
Abstract
Polyethylene (PE) remains the gold standard for the articulating surface in hip and knee arthroplasty. To increase arthroplasty longevity and improve wear resistance, newer versions of PE have been designed with resultantly different wear properties. Highly cross-linked polyethylene (HXLPE) is used in total hip arthroplasty with excellent outcomes; however, its use in total knee arthroplasty (TKA) remains conflicting. This review summarizes biomechanical and wear properties, clinical outcomes, and cost of polyethylene inserts in TKA. Simulation studies have convincingly shown decreased wear and oxidation rates with HXLPE when compared to conventional polyethylene (CPE). Registry results have been conflicting, and short- to midterm clinical studies have not demonstrated a significant difference between HXLPE and CPE. The cost of HXLPE inserts is higher than CPE. Long-term clinical data are lacking and further studies are warranted to evaluate the role of HXLPE in TKA.
Introduction
Ultrahigh molecular weight polyethylene (UHMWPE) is a manufactured subset of polyethylene (PE) with long carbon chains and properties that make it appealing for use in joint arthroplasty. 1 Due to its long chain structure, UHMWPE has a strong resistance to abrasion and high impact strength. It is biocompatible, provides a low-friction articulating surface, and can be manufactured relatively easily. For these reasons UHMWPE has been considered as the gold standard in total joint arthroplasties. 2,3 While UHMWPE is commonly used, there are several concerns with in vivo use. These include the negative effects of PE wear particles on joint tissues and implant longevity and potential fatigue wear and component fracture from oxidative degradation. 4
PE has been a common cause of knee arthroplasty revisions. 5 These implant failures are a result of wear particles on a submicron scale leading to periprosthetic inflammation and activation of phagocytosis. This can eventually lead to periprosthetic osteolysis and subsequent implant loosening. 3,6 Kim et al. reported 45% of total knee arthroplasty (TKA) failures in patients less than 55 years old were secondary to PE wear. 7 TKA is a high volume procedure and is projected to increase to 3.48 million performed annually by the year 2030. 8 It is prudent to reduce PE wear-related implant failures.
Materials
UHMWPE is the base material of both conventional polyethylene (CPE) and the more irradiated highly cross-linked polyethylene (HXLPE). Structurally, the material mimics the natural joint surfaces by maintaining an intermediate semi-crystalline and amorphous state. 9 CPE contains fewer cross-linked chains leading to the production of wear particles and osteolysis. In an attempt to decrease the PE wear particles created in CPE, first-generation HXLPE is irradiated to generate free radicals and then thermally treated to maximize free radical induced cross-linking. 5,9 –12 Free radical production increases wear resistance by cross-linking but is a more brittle PE, with decreased fatigue crack resistance and increased risk of crack propagation. 13 Additionally, the radiation needed to manufacture HXLPE reduces in vivo oxidative resistance and potential longevity. 10,11,14 –16
Second-generation HXLPE is manufactured by means other than a single irradiative and/or thermal treatment with the intent to decrease free radical oxidation while improving crack resistance and crystallinity. 11,17 –20 Common methods include sequential annealing and the addition of chemical anti-oxidants (primarily vitamin E) for improved free radical removal. 1,2,21,22 More recent attempts have been made to spatially limit cross-linking to the surface of the implant, maximizing overall toughness while decreasing surface wear rates. 23,24
Biomechanics and wear properties
The most common cause of TKA failure is related to consequences of PE wear debris. 25 Wear debris is generated via surface delamination and adhesive/abrasive wear of the PE insert. 26,27 Delamination is the result of compressive and tensile loads that lead to subsurface cracking of the PE. Cracks are formed just below the surface and propagate with further stress, leading to the release of flakes of material. Adhesive and abrasive wear occurs directly on articular surfaces. Free floating particles on a submicron scale induce inflammation and subsequent osteolysis, leading to aseptic loosening and periprosthetic fractures. 9 Free radicals within the insert can also lead to oxidative degradation of the PE, contributing to the delamination, adhesive, and abrasive wear of the PE. 26 –28
Many studies have compared the in vitro wear properties of CPE and HXLPE. First-generation HXLPE has been shown to generate smaller particles and lower wear rates as compared to CPE. 26,27,29 Second-generation HXLPE has demonstrated superior mechanical properties (fatigue crack resistance and crack propagation) when compared to first-generation HXLPE. 9,30,31 Specifically, the addition of vitamin E as an antioxidant in second-generation HXLPE demonstrated decreased wear rates, increased fatigue strength, and increased resistance to delamination. 28,32 –35
Clinical outcomes
TKA is a high volume, successful, and cost-effective treatment with emphasis on measurable health outcomes. 8,36 Unlike total hip arthroplasty, it is difficult to determine PE wear using postoperative radiography due to the unique weight bearing anatomy of the knee. 37 The most commonly studied outcome is TKA failure, which is ultimately defined by the need for a revision surgery. This provides useful data points such as patient characteristics, surgical technique, and implant style. However, this does not allow for reliable evaluation of insert performance and often underscores patient pain and function. 38,39 As there is no best method to measure TKA outcome and PE durability, additional study modalities are used for a more comprehensive comparative analysis of CPE or HXLPE. These designs have included retrieval studies of explanted PE inserts, PE particulate measurement in synovial fluid, prospective clinical studies, analysis of joint registries, and failure case reports.
