
Abstract
Purpose:
Modern hip stem design includes a prosthesis that has a predictable outcome in all total hip arthroplasty (THA) patients, regardless of approach, surgeon or patient characteristics. Introduction without a learning curve and, in cases of problems, the possibility for a simple revision are other prerequisites. The purpose of this study is to evaluate whether the Accolade TMZF stem (Stryker Orthopedics, Mahwah, New Jersey, USA) is suitable to fulfil these demands. We report our mid-term survival of the Accolade TMZF hip stem in all patients from the first implantation at our institute.
Methods:
From the start of using the Accolade TMZF stem (March 2009) until February 2011, 937 THA were performed by 12 surgeons using a posterolateral or anterolateral approach. Survival of the stem was calculated using Kaplan–Meier analysis. Effect of approach, patient age and comorbidity were analysed with a Cox proportional hazards’ model. The learning effect was determined by comparing the number of revisions in the surgeons’ first 20 THAs with their next 30 THAs and the subsequent THAs.
Results:
At 5 years, cumulative stem survival was 97.9% based on revisions for all reasons and 98.8% with aseptic loosening as endpoint. We found no effect of surgical approach, patient age or comorbidity on stem survival. No learning effect was found.
Conclusion:
The Accolade TMZF stem fulfilled the demands of modern stem design.
Introduction
It has been proven that total hip arthroplasty (THA) improves quality of life for patients. 1 –3 Worldwide, both cemented and uncemented femoral stems are being used in THA. Studies concerning survival of these stems have shown varying results, and so far no technique can be considered superior to the other. 4,5 Lettich et al. stated that the challenge is to design a prosthesis that (1) has longevity in all patient groups, regardless of age and activity level, (2) can be implanted with relative ease and has a small learning curve, (3) minimizes bone loss and (4) has a predictable outcome with little complications. 6 In our opinion, a fifth criteria can be added in stating that any revision of a femoral stem should be as easy as possible, without adding further damage to the femoral bone.
An uncemented tapered stem with reliance on metaphyseal fixation, introduced with minimal reaming and broaching to minimize bone loss, may fulfil all of these conditions. A titanium stem provides a progressive transition from the bulky and relatively inflexible proximal segment to the finer and more flexible distal section. This permits loading of the proximal femur and protects against the effects of stress shielding. 6 Proximal hydroxyapatite (HA) coating in uncemented hip stems allows for a biological and better proximal fixation compared to proximal porous stems. 6 –10 Multiple studies have shown favourable outcomes in patients of all ages. 11 –13 In contrast, data from the national hip registries from Sweden and Denmark showed similar outcomes between these stems and debated whether an HA coating is truly needed to improve long-term survival in specific well-functioning uncemented femoral stem designs. 14 –16
The Accolade TMZF (Stryker Orthopaedics) is made of a β-titanium alloy (titanium–molybdenum–zirconium–iron) that better approximates the elastic modulus of bone, providing increased flexibility and greater tensile strength compared to other uncemented, tapered stems. 17 These features should provide the patient with a hip that better resembles the feel and functionality of natural bone. 4 The reduced modulus of elasticity, although still several times that of bone, should have a beneficial effect on stress shielding. 6 The Accolade femoral stem has a trapezoidal neck that should allow for improved ROM and may reduce the occurrence of instability. Proximal circumferential plasma spray and a PureFix HA coating should allow for a reliable mechanical engagement in bone.
Until now, only a few studies are available in the literature concerning the Accolade TMZF stem, reporting good clinical and functional outcomes together with an excellent mid-term (5–9 years) survivorship of 99.4–100% with aseptic loosening as endpoint. 6,9,10,13 However, despite these excellent survival rates in the literature, there are also concerns regarding the use of uncemented stems in general. 5,18 For this specific Accolade TMZF stem in particular trunnion wear, 19 –21 dissociation between femoral head and stem trunnion, 21 fractures of the neck of the stem 22 and more important high incidence of early migration with subsequent higher chance of aseptic loosening 23,24 were reported.
The primary goal of the current study is to investigate whether the mid-term survival of the uncemented tapered Accolade TMZF stem (minimal follow-up of 5 years) implanted in a large cohort of patients in a non-designer and non-academic teaching hospital was comparable to the outcome presented by the designer or specialized hip centres. As secondary outcome measures, we analysed whether age, comorbidity or surgical approach is associated with the outcome. The potential effect of a learning curve was calculated by including the entire series in our hospital including the first stem placements.
