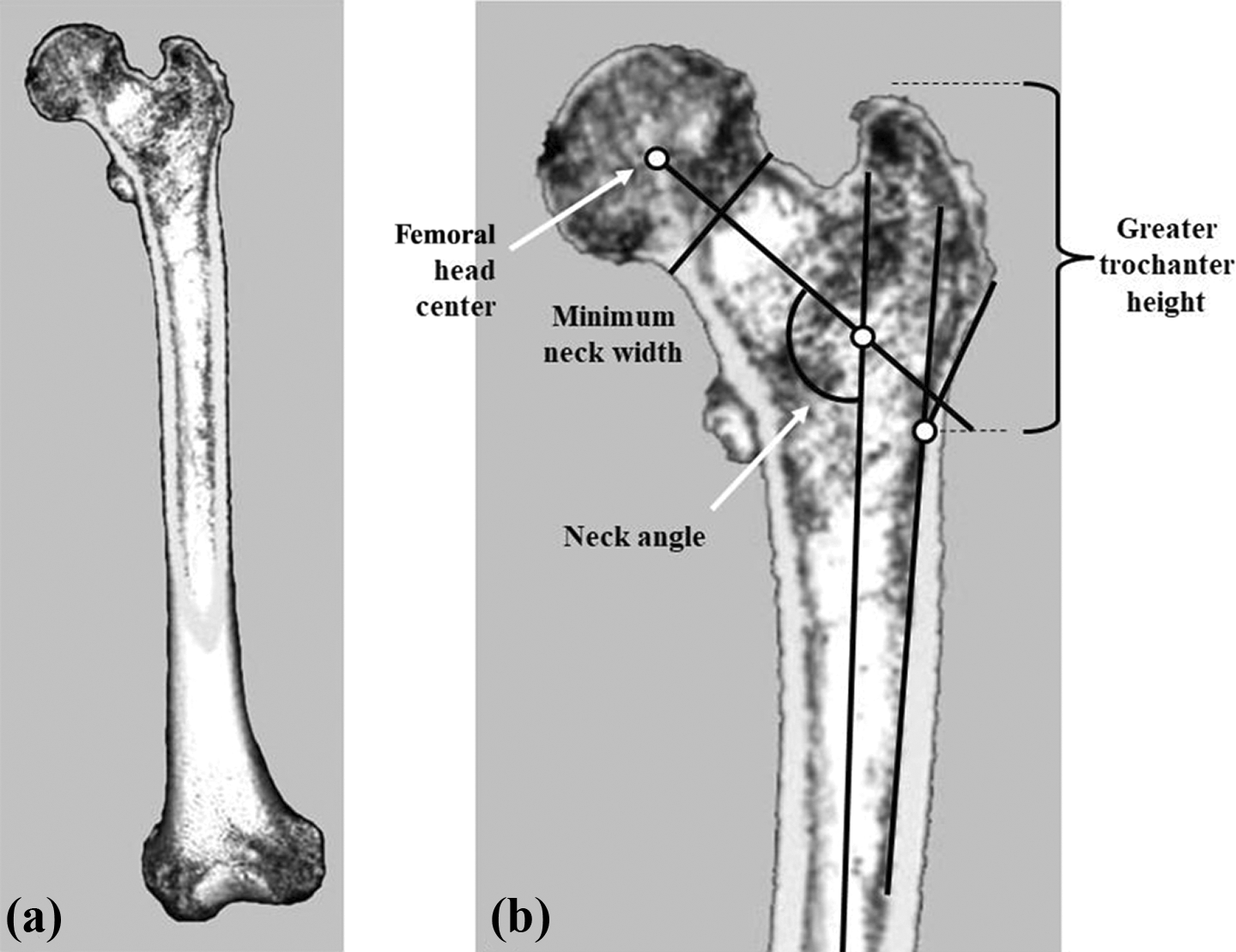
Measurement on the TPI. (a) TPI; (b) measurement of NS angle and GT height. TPI: theoretical plane to place implant; NS: neck–shaft; GT: greater trochanter.