Retrieval studies
Retrieval studies investigate retrieved PE implants, typically after a revision procedure or autopsy. 37 Published retrieval studies over the last 15 years have demonstrated no difference between CPE and HXLPE wear in early TKA revisions (Table 1). 6,40,41 These results are not entirely unexpected, since failure in these early revision cases is unlikely to be due to PE wear. However, these studies can serve as a comparative data point for future long-term studies. First-generation remelted HXLPE has been shown to have increased oxidation resistance compared to CPE. 42 Second-generation vitamin E HXLPE inserts have significantly improved in vivo and ex vivo oxidative resistance when compared to both first-generation HXLPE and CPE. 44,45
Summary of retrieval studies.
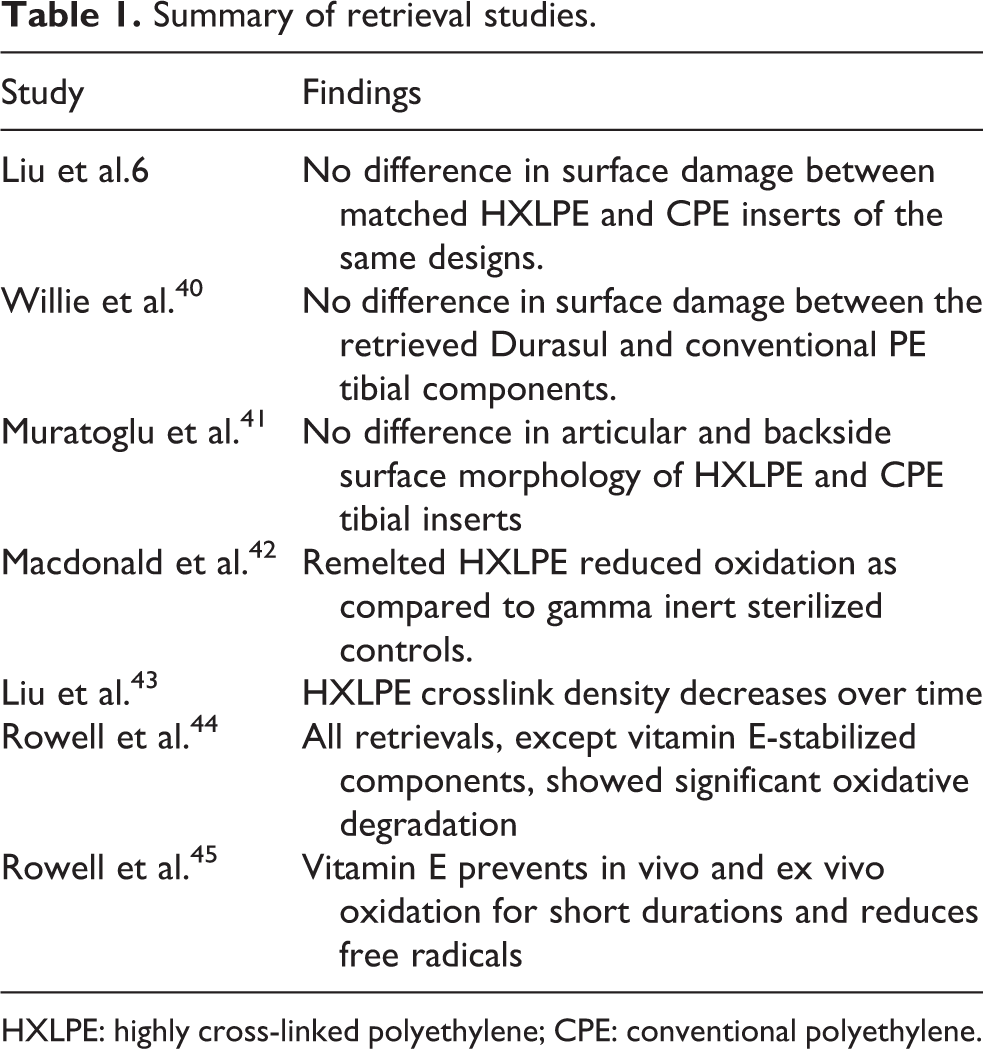
HXLPE: highly cross-linked polyethylene; CPE: conventional polyethylene.
