
Abstract
Current guidelines on the management of hip and knee osteoarthritis (OA) do not compare safety of treatment modalities. We therefore systematically reviewed 20 studies investigating mortality and serious complications of both medical and surgical treatments for hip and knee OA using PubMed, Scopus, Web of Knowledge and Google Scholar. Mortality was the highest for naproxen (hazard ratio (HR) = 3 (1.9, 4.6)) and lowest for total hip replacement (relative risk (RR) = 0.7 (0.7, 0.7)). Highest gastrointestinal complications were reported for diclofenac (odds ratio (OR) = 4.77 (3.94, 5.76)) and lowest for total knee replacement (HR = 0.6 (0.49, 0.75)). Ibuprofen had the highest renal complications (OR = 2.32 (1.45, 3.71)), whereas celecoxib had the highest cardiovascular risk (OR = 2.26 (1, 5.1)) and lowest was for tramadol (RR = 1.1 (0.87, 1.4)). Results show that medical management of hip and knee OA, particularly with non-steroidal anti-inflammatory drugs, may carry higher mortality compared to surgery. Careful consideration should be given to medical management taking into account known co-morbidities.
Keywords
Introduction
Osteoarthritis (OA) is one of the largest contributors in the elderly population to pain, functional impairment and reduced independence. 1 Of the large joints, the hip and knee are the most commonly affected. 2 Although the causes of primary OA are not fully established, numerous studies have indicated a genetic basis, and, in the case of primary hip OA in young and middle aged adults, femoroacetabular impingement has recently been recognized. 3
A number of treatment options are available. Conservative measures include aerobic exercise, local muscle strengthening, weight loss, education, shock-absorbing footwear and oral analgesics such as paracetamol and non-steroidal anti-inflammatory drugs (NSAIDS). Intra-articular corticosteroid injections and arthroplasty are the two available more invasive options. Current treatment strategies including the The National Institute for Health and Care Excellence (NICE) pathway for OA recommend a step-wise approach where such options are reserved for patients with symptoms refractory to non-surgical treatments. 4
Although established on evidence-based methods, the published guidelines do not take into account the safety of various treatment modalities. Studies have shown that patients’ willingness to opt for surgery is generally low, 5 and this may represent misperceptions among patients regarding the safety of surgery compared to medical management as well as the recommendation from current guidelines, which state that arthroplasty should be offered to patients in whom medical treatment has failed. Mortality and serious complications risk is important in the choice of treatment, and to date, there are no studies comparing the safety of arthroplasty to medical treatments. We therefore aimed to systematically review the published evidence on the mortality and risk of serious complications of various treatments for hip and knee OA. We assessed the quality of the included studies and quantified the overall risk for each treatment modality to inform treatment choice.
Materials and methods
This systematic review was performed according to the review protocol defined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (www.prisma-statement.org/).
Eligibility criteria
Studies investigating the safety of total knee replacement (TKR), total hip replacement (THR), arthroscopy, opiods, NSAIDS, paracetamol, chondroitin sulphate and glucosamine were evaluated in the study. The articles also had to be a full report of a clinical study published in the peer-reviewed literature after 1960. Review articles (other than meta-analysis), meeting abstracts, case reports, bulletins, letters, comments and studies not reporting quantified results, smaller studies (recruiting less than 1000 patients), studies of risk prevalence with no control group, studies reporting short-term outcomes (<60 days) and studies of mild complications or side effects were excluded from the study. Treatments within studies that have been withdrawn from the market for safety concerns were excluded from the final analyses.
Information sources and search
In October 2016, a literature search for relevant articles was performed using PubMed, Scopus, Web of Knowledge and Google Scholar. We restricted the search to articles between January 1960 and October 2016. Initial searches were performed using the phrase: ‘osteoarthritis treatment’ to identify common treatment modalities. The treatments ‘total knee replacement’, ‘total hip replacement’, ‘arthroscopy’, ‘opioids’, ‘non-steroidal anti-inflammatory drugs (NSAIDS)’, ‘paracetamol’, ‘chondroitin sulphate’, ‘glucosamine’ and ‘propoxyphene’ were searched and then combined using Boolean connectors (‘OR’ and ‘AND’) with ‘serious complications’, ‘mortality’, ‘gastrointestinal risk’, ‘renal risk’, ‘cardiovascular risk’ and ‘infection’(see Online Supplemental Material A, which lists the full PubMed search strategy). Additional citations were found by assessing the references contained within each article. Articles not available online were retrieved from the Royal Society of Medicine Library or from the British Library.
Study selection and data collection
Search results were assessed jointly by two authors (OA and AS) to identify the potentially relevant articles, and any conflicts were resolved by discussion until there was 100% conformity on which studies to include.
Data items
The data obtained from each study included study design, exposure duration, dosage, number of patients and number of controls. Odds ratios (ORs), relative risks (RRs) and hazard ratios (HRs) were also noted from each study or calculated in studies providing the data.
Assessing the quality of evidence
The quality of studies was assessed based on the approach used by the American Academy of Orthopaedic Surgeons (AAOS) in judging the quality of treatment studies. 6 This two-step process involves firstly assigning all data presented in meta-analysis or randomized controlled trials (RCTs) as level I evidence. Results presented in non-RCTs and other prospective studies were initially categorized as level II, those in retrospective comparative and case-controlled studies were categorized as level III, and results in case-series reports were categorized as level IV. For studies other than meta-analysis, each outcome was then assessed using the AAOS’ quality questionnaire for treatment studies and when quality standards were not met, the final level of evidence (LOE) was downgraded by one (see Online Supplemental Material B, which includes a copy of the quality questionnaire).
Quantifying risk
The risks for five groups of adverse events were presented for each treatment modality: mortality risk, serious gastrointestinal (GI) complications risk, serious renal complications risk, serious cardiovascular (CV) complications risk and infection risk. If more than one study was identified reporting a certain treatment modality adverse event, the one with the highest LOE was included in the overall ‘risk score’ calculation. Mortality risk was made to weigh more heavily than infection, serious CV, GI and renal risk. This was done by multiplying the mortality HRs by 10 and adding this value to the serious CV, GI renal and infection RRs, ORs or HRs to give the overall risk score. The treatments were then graded for overall risk by creating a simple schematic for both patient and clinicians to aid treatment choice. Treatments scoring between 12 and 24 were graded as ‘high risk’, those scoring between 0 and 12 were graded as ‘low risk ‘and those scoring less than 0 as ‘no risk’.
Results
Study selection
In total, the search strategy identified 24,110 potentially relevant articles, with a further 10 being identified once references from relevant studies were reviewed. Duplicates were removed, giving a total of 12,109 articles. Of these, 11,529 articles were excluded from analysis after review of the title/abstract. Of the remaining 580 studies, a further 560 were excluded after reviewing the full text (see Figure 1). Therefore, 20 studies were finally included in the review.