Measurement is done on the TPI and the neck–shaft (NS) angle, calculated by measuring the angle between the straight line connecting the center of the femoral head with the midpoint of the minimum neck width and the proximal shaft axis. Furthermore, the inflection point where the cortex of the GT extends from the shaft was established as the lower border of the GT, and evaluation carried out of the height of GT (Figure 2(b)).
Evaluation of anterior curvature
For evaluation of femoral anterior curvature, firstly the anteroposterior (AP) view was established based on the posterior condyles. Within the femoral bone shaft, the proximal end was defined as the level of lesser trochanter and the distal end as 50 mm proximal from the articular surface. Using the straight line connecting the midpoints of the bone widths at both ends of the bone shaft as a reference axis, measurement was carried out on the lateral view that was parallel to posterior condyle axis. Then, the femoral shaft is divided into four sections and the X and Y axis set as shown in Figure 3(a). The distance of anterior deviation was measured from each point on the reference axis and recorded as coordinates (Figure 3(b)).

Measurement of anterior curvature. (a) Femoral shaft divided into 4; (b) measure the distance at each point.
Results
Morphological evaluation of the proximal femur
Measurement results are shown in Table 1. The average age of subjects was 83.0 years and average height was 149.1 cm. The average NS angle was 128.1°. The average height of GT was 62.4 mm; however, there was considerable variation across subjects.
Result.

Head: diameter of the head; NS angle: neck–shaft angle; GT height: greater trochanter height.
Evaluation of anterior curvature
Figure 4 shows the coordinates from the 50 cases plotted on to a graph. The result of approximating the three measured points with a circle gave an average curvature radius of 1040 mm, ranging from a minimum of 658 mm up to a maximum of 1905 mm.

Results of curvature radius measurement. Curvature radius: R 1040 mm (658–1905 mm).
Discussion
Proximal morphology
In the preoperative planning for treatment of proximal femoral fractures, evaluation of points such as the NS angle and the medullary canal diameter is generally carried out using X-ray imaging of the unaffected side as a reference. It is important to be aware that the shape may differ depending on the conditions under which the femur is observed. For example, it is well known that in an AP view of the femur based on knee joint (posterior femoral condyles), as the neck has anteversion, the NS angle is observed as being slightly large. Even with the application of internal rotation to reduce the effect of the anteversion, it remains difficult to obtain an accurate AP view of the neck, as the angle varies depending on the individual. Furthermore, in cases with strong anterior curvature, the proximal portion of the femur may show considerable inclination. In other words, it seems as if the hip joint is flexed, the apparent neck angle is small, and the medullary cavity of the bone shaft is enlarged. To minimize such errors, the ideal AP view of the proximal femur would be one which takes in to consideration not only anteversion but also anterior curvature. However, it is not currently possible using X-ray imaging to make the fine adjustments necessary to produce such an image. Due to the difficulty in finding solutions to the problems listed above, we chose to define and make measurements from the “TPI” as described.
A comparison of our measurement results and those reported by Tsubouchi 1 is shown in Table 2. Although the average values are roughly similar, our data tended to show lesser variation in all aspects, except for the height of the trochanter, for which the method of measurement differed. This study is considered to be more advantageous because the age and sex of subjects are limited to be more accurate. X-ray lacks accuracy because the enlargement ratio is not constant in the measurement due to imaging conditions.
Comparison with measurement results from X-ray study.a

CT: computed tomography; NS: neck–shaft; GT: greater trochanter.
a The method of measurement differed for GT height.