PE particulate studies
PE particles are readily measured from both in vitro simulations and synovial fluid studies (Table 2) and contribute to osteolysis and aseptic loosening in TKA. 48,49 Higher quantities and more elongated particles appear to elicit a stronger inflammatory response. 18,50 Particulate size also plays a key role as particles smaller than 0.05 μm fail to activate a response, 43 and those larger than 10 μm are too large to be phagocytosed. 51,52 Most wear particles in TKA are approximately 1 μm in diameter. 46 Iwakiri et al. in 2009 and Hinarejos et al. in 2013 found in vivo wear particles as early as 1 year post TKA. 46,47 Their results were conflicting as Iwakiri et al. reported fewer, smaller, and more spherical particles in HXLPE, while Hinarejos et al. in a larger study found no significant difference in particulate quantity, size, and morphology between PE groups. 46,47
Summary of PE particulate studies.

PE: polyethylene; HXLPE: highly cross-linked polyethylene; CPE: conventional polyethylene.
Revision rates
Ten year revision rates for TKA have been reported to be approximately 5%, regardless of age. 38 Thus, a comparative analysis of PE with any significance requires mid- to long-term follow-up and a large cohort. 53,54 Yu et al. recently published a meta-analysis investigating PE function and failure rates. 55 Totally, six studies (three randomized clinical trials and three non-randomized clinical trials) were included with a follow-up period of 2–6 years (Table 3). 56 –60,64 Outcome measures included total number of operations, reoperations for prosthesis loosening, radiolucent lines, osteolysis, prosthesis loosening, mechanical failures related to tibial PE, postoperative total knee score, and functional scores. No significant differences were seen in any of the measured variables. 55 Similarly, other clinical studies also failed to find a significant advantage or disadvantage to using HXLPE over CPE. 61 –63 There remains a need for longer term follow-up to evaluate more definitively the effectiveness of HXLPE.
Revision rates studies.
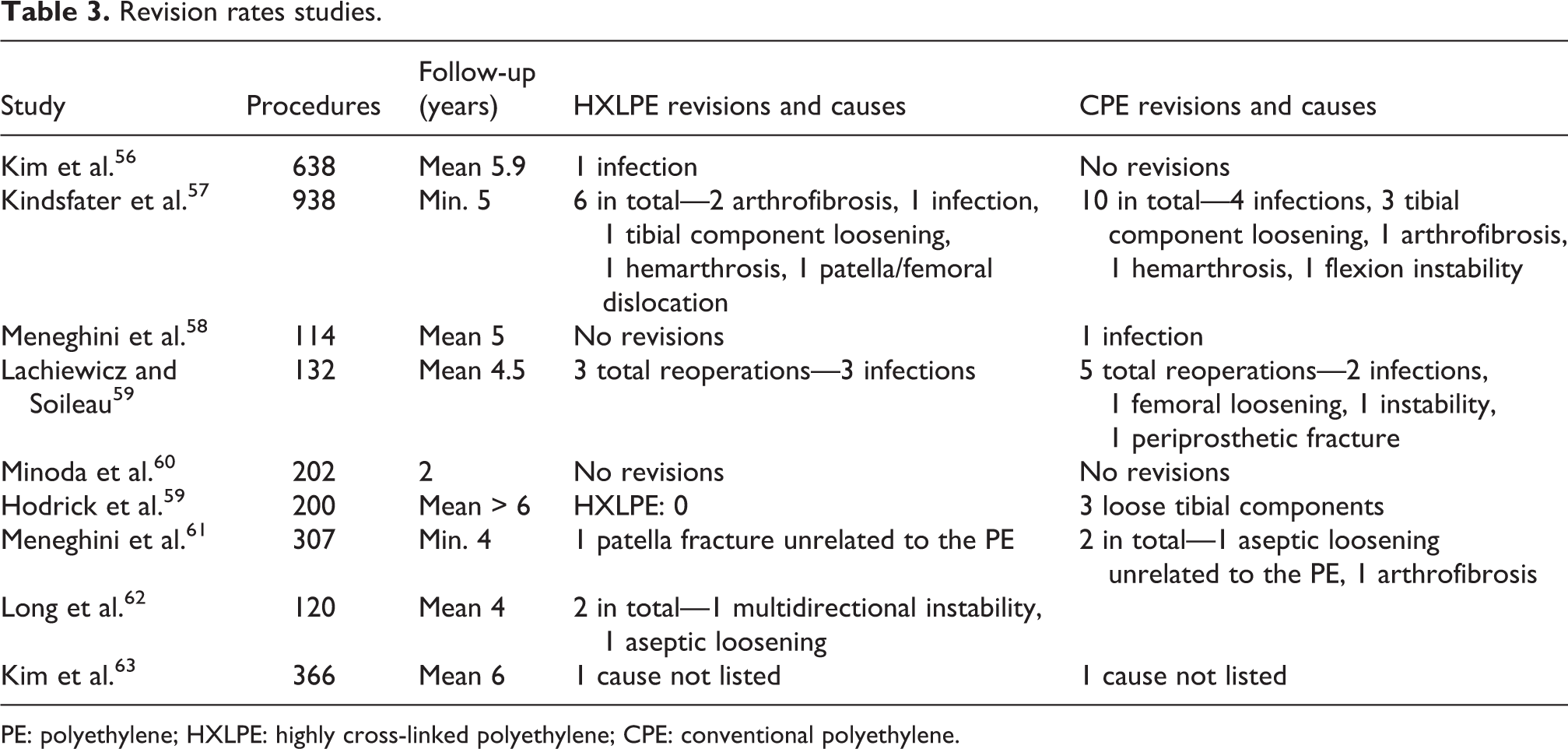
PE: polyethylene; HXLPE: highly cross-linked polyethylene; CPE: conventional polyethylene.
Joint registry studies
Joint replacement registry studies (Table 4) bypass the typical constraints seen in clinical trials of small sample sizes, study attrition, and lack of generalizability often seen with clinical research. 66 While this is useful, data are strictly limited to revision rates and patient demographics. 67 Inacio et al. reported no difference in revision rates in 62,177 TKA cases comparing HXLPE and CPE at a mean 2.8-year follow-up. 65 Paxton et al. similarly found no significant difference in revision rates between the two most popular HXLPE implants within the Kaiser Permanente Total Joint Replacement Registry, at a 5-year follow-up of 77,084 TKA cases. 