Study selection process.
Study characteristics and results synthesis
The characteristics of the studies included are presented in Table 1. The control population was mentioned in 11 of the 20 papers. Age ranged from 25 years 27 to 79 years. 22 All patient populations were control matched for age, gender and co-morbidities. Exposure to the various treatments ranged from 60 days to 12.7 years. The studies varied in the serious complications for each treatment. The authors identified 15 relevant treatment modalities for OA. The StatsDirect software package (version 3) was used to create the various forest plots (see Figures 2 to 6). With regard to mortality, naproxen had the highest risk (HR = 3 (1.9, 4.6)), 7 whereas THR had the lowest (RR = 0.7 (0.7, 0.7)), 20 followed by TKR (HR = 0.79 (0.66, 0.92)) 21 (see Figure 2). Arthroscopy had a relatively low mortality risk (HR = 0.96 (0.04, 5)). 23
Summary of studies.

NP: not provided; P: prospective; R: retrospective; THR: total hip replacement; TKR: total knee replacement; TJR: total joint replacement; LOE: level of evidence; OR: odds ratio; HR: hazard ratio; RR: relative risk.
a Meta-analysis.
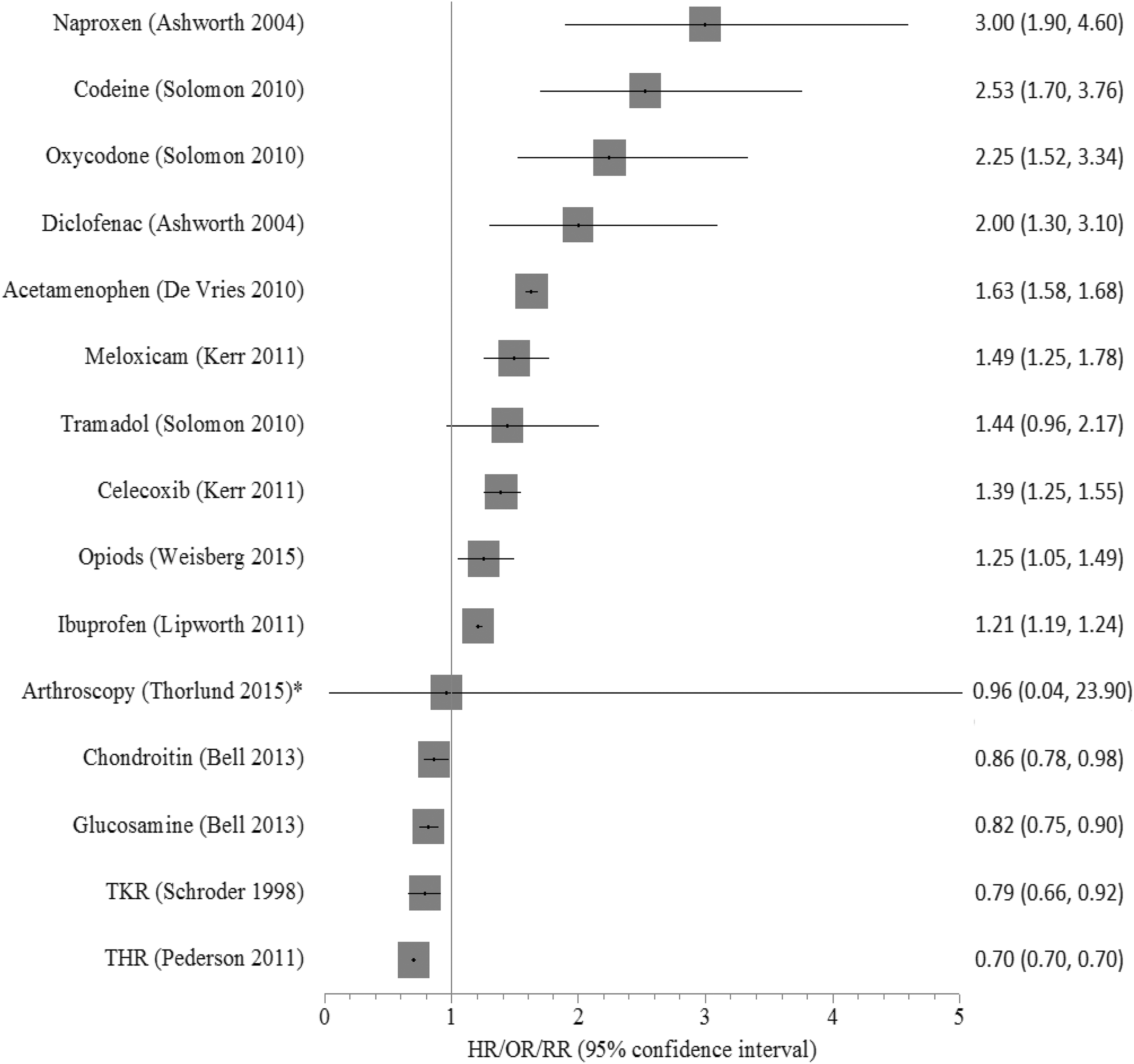
Forest plot showing mortality following intervention for OA. Asterisk indicates arthroscopy upper confidence interval limited to five for graphical purposes. OA: osteoarthritis; TKR: total knee replacement; THR: total hip replacement.

Forest plot showing cardiovascular complications following intervention for OA with 95% CI. OA: osteoarthritis; CI: confidence interval.

Forest plot showing GI complications following intervention for OA with 95% CI. GI: gastrointestinal; OA: osteoarthritis; CI: confidence interval; TKR: total knee replacement; THR: total hip replacement.

Forest plot showing renal complications following intervention for OA with 95% CI. OA: osteoarthritis; CI: confidence interval.