Methods
Patients
All patients undergoing a primary THA with an Accolade TMZF stem (Stryker Orthopedics; X-ray shown in Figure 1) from March 2009 (start of the use of the Accolade TMZF stem in our hospital) until February 2011 (to report at least 5 year follow-up) are included in the current study. The Accolade TMZF stem was used as a primary stem in all patients regardless of age or ASA grade. Only a small cohort of THA (n = 44) including the first experience with the direct anterior approach was excluded, because the implementation of the anterior approach has a learning curve of its own. 25 In this period, we performed 937 primary THAs in 881 patients. No patients were lost to follow-up. We prospectively follow all our patients in a local database. To ascertain correct survival data, we checked the national population registry for patient mortality and prosthesis data from the institute can be verified from the nationwide arthroplasty registry (LROI). Patient demographics showed 574 females (65.2%) and 307 males (34.8%) with a mean age of 70 years (range 23–95). ASA classification showed 18.4% ASA 1, 58.8% ASA 2, 22.3% ASA 3 and 0.5% ASA 4 patients. Major indication for the procedure was osteoarthritis of the hip joint in 822 patients (87.7%), followed by acute hip fracture (n = 53, 5.7%), osteonecrosis of the femoral head (n = 23, 2.5%), late post-traumatic deformity (n = 18, 1.9%) and miscellaneous (n = 21, 2.2%).

Accolade TMZF stem. An X-ray of the Accolade TMZF stem, which is discussed in the current study.
Surgery
Procedures were done by 12 different orthopaedic surgeons, performing a median of 59 THAs (range 1–255). Five surgeons performed over 100 THAs (range 103–255).
Two different surgical approaches were used: the anterolateral approach (n = 75, 8%) and most frequently the posterolateral approach (n = 862, 92%). The stems were used in combination with an uncemented Trident HA coated cup (Stryker Orthopedics) in 890 cases, a cemented RimFit cup (Stryker Orthopedics) in 36 cases and an Avantage double mobility cup (Biomet, Warsaw, Indiana, USA) in 11 cases.
Analyses
Analyses were performed using SPSS 19.0 (IBM SPSS Statistics, Armonk, NY). Survival of the stem was determined using the Kaplan–Meier survival analysis. A Cox multiple regression model was used to assess the effect of type of surgical approach, age and comorbidity on the survival rate. Endpoints were any change or removal of the stem for either ‘aseptic’ or ‘for all reasons’ in case of the Kaplan–Meier analysis and ‘for all reasons’ in the Cox regression. Deaths without revision were treated as censored data (with censoring the date of death). Kaplan–Meier survival data were used to construct the survival probabilities, with 95% confidence interval (CI). The factors studied with the Cox model were surgical approach (posterolateral, anterolateral), age group (less than 65, 65–75, greater than 75 years) and severity of comorbidity (ASA classification grades ‘I’, ‘II’ and ‘III and IV’). The Wald test was used to test the resulting estimated hazard ratios.
To evaluate the effect of a learning curve, we compared the number of revisions between the first 20 THAs of each surgeon, the subsequent 30 THAs (21–50) and the remaining THAs (>50). A χ 2 test was used to compare the number of events between these three groups. A p value of <0.05 was considered statistically significant.
Results
At 5 years, the cumulative survival of the stem was 97.9 (95% CI: 96.9–98.9) with endpoint revision for all reasons and 98.8 (95% CI: 98.0–99.5) with aseptic loosening as endpoint (Figure 2). No independent associations with survival of the stem were found for age, comorbidity and surgical approach (Table 1). We revised 21 Accolade TMZF stems. Main reason for femoral revision was aseptic loosening of the stem (n = 12, 57.1%) followed by periprosthetic fracture (n = 6, 28.6%), recurrent dislocation (n = 1, 4.8%), deep infection (n = 1, 4.8%) and pseudotumour formation as a result of trunnion wear in one case (n = 1, 4.8%). For revision surgery, we used another primary stem (Exeter cemented or Accolade TMZF uncemented stem) in 13 cases and a modular long stem (restoration modular hip stem) in 8 cases.