66 Conversely, in a larger study of 386,104 TKA cases from the Australian Orthopedic Association National Joint Replacement Registry, HXLPE had overall and prosthesis specific reduction in 10-year revision rates when compared to CPE (5.8% vs. 3.5% revision rates at 10-year follow-up). 54 The overall reduction in revision rates in this study was mainly due to lysis and loosening and was most pronounced in patients under the age of 65. In general, age is the most relevant factor affecting outcome of TKA, as younger patients live longer, more active lives. 68,69
Joint registry studies.

HXLPE: highly cross-linked polyethylene; CPE: conventional polyethylene.
Safety
A concern with HXLPE has diminished fatigue fracture resistance 16 ; however, there are only a limited number of PE fracture case reports. 70 –74 In a large national registry containing over 300,000 TKA procedures, there were only two cases of PE fracture. 54 The literature has shown that HXLPE is as safe as CPE in TKA; however, due to the limited long-term data available, it is premature to make definitive conclusions. 53,54 Further, clinical studies with long-term follow-up are needed.
Cost
TKA is a highly beneficial and cost-effective procedure. 36 Patient outcomes demonstrate significant improvement in daily function and pain levels. 75 Even so, TKA carries a large cost to the US Healthcare system. In 2005, the overall cost for TKA in the United States exceeded US$11 billion. 76 The overall goal of cost analysis is to increase the value of a procedure, with value defined as health outcomes achieved per dollar spent. 77 Therefore, to increase the value of TKA, the longevity (outcome) of the implant would need to improve more than the increase in associated cost of HXLPE. Correlating outcomes with associated changes in cost is challenging. 75 Furthermore, the cost of implants is not standardized and varies greatly between hospitals, manufacturers, and geographic regions. Data from one hospital showed that the HXLPE insert costs US$150 more than CPE, 64 while others believe the price increase is higher. 67,78,79 The question can be asked then, what is the outcome needed to increase the value of a TKA by greater than US$150? Without data proving an increase in TKA life span, it is hard to justify the additional costs of HXLPE on such a high-volume procedure in all patients. HXLPE may be warranted in the younger population, as the increase in up-front costs may potentially decrease the need for revisions within the patient’s lifetime, 75,80 though definitive supportive data are currently lacking.
Conclusion
Currently, there is no definitive evidence that HXLPE outperforms CPE clinically in TKA. While simulation studies have convincingly shown decreased wear and oxidation rates in HXLPE, registry results have been conflicting and short- to midterm clinical studies have not demonstrated a significant difference between HXLPE and CPE. Further investigation with longer term studies is warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.