Forest plot showing infection complications following invasive intervention for OA. OA: osteoarthritis; TJR: total joint replacement.
The most hazardous treatment with regard to CV risk profile was celecoxib (OR = 2.26 (1, 5.1)), 9 while conversely the least hazardous was tramadol (RR = 1.1 (0.87, 1.4)) 22 (Figure 3). There was no published evidence on serious CV complications following TKR based on our inclusion criteria. The most hazardous treatment in terms of GI risk was diclofenac (OR = 4.77 (3.94, 5.76)) 24 (Figure 4). Arthroplasty, however, was the least hazardous and in fact protective with THR and TKR having a risk of HR = 0.9 (0.87; 0.99) and HR = 0.6 (0.49, 0.75), respectively. 20 Ibuprofen had the highest renal complications risk (OR = 2.31 (1.45, 3.71)), 14 whereas celecoxib was protective (OR = 0.61 (0.4, 0.94)). 26 There was no published evidence on serious renal complications following total joint replacement (TJR), arthroscopy or opioids based on our inclusion criteria. TJA had the highest infection risk (OR = 15 (4.1, 54.3), followed by arthroscopy (OR = 5.1 (2.2, 11.9)) and then intra-articular injection (OR = 1.24) 16 (Figure 6).
Risk of bias and quality of evidence
Most of the 20 studies included were initially graded as level III. However, using the quality assessment tool for treatment studies (see Online Supplemental Material B), the final adjusted LOE was predominantly level IV (see Table 2).
Quality scores.

LOE: level of evidence; Y: yes; N: no; NA: not applicable.
Quantifying risk
Based on the process outlined in the Methods section, an overall ‘risk score’ for each treatment is presented in Figure 7. Naproxen had the highest risk, whereas glucosamine was the safest.