In the measurement results, the average NS angle on the TPI was found to be 128.1°. As shown by our results, there are many femurs with a NS angle of less than 130°. Therefore, predominate centrum-collum-diaphysis angles of popular implants (125° and 130°) seems reasonable. Also, the average GT height was 62.4 mm, and more than half of these were inwardly convex in shape. So, to avoid jamming of the nail at the proximal cavity, the proximal part of the nail should be shortened to about 60–65 mm and the bend point also set to the same level. Figure 5 shows the matching of two nails to the TPI of average shape femur. It seems that the higher the nail bend point, the less interfere with the lateral cortex. In recent years, there have been reports in Japan that identify issues with the shape of foreign made nails. Teramoto et al. 2 reported a mismatch in 6% of cases using Japanese Proximal Femoral Nail Antirotation (PFNA). Watanabe et al. 3 found that in InterTAN, jamming occurred in 4 of 29 cases (13.8%) due to contact with the lateral cortex, and proposed narrowing the proximal part of the nail as a countermeasure to prevent interference. Maehara et al. investigated the morphology of the proximal part of the femur using templates based on X-ray imaging 4 and CT 5 , reporting that the higher the location of the nail bend point, the less likely it is to interfere with the cortex. We believe that these current results also suggest the importance of the nail bend point.
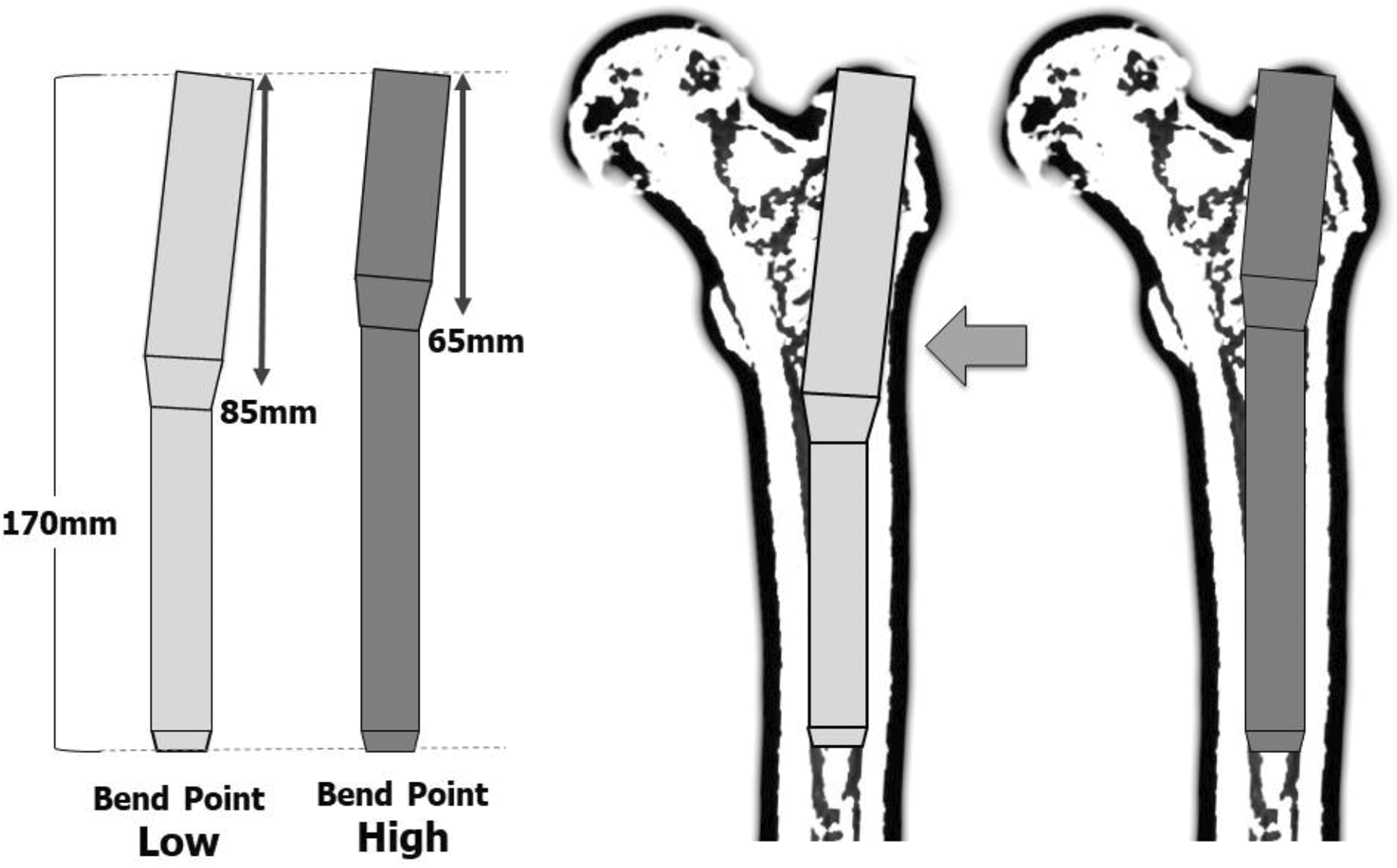
Difference of suitability by bend point. The low bend point can be a risk to interference with the lateral cortex.