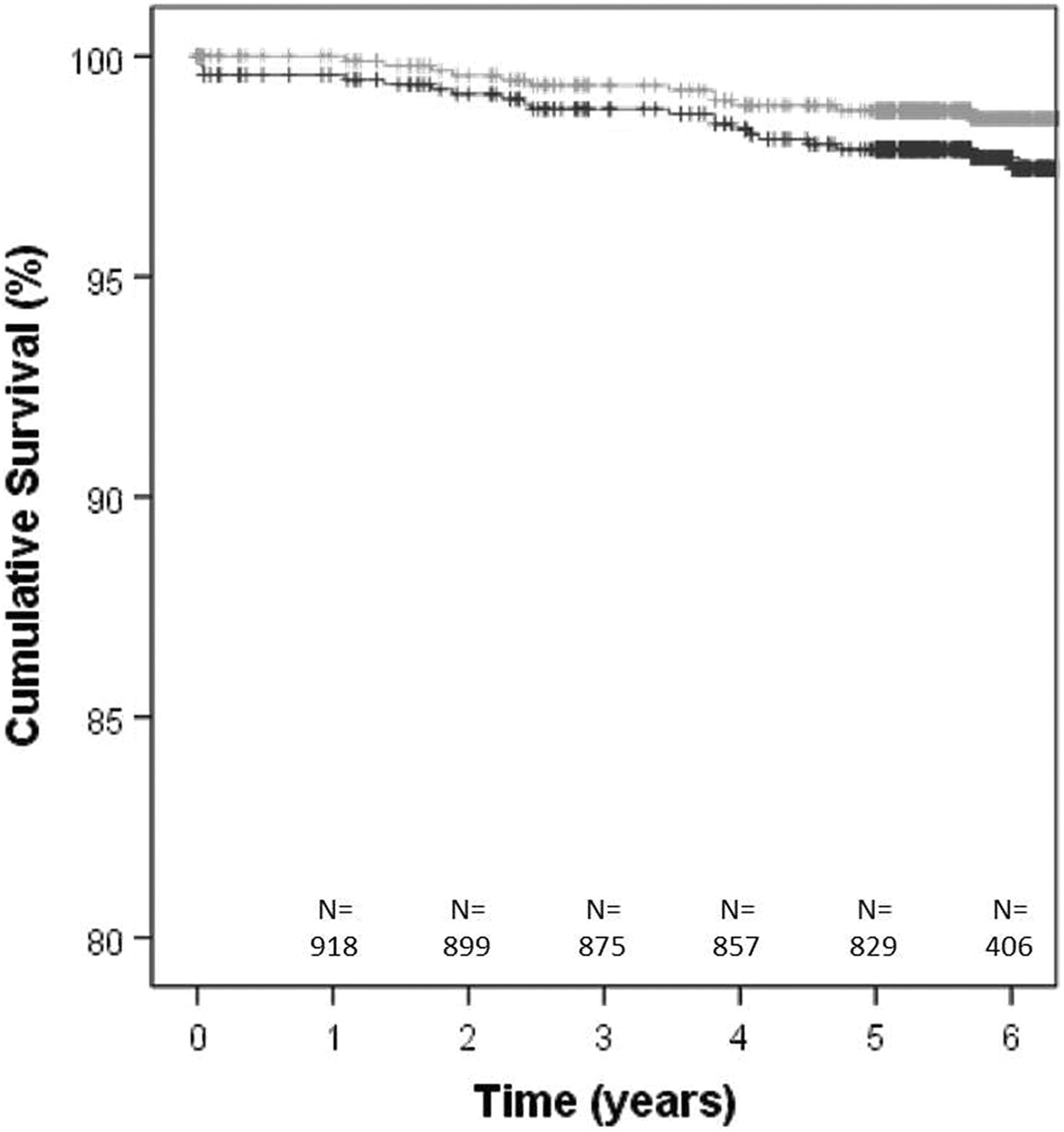
Kaplan–Meier survival curve for the Accolade TMZF. The grey curve indicates the survival with aseptic loosening as the reason for revision, while the black curve indicates the survival for all reasons for revision. At the bottom of the graph, the remaining number of THAs in the cohort of the black curve at the corresponding time point is presented. THA: total hip arthroplasty.
RRs with 95% CI resulting from the Cox regression analysis.

RR: revision ratio; CI: confidence interval.
With regard to the effect of a learning curve, a χ 2 test revealed no difference (p = 0.74) in the number of revisions between the group that consisted of the first 20 THAs of all surgeons (n = 205), the group with the 21st up to the 50th THA of each surgeon (n = 229) and the group consisting of procedures performed with the experience of 50 previously performed Accolade TMZF stems (n = 503). Respectively, 6 (2.9%), 5 (2.2%) and 10 (2.0%) revisions were observed.
Discussion
The current study demonstrated an implant survivorship of the Accolade TMZF stem of 97.9% after 5 years follow-up in a cohort of 937 primary THA. It was also demonstrated that no learning curve was observed after the introduction of this prosthesis. Furthermore, patient age, comorbidity and surgical approach had no effect on survival.