Combined risk score for each treatment modality. TKR: total knee replacement; THR: total hip replacement; COX: cyclooxygenase.
Discussion
Although there is no known cure for OA, various treatments are available to reduce pain, minimize functional impairment and improve joint mobility. Taking into account its mortality and GI, CV and renal complications risk, naproxen had the highest overall risk score. A recent network analysis of the effectiveness of NSAIDS for the treatment of pain in knee and hip OA found a significant linear dose effect for naproxen in improving OA pain. 28 Our findings concur with the authors’ caution that despite this, physicians need to take into account the safety profile of NSAIDS when selecting pharmacological therapies for OA. The authors also identified 150 mg/day of diclofenac to be the most effective in terms of pain and physical function. We found diclofenac, however, to have the third highest overall adverse event risk score and the most harmful in terms of GI complications risk. Its role in GI injury is believed to be related to the inhibition of cyclooxygenase (COX), resulting in the inhibition of prostaglandin which has important roles in maintaining homeostasis of GI mucosa. 29
Both glucosamine and chondroitin had the lowest overall adverse event risk score. A Cochrane review supports this finding concluding that glucosamine therapy is well tolerated with a safety profile similar to placebo and significantly better than NSAIDs. 30 Controversy exists, however, around the efficacy of these drugs. Although some patients feel that they are beneficial, 31 a meta-analysis in 2010 of 10 large-scale randomized controlled trials found that glucosamine, chondroitin and their combination neither result in reduced joint pain nor affect joint space narrowing compared with placebo, 32 findings supported by NICE in their recent systematic review and recommendations. 4 In terms of adverse event risk, we found no evidence for serious GI, renal and CVS complications. Instead, we noted a reduced risk of mortality compared with patients who never use the drug according to a large prospective cohort study by Bell et al. 33 Laboratory and human studies suggest that glucosamine and chondroitin are associated in reducing inflammation by possibly inhibiting the transcription factor, nuclear factor kappa B (NF-κB), which is involved in inflammatory processes from translocating to the nucleus. 34 Inflammation has been linked to several diseases including cancer and chronic obstructive pulmonary disease, and this may account for the reduced mortality risk found with glucosamine or chondroitin use. 33 The authors did control for numerous predictors of mortality. However, there is still the possibility of bias from confounding as glucosamine and chondroitin use is associated with several positive health behaviours.
Although having a low combined adverse risk score when compared to the non-steroidals naproxen and diclofenac, acetaminophen (paracetamol) was reported to have the second highest risk for renal and CV complications and third for GI complications. A network meta-analysis of 137 RCTs on the effectiveness of pharmacological interventions for knee OA published last year found that naproxen, ibuprofen, diclofenac and celecoxib were significantly superior to acetaminophen in terms of pain and functional-related outcomes. 35 Paracetamol was the only analgesic that did not meet the criteria for clinically significant improvement. 35
Taking into account its low relative effectiveness and high risk for renal and CV complications, paracetamol prescription as a first-line treatment for OA should therefore not be recommended. The same meta-analysis also identified intra-articular hyaluronic acid (IAHA) as significantly superior to intra-articular (IA) corticosteroids and as having the greatest effect size of all pharmacological interventions in terms of function-related outcomes at 3 months. 35 Its higher cost though, combined with a recent double blind RCT showing no clinical superiority to corticosteroid injections suggest that controversy will still exist around the ideal intra-articular injection for OA. 36 Nevertheless, we found intra-articular injections to be a safe overall intervention ranking third when compared to the other interventions reviewed.