Anterior curvature
There are relatively few previous reports on femoral anterior curvature. Domestically, Onoue 6 reported an average curvature radius of 1159 mm based on X-ray imaging from 160 limbs. He also found a tendency for stronger curvature in women over men and for curvature to become stronger with age. Additionally, in X-ray examination of 250 limbs, Kanekasu et al. 7 stated that when intramedullary nails with a curvature radius of 3000 mm were used, there was a possibility of mismatch in 62 limbs (25% of cases): therefore, extra caution should be placed on curvature radius below 1000 mm. In X-ray measurement of femoral curvature across 14 cadaver specimens, Harper et al. 8 reported an average curvature radius of 1144 mm (689–1885 mm). Egol et al. 9 reported an average curvature radius of 1200 mm (530–3260 mm) based on digital photography of the exterior of 948 femoral specimens. Additionally, Ehmke et al. 10 conducted reaming on 31 femoral cadaver specimens using a reamer with attached sensors which analyzed tip trajectory three-dimensionally, finding an average curvature radius of 1210 mm. Recently, Marratt et al. 11 calculated a curvature radius of 1120 mm from CT data of 1961 patients and reported that the strength of the curvature correlated with femur length and stature.
In our study, limited to elderly women, although the curvature radius shows a considerable range, the average value of 1040 mm is smaller than any previously reported. In terms of existing gamma-type intramedullary nails, the curvature radius of long nails is often approximately 1500–1800 mm. However, a risk has been identified of damaging the femoral anterior cortex with the nail. The results of this study suggest that when using gamma-type long nails for treatment of reverse oblique trochanteric fractures and subtrochanteric fractures in elderly Japanese women, nails with a smaller curvature radius (more curved) appear to be safer. Furthermore, the development of a more compatible model for such conditions is required.
The advantage of this research using CT imaging was the ability to reduce, as much as possible, errors due to the magnification caused by X-ray imaging, as well as errors due to distortion, occurring in the peripheral portion of the image. On the other hand, there were several limitations; The medullary space itself cannot be evaluated as measurement is taken at the midpoint of the width of the cortex, rather than the center of medullary cavity. While 3D-CT imaging was used, actual measurement was done with the 2D projection on the monitor. Lateral curvature was not considered. The radius of curvature, indicating the degree of curvature, was calculated by approximating to a simple circle.
However, even considering these limitations, these measurement results, taken solely from elderly Japanese women, are significant in terms of implant selection and avoidance of intraoperative difficulties for femoral fracture treatment. This is particularly the case for trochanteric and subtrochanteric fractures in elderly Japanese women which look likely to increase in future.
Conclusion
We proposed a reference plane called “TPI” and measured NS angle and height of GT on it. On this plane, NS angle was found to be 128.1° and height of GT was 62.4 mm. In Japanese elderly women, the radius of curvature of the femur was 1040 mm, which was smaller than in the past reports. We must be careful when using intramedullary nails. By knowing these numerical values, it may be possible to reduce intraoperative troubles due to mismatch of implants.
Footnotes
Authors’ note
This article is based on a study first reported in the “The morphology of the femur in elderly Japanese female: Analysis using 3D-CT” (Maehara T, Shinohara K, Yamashita K, et al., The morphology of the femur in elderly Japanese female: Analysis using 3D-CT. JSFR 2012; 34: 451–455).
Acknowledgments
We would like to express our deepest gratitude to Dr Shinohara (Okayama medical center) and Dr Yamashita (Tokushima university) for providing support and encouragement in the present study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.