
Abstract
Purpose:
The aim of this study was to investigate the histopathological changes in the humeral head in cuff tear arthropathy (CTA) compared with those in glenohumeral osteoarthritis (OA) and humeral neck fracture, which served as non-cuff tear controls.
Methods:
Twenty-three humeral heads extracted at the time of shoulder prosthesis arthroplasty between June 2014 and July 2015 were evaluated in the present study. The diagnoses included four-part humeral neck fracture (n = 4; average age, 85.0 years), glenohumeral OA (n = 4; average age, 71.0 years), and CTA (n = 15; average age, 73.0 years). The humeral heads were evaluated pathologically by hematoxylin and eosin and Safranin-O staining, and the thickness of the articular cartilage was measured.
Results:
Fibrillation, thinning, and tearing of the cartilage were observed in the superior area of the humeral heads in CTA and glenohumeral OA. In CTA cases, clusters of chondrocytes in the cartilage were observed. Moreover, the thickness of the cartilage layer in the middle of the humeral head was 1.54 ± 0.07, 0.32 ± 0.46, and 2.19 ± 0.50 mm in humeral neck fracture, glenohumeral OA, and CTA, respectively. The cartilage layer in CTA was thicker than that in glenohumeral OA (CTA vs. OA: p < 0.05).
Conclusion:
OA changes in the superior area of the humeral heads and thickening of the cartilage layer from the middle to the inferior of the humeral heads were confirmed histopathologically, suggesting that simultaneous mechanical and nutritional factors might be contributing to CTA pathogenesis. The current study provided the better understanding of cartilage damage and thickening in CTA. This will help guide treatment options in the setting of CTA.
Introduction
Neer et al. 1 defined cuff tear arthropathy (CTA) as a pathoanatomical change associated with chronic full-thickness rotator cuff tear, which includes erosion of the osseous structure, osteopenia of the humeral head, and restriction in shoulder motion. Neer et al. and Visotsky et al. also suggested the mechanisms by which mechanical and nutritional factors are correlated with CTA. 1,2 Although CTA is common in ordinary clinical practice, it remains one of the most difficult shoulder pathologies to treat. Regarding CTA treatments, simple cuff tear repair procedures have been unfavorable because osteoarthritis (OA) conditions should be managed in the context of CTA cases, 3 either have been only humeral head replacement. 4 Anatomical total shoulder arthroplasty combined with cuff tear repair has achieved favorable clinical outcomes. 5 Recently, some reports have found that reverse shoulder arthroplasty has favorable outcomes with CTA cases that do not require cuff tear repair. 6,7
In CTA cases, enlarged humeral heads have been often observed. Previous reports revealed that the diameter of affected humeral heads, which was determined based on the diameter of the humeral head of CTA on X-ray, was nearly 5 mm larger than that of the contralateral side. 8,9 In rat animal models, pathological findings in the humeral heads in CTA models have been reported. 10 However, rat shoulder joints are weight-bearing joints. Hence, the influence of weight-bearing OA changes should be considered in CTA changes in rat shoulder model. Moreover, little is known regarding the pathology of the humeral head in human CTA as nonbearing joint, 2 particularly in the histopathological perspective.
The purpose of the present study was to clarify the pathology and etiology of CTA by evaluating the histopathological changes in the humeral head in CTA cases and comparing those findings with the changes associated with glenohumeral OA and humeral neck fracture, which served as non-cuff tear controls.
Materials and methods
Twenty-three extracted humeral heads following shoulder hemiarthroplasties between June 2014 and July 2015 were evaluated in the present study. The diagnoses included four-part humeral neck fracture in 4 patients, glenohumeral OA in 4, and CTA in 15. Patients’ details in these three groups are given in Table 1. All patients provided written informed consent, and the research protocol was approved by the Institutional Review Board of our institute (Institutional Review Board Approval: Hokushin Orthopaedic Hospital (IRB approval no. 1502).
Patient characteristics.

CTA: cuff tear arthropathy; OA: osteoarthritis.
Groups
Group 1: Humeral neck fracture
In humeral neck fractures, four shoulders (one male and three females) with four-part humeral neck fracture as defined by Neer’s classification system were evaluated. The average age of the patients was 85.0 years (range: 77–93 years), and the average time from injury to surgery was 13 days (range: 6–24 days). An intact rotator cuff was confirmed during surgery.