Charnley revolutionized the management of OA with the development of low-friction hip arthroplasty in 1962. 37 Excellent survivorship and THR’s widely recognized capacity to improve pain, quality of life and function, led authors to conclude that ‘total hip arthroplasty might be the operation of the century’. 38 Gunsten applied Charnley’s principles to the knee replacement and with the development of newer designs, its effectiveness has also become recognized. 39 Despite the good outcomes, less than 15% of patients with clinically and radiologically severe arthritis are willing to undergo arthroplasty. 5 This emphasizes a potential perception among patients of high risk associated with surgery. We found both total hip and knee arthroplasty to be ‘low risk’ when compared to other treatment modalities for hip and knee OA. Taking into account mortality and infection risk as well as major CVS, renal and GI complications risk, arthroplasty was safer than some commonly used pharmacological treatment modalities including naproxen, codeine, diclofenac and oxycodone. In terms of mortality, THR and TKR had the lowest reported risk of all 15 treatment modalities including glucosamine and chondroitin. This may be explained by the careful selection of patients for surgery. However, studies reporting low mortality risk in arthroplasty matched cases and controls for age, sex and co-morbidities reducing potential selection bias. 20,21 It is difficult to ascertain fully the effects of surgery, although it is possible that its protective effect may be secondary to the reduced use of high-risk pharmacological analgesics as well as a return to a more active lifestyle. With more widespread use of low-molecular-weight heparins (LMWHs), the trend to shorter hospital stays, safer anaesthesia and more accelerated post-operative rehabilitation programmes further drops in mortality risk may be published in the future.
Limitations of our study
Although most major complications of arthroplasty were considered in our risk analysis, we did not take into account several other notable complications. The UK’s National Joint Registry in 2015 reported that the risk of revision for primary total hip replacements at 11 years was 3.63% for all cemented procedures with dislocation, fracture or infection being the commonest reason for revision within the first year and implant loosening or pain being the commonest after 5 years. 40 The reported 11-year revision rate for cemented primary knee replacements was very similar at 3.62%. 40 In terms of satisfaction, it is reported that 7–32% of the patients are dissatisfied after their TKA, 41 whereas the figure is slightly lower for THA at 7–15%. 42 Stiffness is another recognized complication of TKA with an incidence of between 1% and 13%. 43
Conclusion
Long-term medical management of hip and knee OA particularly with some NSAIDS may carry a higher long-term risk of serious complications compared to surgery. In terms of mortality, there is evidence that arthroplasty as well as glucosamine and chondroitin are protective; however, controversy exists around the analgesic efficacy of the latter. We therefore recommend that the practitioner and patient should carefully consider the risks of medications and not just surgery prior to commencing treatment. When opting for medical management, we recommend a combination of ‘low-risk’ analgesics. Moreover, treatment choice should be tailored to the patient taking into account known GI, CVS and renal co-morbidities (see Figures 3 to 5). Patients with known CV co-morbidities should be recommended tramadol or ibuprofen, whereas those with GI conditions can be prescribed tramadol. Patients with renal co-morbidities can be recommended celecoxib. Patients who are still symptomatic despite taking ‘low-risk ‘analgesics or who require regular ‘high-risk’ analgesics should be recommended surgery (see Figure 8).

Proposed step-wise management algorithm for hip and knee OA. OA: osteoarthritis; GI: gastrointestinal; PPI: proton pump inhibitor.
Supplemental material
OSJ808669_Supplementary_material - Treatment modalities for hip and knee osteoarthritis: A systematic review of safety
OSJ808669_Supplementary_material for Treatment modalities for hip and knee osteoarthritis: A systematic review of safety by Osama Aweid, Zakir Haider, Abdel Saed, and Yegappan Kalairajah in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.