In our series, a mid-term Kaplan–Meier implant survivorship for the whole group of 97.9% with revision for all reason and 98.8% with aseptic loosening as endpoint is slightly lower but by all means comparable with the results of other groups using this stem. 1,6 –8 These studies reported 99.4 to even 100% survival with aseptic loosening as endpoint. However, most of these results are from high volume hospitals where the procedures were performed by a few high volume hip surgeons or even developers of this particular stem. Results from the current study align with findings in the British National Joint Registry (probability for revision 2.65% for the Accolade I/Trident combination) and from the Australian Orthopaedic Association (cumulative percent revision of 3.8% for the Accolade I/Trident combination) relating to use of this implant at 5 years follow-up. 26,27 Our series, coming from a non-designers’ high volume general teaching hospital, includes 12 different orthopaedic surgeons, of which only 5 are relatively high volume surgeons. Moreover, our series includes all hips from the first day we used this stem and also all THA performed by orthopaedic fellows and residents under supervision at our institute. Early subsidence of the Accolade TMZF stem has been described using Einzel-Bild-Röntgen-Analyse (EBRA) analysis and it was uncertain if this would lead to poorer results on behalf of early aseptic loosening due to poorer initial fixation. 18 Jacobs and Christensen reported a higher revision rate in males (4.2% revisions within the first 3 years) of the Accolade TMZF stem. 23 It was supposed that this early subsidence of the stem and higher revision rate possibly was a result of immediate full weight bearing direct after surgery. 18 In our series, immediate full weight bearing after surgery was permitted in all patients and that did not seem to have had that amount of a negative effect on survival of the stem.
In the current series, the predominant reason for failure was aseptic loosening. We found a risk of periprosthetic fracture of 0.6%, while recurrent dislocation was the reason for revision in 0.1%. One hip was revised for infection (0.1%) and one hip showed signs of trunnion wear with pseudotumour formation (0.1%). The infection rate was low in this series. Every patient in need of an orthopaedic implant is routinely screened at our department for Staphylococcus carriership and every carrier is consequently treated to eradicate Staphylococcus perioperatively. This generally decreases surgical site infections. 28 On the other hand, this infection rate does not reflect all infection cases, but only the one that required stem revision. We have a low threshold for treating any suspicion on deep infections in the early postoperative period by debridement, antibiotics and with implant retention. These cases do not show in the stem revision outcome. Revision of the Accolade stem was fairly easy, and in most cases, a standard primary stem (Exeter cemented stem or Accolade TMZF stem in cases of under sizing) could be used. In the cases with a periprosthetic fracture, a long modular hip stem was necessary.
We included all inserted stems in this series from day 1. We wondered whether we could find any sign of a learning curve that led to a negative effect on the mid-term survival of the Accolade TMZF stem. Data from the Nordic Arthroplasty Register Association database suggested that there is only an association between hospital volume and risk of revision for uncemented prosthesis for hospitals producing over 200 total hip arthroplasties annually. A reduced risk of revision at 5, 10 and 15 years was shown compared to hospitals having a lower amount of THA annually in only one of four large hospital volume groups, suggesting that generally there is not much of a learning curve in uncemented THA. 29 In our surgeon-based analysis of the learning curve, we did not find a statistically significant difference comparing the first 20 with the next 30 and all subsequent THAs of all surgeons. This also would suggest that the learning curve of the uncemented Accolade TMZF is small or even non-existent.
The total number of THA still increases annually in all developed countries. 5,30 There is a trend in a progressive use of uncemented femoral and acetabular components in time. 5 In the Netherlands, 62% of all primary THA were done uncemented between 2007 and 2014. 31 Worldwide, the use of the total amount of uncemented THA varies enormously. 5 If this vast and increasing use of uncemented THA can be justified has been doubted, especially in the older (>65 years) patient group. 5 However, in our current series, we have found no effect of age on the outcome. Therefore, we would conclude that the stem can safely be used in any age group.
We conclude that the Accolade TMZF stem fulfils the challenges to stem design as formulated by Lettich et al. 6 The current study shows a good mid-term survival of the Accolade TMZF in a non-developer, non-academic teaching hospital. The stem can be implanted with ease and without an apparent learning curve. Complication rate is low and if stem revision is needed, this can be performed quite easily. Hence, the Accolade TMZF hip stem can safely be used in all patients. Stryker Orthopedics also has launched the Accolade 2 stem based on three-dimensional design using a large database of high resolution computed tomography; a new stem design would in theory allow for a better proximal fit and fill than the Accolade TMZF stem. 32 Whether this influences the outcome remains to be debated.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first and last authors are paid consultants for the supplier of the prosthesis discussed in this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our research foundation receives financial support from several companies (including the supplier of the prosthesis discussed in this manuscript), although not related to the content of the current manuscript.