Group 2: Glenohumeral OA
In glenohumeral OA cases, four shoulders (one male and four females) were evaluated. The average age of the patients was 71.0 years (range: 61–86 years). All patients had severe OA without rotator cuff tear.
Group 3: CTA
In CTA cases, 15 shoulders (eight males and seven females) were evaluated. The average age of the patients was 73.0 years (range: 68–84 years). Patients with chronic rotator cuff tear with femoralization of the humeral head were categorized into this group. To exclude patients with cartilage damage of the humeral head at the middle portion, those with Seebauer type IB injury (minimal superior migration of the humeral head and medial erosion of the glenoid) were excluded. 2
Pathologic examination
The extracted humeral heads were decalcified using a decalcifying solution that contained formic acid, 100% formalin, and distilled water at a ratio of 5:1:15 for 20 days. The decalcifying solution was renewed once a day. Each humeral head was sliced along the middle line on the coronal plane from superior to inferior direction and the arc of the humeral head was divided into thirds (Figure 1(a) and (b)). Then, each humeral head was stained with hematoxylin and eosin (H&E) and Safranin-O. Each layer of the cartilage (tangential, transitional, radial, and calcified zones), subchondral bone, and trabecular bone was observed and compared among the three groups. Finally, the maximum thickness of the cartilage in the middle of the humeral head was measured. The brightness of the images was adjusted with Adobe Lightroom software (Adobe® v2.0.2) and was not modified beyond the standard adjustment of brightness levels.
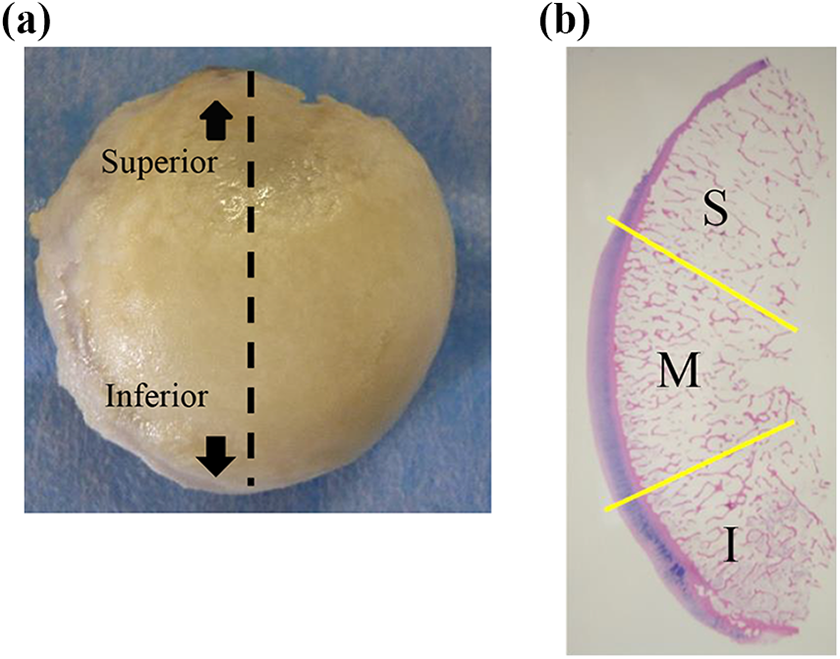
Extracted humeral head with CTA. (a) The humeral head was sliced along the middle line on the coronal plane from the superior to inferior directions. (b) H&E staining of a humeral head (magnification ×10). The humeral head was divided into three areas. S, superior; M, middle; I, inferior. CTA: cuff tear arthropathy; H&E: hematoxylin and eosin.
Statistical analysis
To compare the thickness of the cartilage among the three groups, single-factor analysis of variance between unpaired groups was performed. For nonparametric multiple comparison, the Steel–Dwass test was used to compare among the three groups. p Values < 0.05 were considered statistically significant.
Results
Group 1: Humeral neck fracture
The cartilage, subchondral bone, and trabecular bone showed normal structure and nonspecific findings (Figure 2(a) and (b)). Thickness of the cartilage was constant from the superior to the inferior part of the humeral head. The average maximum thickness of the cartilage in the middle of the humeral head was 1.54 mm (range: 1.46–1.60 mm) at the middle portion. As this group showed normal articular cartilage, subchondral bone, and trabecular bone according to both macroscopic and histopathological analyses, we considered those specimens as a normal control group of elderly subjects.
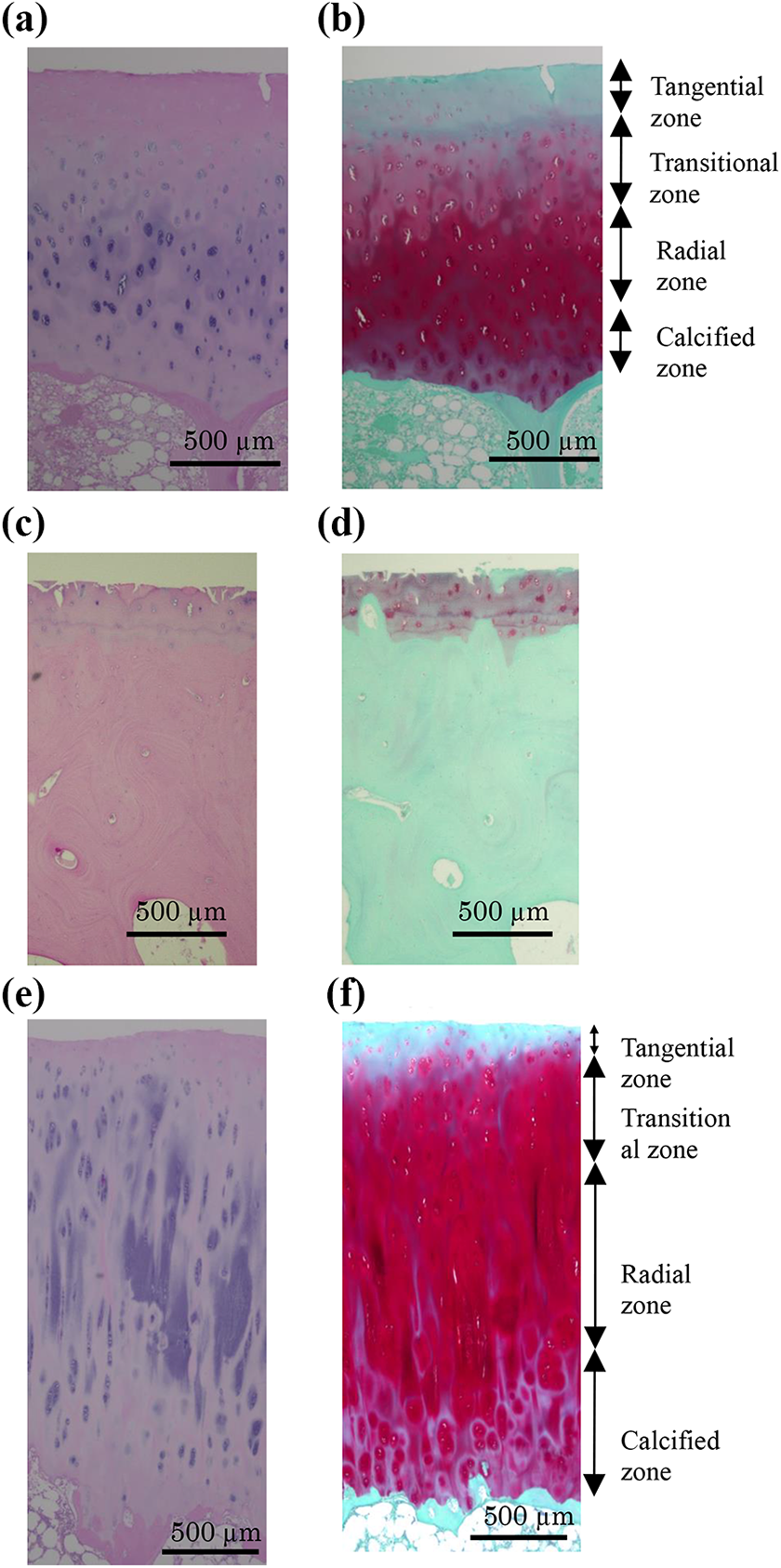
Pathological findings of fracture, glenohumeral OA, and CTA. (a) H&E staining of a humeral head with humeral neck fracture (magnification ×40). (b) Safranin-O staining of a humeral head with humeral neck fracture (magnification ×40). (c) H&E staining of a humeral head with glenohumeral osteoarthritis (magnification ×40). Fibrillation, fissuring, and eburnation of the cartilage and exposure of the subchondral bone were observed. (d) Safranin-O staining of a humeral head with glenohumeral osteoarthritis (magnification ×40). The stained zone was smaller than that in the humeral neck fracture group. (e) H&E staining of a humeral head with CTA (magnification ×40). In the middle of the humeral head, thickening of the cartilage, multiple clusters of chondrocytes, and an irregular calcified zone were observed. The average maximum thickness of the cartilage was 2.19 mm (range: 1.40–3.14 mm). (f) Safranin-O staining of a humeral head with CTA (magnification ×40). Radial and calcified zones showed increased staining. Bars: 500 μm. CTA: cuff tear arthropathy; H&E: hematoxylin and eosin; OA: osteoarthritis.
Group 2: Glenohumeral OA
Fibrillation, fissuring, eburnation of the cartilage, and exposure of the subchondral bone, with advanced stage of cartilage degeneration, were observed with H&E staining from the superior to the inferior part of the humeral head (Figure 2(c) and (d)). The average maximum thickness of the cartilage in the middle of the humeral head was 0.32 mm (range: 0–1.10 mm). Compared with those in the humeral neck fracture group, the Safranin-O-stained zone was smaller (Figure 3(b)) and the trabecular bone was thicker.

Cartilage thickness. Cartilage was thicker in the CTA group than in the humeral neck fracture and OA groups. *p < 0.05.: CTA: cuff tear arthropathy; OA: osteoarthritis.
Group 3: CTA
Fibrillation, thinning, and tearing of the cartilage were observed in the superior area of the humeral head with H&E staining. In contrast, multiple clusters of chondrocytes, an irregular calcified zone, and thickening of the cartilage were observed from the middle to the inferior part of the humeral head (Figure 2(e)). These findings were more prominent in the inferior area where thickening was observed in the radial and calcified zones. The average maximum thickness of the cartilage in the middle of the humeral head was 2.19 mm (range: 1.40–3.14 mm). Cartilage was thicker in the CTA group than in the glenohumeral OA group (CTA vs. OA: p < 0.05; Figure 3). The thickest portion was in the middle area in 11 (73%) of 15 shoulders and in the inferior area in 4 (27%) of 15 shoulders. Compared with those in the humeral neck fracture group, the Safranin-O-stained zone was larger (Figure 2(f)) and the trabecular bone was thinner in the CTA group, and multilayer tidemarks in the deep layer of the cartilage were observed in 12 (80%) of 15 shoulders (Figure 4(a)). An irregular subchondral bone structure was found in 8 (53%) of 15 shoulders (Figure 4(b)), and vascularization of the cartilage and calcification around the blood vessel were observed in 4 (27%) of 15 shoulders (Figure 4(c) and (d)). Cartilage tissue inside the subchondral bone was found in 7 (47%) of 15 shoulders (Figure 4(e) and (f)).
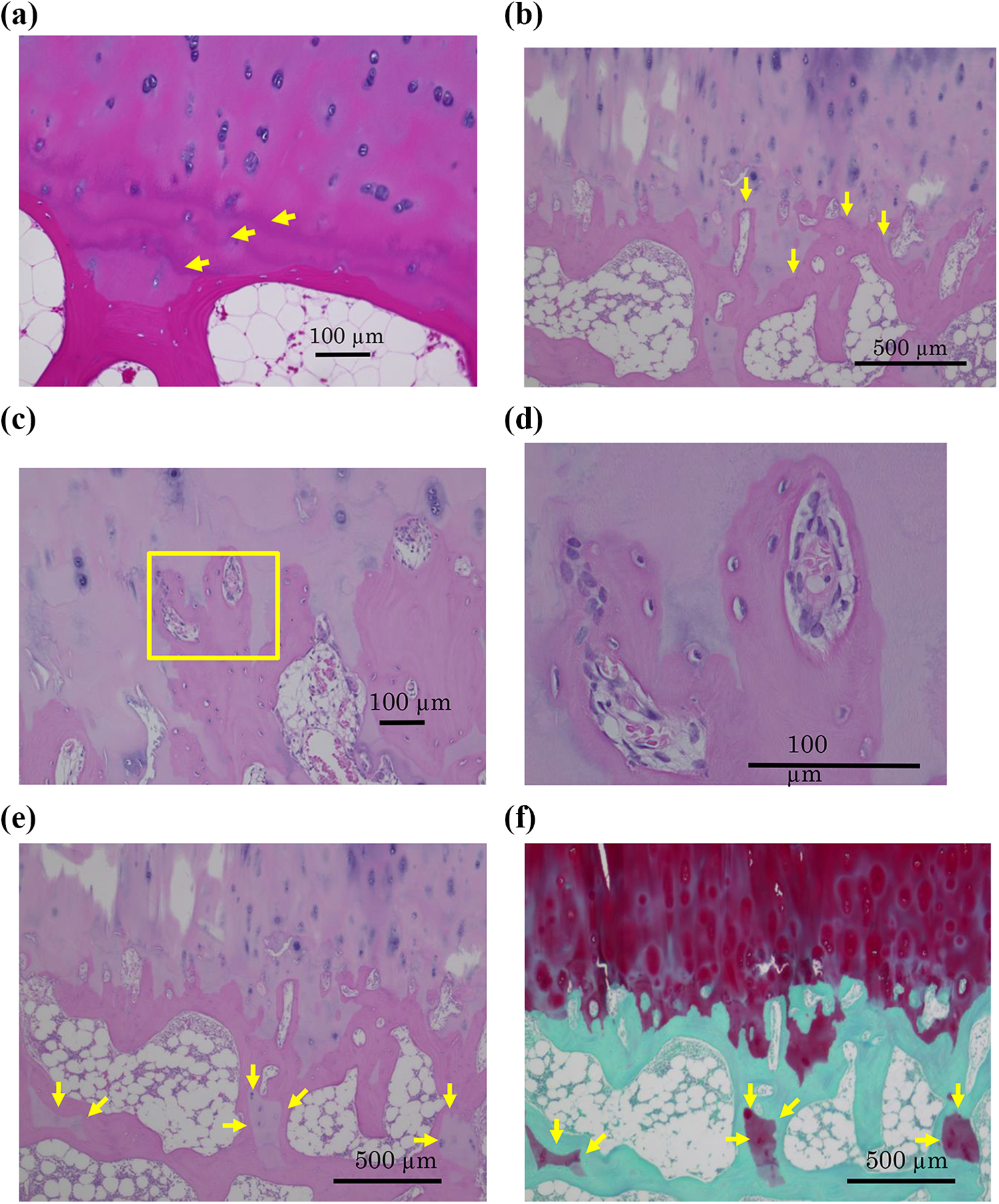
Multilayer tidemarks, irregular subchondral bone structure, and vascularization of the cartilage and calcification around the blood vessel and cartilage inside the subchondral bone in CTA. (a) H&E staining of a humeral head with cuff tear arthropathy (magnification ×100). Bar: 100 μm. Multilayer tidemarks (arrows) were observed in 12 (80%) of 15 shoulders. (b) H&E staining of a humeral head with CTA (magnification ×40). Bar: 500 μm. Irregular subchondral bone structure (arrows) was observed in 8 (53%) of 15 shoulders. (c) and (d) H&E staining of a humeral head with CTA. Vascularization of the cartilage and calcification around the blood vessels were observed in 4 (27%) of 15 shoulders. Bars: 100 and 500 μm, respectively. (e) and (f) H&E and Safranin-O staining of a humeral head with CTA. Cartilage inside the subchondral bone (arrows) was observed in 7 (47) of 15 shoulders. Bars: 500 μm. CTA: cuff tear arthropathy; H&E: hematoxylin and eosin; OA: osteoarthritis
Discussion
In the present study, we evaluated the histopathological findings of the humeral head in CTA cases compared with glenohumeral OA cases (non-cuff tear controls). In the CTA group, different macroscopic and histopathological findings were observed between the superior and middle parts to the inferior part of the humeral head; thickening of the cartilage, multiple clusters of chondrocytes, and a larger stained zone were observed in the middle area of the humeral head. However, the entire humeral head in both the CTA and glenohumeral OA groups showed similar severe damage. The average maximum thickness of the cartilage in the CTA group was 2.19 mm, and the radial and calcified zones were particularly thickened. Hodler et al. 11 reported that the mean thickness of the cartilage of the humeral head in normal cadavers was 1.23 mm. We demonstrated that the cartilage in the middle area of the humeral head in the CTA group was thicker than that in the gleno-humeral OA group (non-cuff tear controls). The cartilage layer of the CTA group tended to be thicker than that of the humeral neck fracture group. However, there was no statistical difference in cartilage thickness between CTA and humeral neck fracture.
In a previous study, synovitis was correlated with enlargement of the femoral head and thickening of the cartilage in the hip joints of rabbits from 27 to 31 days. 12 Other studies have shown that inflammation or reactive hyperemia in the hip joint would be expected to cause coxa magna. 13,14 In addition, another investigation has revealed that biochemical markers such as matrix metalloproteinase (MMPs), MMP-1, MMP-2, MMP-3, and MMP-13 in the synovial fluid were more enhanced in the rotator cuff tear group than in the nonrotator cuff tear group. 15 In the present study, synovitis or increased in synovium in the CTA cases was not investigated. However, these findings suggest that chemical mediators released by the synovium might be involved in the cartilage layer thickening seen in CTA.
OA changes in the superior area of the humeral heads and thickening of the cartilage layer from the middle to the inferior area of the humeral heads in CTA were confirmed histopathologically, suggesting that simultaneous mechanical and nutritional factors might be contributing to CTA pathogenesis. Most of the bony changes and subsequent cartilage changes in the CTA cases are consistent with biomechanical environment response to Wolff’s law. 16 Increased stress concentration in the superior part of the humeral head by rotator cuff tear might cause the thickening of the cartilage layer in CTA cases. Meanwhile, nutritional factor and inflammatory cytokine from the bone marrow through osteoarthritic change following cuff tear might cause the cartilage layer thickening of the humeral heads.
In this study, in cases with CTA, more thickening of the cartilage layer and deeper Safranin-O-stained zones were observed in the middle of the humeral heads of CTA cases than those of the OA and four-part fracture cases. Moreover, tidemarks crossed by blood vessels were observed in CTA cases. Angiogenesis in the cartilage causes calcification of the cartilage layer during growth period. Therefore, this angiogenesis suggests that calcifications occur in the cartilage layer in CTA cases. This repeated angiogenesis phenomenon might cause cartilage layer thickening of the humeral head in CTA cases.
In rat cuff tear models, the cartilage layer got thinner and decreased in Safranin-O staining. 10 In the knee joints of mice with anterior/posterior and medial/lateral transection, the cartilage tissue extended from the posterior direction and gradually showed increased Safranin-O staining and the tissue had developed osteophytes through endochondral ossification. 17 Cartilage changes varied among the four-legged walking animal joints. In our study, increased Safranin-O staining was found in the calcified zone in the CTA group, and multilayer tidemarks in the deep layer of the cartilage, vascularization of the cartilage, and calcification around the blood vessel were also observed in some cases. Cartilage changes in human humeral head were quite different from experimental animal models.
Lane and Bullough 18 reported that the change from noncalcified cartilage to calcified cartilage emerged by duplication of the tidemark. In the nonpressure area of the hip, the calcified zone increases in thickness and darker-stained bands within the calcified zone increase in number according to depth. 19 In patients treated with high tibial osteotomy (HTO) or knee joint distraction, median joint cartilage width was increased on radiographs due to median decompression. 20
As the process continues, the subchondral blood vessels enter the calcified zone and progress toward the joint’s surface, which is consistent with our data, showing that the duplication of the tidemark and ossification in the deep layer of the cartilage appeared in the CTA group.
The current study has some limitations. First, the diameter of the affected humeral heads among the three groups was not evaluated in the current study. However, our previous reports have found that the diameter of humeral head in CTA cases was larger than that of the contralateral side. Therefore, thickening and calcification of the cartilage might be causing the humeral head enlargement observed in CTA. Second, we did not evaluate the immune response or nutritional factors in the current study. Therefore, further investigations regarding immune response or nutritional factors to CTA pathogenesis should be performed. However, our data showed that OA changes in the superior area of the humeral heads and thickening of the cartilage layer from the middle to the inferior of the humeral heads occurred in CTA, suggesting that simultaneous mechanical and nutritional factors might be contributing to CTA pathogenesis.
Conclusion
The middle to the inferior area of the articular cartilage of the humeral head was thickened in CTA compared with that in glenohumeral OA, which suggests that thickening and calcification of the cartilage might be causing the humeral head enlargement observed in CTA.
OA changes in the superior area of the humeral heads and thickening of the cartilage layer from the middle to the inferior area of the humeral heads in CTA were confirmed histopathologically, suggesting that simultaneous mechanical and nutritional factors might be contributing to CTA pathogenesis. The current study provided the better understanding of cartilage damage and thickening in CTA. This will help guide treatment options in the setting of CTA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.