
Abstract
Purpose:
To explore factors influencing muscle strength after anterior cruciate ligament (ACL) reconstruction (ACLR) in pediatric patients. We hypothesized that obesity/overweight, autograft hamstring tendon, and concomitant injuries would be associated with slower muscle recovery.
Methods:
We retrospectively reviewed the records of pediatric ACLR patients during a 3-year period. Muscle recovery was defined as ≥85% of peak torque compared with the contralateral side. We categorized patients as either obese/overweight or normal weight. Statistical analysis was performed using Mann–Whitney U, analysis of variance, and χ 2 tests (α level < 0.05).
Results:
The study group consisted of 330 patients, of whom 198 (60%) and 231 (70%) met quadriceps and hamstring recovery criteria, respectively, at final testing (mean: 7.0 ± 3.2 months). Patients recovered hamstring and quadriceps strength at a mean of 5.3 ± 2.2 months and 6.1 ± 2.3 months, respectively. Hamstring muscle recovery took significantly longer in obese/overweight patients (mean: 5.7 ± 2.2 months) versus normal-weight patients (mean: 5.1 ± 2.1 months; p = 0.025), but quadriceps recovery did not (obese/overweight mean: 6.5 ± 2.6 months; normal-weight mean: 5.9 ± 2.1 months; p = 0.173).
Conclusion:
Concomitant injuries and graft type were not associated with length of time to recovery of muscle strength. Obesity/overweight was associated with delay in recovery of hamstring but not quadriceps strength.
Introduction
The number of anterior cruciate ligament (ACL) tears in children and adolescents has increased in recent years, partly because of the rise in the number of young athletes. The number of youth participating in organized sports rose from 32.8 million in 1997 to 44 million in 2008. 1 Female athletes, who have a higher incidence of ACL tears than their male counterparts, make up 34% of this group. More young athletes now play sports year-round, resulting in more injury-exposure hours.
Recovery from ACL injuries can be difficult. Biologically, ACL grafts incorporate quickly. Bone-tendon-bone grafts incorporate at approximately 6 weeks, whereas soft-tissue tendon grafts incorporate at approximately 12 weeks. 2 However, it takes approximately 1–3 years for a tendon graft to fully ligamentize. 3,4 A patient’s return to activity depends on the strength and function of the surgical leg, rather than ligament biology. Of the two markers of recovery, strength is the more objective measure. There are, however, many patient and injury variables in the recovery process, which influence the time it takes for muscles to recover strength.
Our goal was to investigate the associations of body mass index (BMI) category, concomitant injuries, and graft type with time to hamstring and quadriceps muscle recovery after ACL reconstruction (ACLR) in pediatric patients. We hypothesized that obesity/overweight, use of an autograft hamstring tendon, and concomitant injuries would be associated with slower quadriceps and hamstring muscle recovery.
Materials and methods
After receiving institutional review board approval, we retrospectively reviewed the records of all patients <18 years of age who underwent ACLR at our institution from January 2009 to October 2013. Patients without Biodex System 3 (Biodex Medical Systems, Shirley, NY, USA) muscle testing data were excluded. Records were reviewed for the following patient information: sex, age, height, weight, concomitant injuries, and graft type. Muscle recovery of the quadriceps and hamstring was evaluated. Muscle recovery was defined as ≥85% peak torque in isokinetic testing compared with the contralateral side, which is standard at our institution. 5 Exclusion criteria were (1) incomplete clinical records; (2) ACL graft tears in the setting of previous ACLR; (3) lack of muscle testing data; and (4) failure to reach muscle strength recovery in the quadriceps and hamstring by the last visit.
We calculated BMI using height and weight measured within 30 days of surgery. We assigned patients with BMI values in the 85th percentile or higher for age to the obese/overweight group, patients in the 5th to 84th percentile to the normal-weight group, and patients below the fifth percentile to the underweight group. Statistical analysis was performed with Mann–Whitney, analysis of variance (ANOVA), and χ 2 tests using SPSS, version 22.0, software (SPSS Inc., Chicago, IL, USA). α-Level was set at 0.05.
Our preferred graft choice for ACLR in pediatric patients was hamstring autograft. Supplemental allograft tendon was used when autograft hamstring did not yield sufficient length or graft diameter. Patients with underlying conditions associated with soft-tissue laxity and those with clinical signs of laxity were the exceptions. In these cases, allograft was the preferred choice. A secondary option for autograft is bone-tendon-bone, which was used at the surgeon’s discretion. Finally, iliotibial band reconstruction is an option for the youngest and smallest patients, which was also used at the surgeon’s discretion.
Our postoperative ACLR protocol allows for partial weightbearing with a brace locked in extension for the first week. Transition to full weightbearing is initiated at week 2 but delayed until week 4 in the setting of meniscal repair. The brace is unlocked for weightbearing at week 4. Finally, the brace is discontinued at week 6. Isokinetic testing is started at 3 months and routinely measured until muscle recovery is obtained.
Results
The study group consisted of 330 patients (188 girls) with a mean age of 14.6 years (range 8.3–17.9 years). In terms of BMI, 218 patients were normal weight, and 112 were obese/overweight. One patient was underweight and was excluded from the analysis.
For concomitant injuries, we analyzed meniscal tears, cartilage damage, and collateral ligament tears. Meniscal tears were present in 238 patients (72%), and cartilage damage was present in 156 patients (47%). Seventy-one patients (22%) had collateral ligament tears (59 medial, 5 lateral, and 7 both medial and lateral). Ten patients (3.0%) had concomitant posterior cruciate ligament (PCL) tears. Most patients (N = 285; 86%) received hamstring autograft, whereas 30 patients (9.1%) had allograft reconstruction and 12 patients (3.6%) had hybrid allograft and autograft reconstruction. The remainder consisted of two bone-patella-bone autografts and one iliotibial band autograft.
Of the 330 patients in the study group, 198 (60%) and 231 (70%) met quadriceps and hamstring recovery criteria, respectively, at their last testing. These patients recovered quadriceps strength at a mean of 6.1 ± 2.3 months and hamstring strength at a mean of 5.3 ± 2.2 months. There were no differences between patients who met our definition of hamstring recovery and those who did not in terms of age, sex, and proportion of obese/overweight patients. Those who did not meet our definition of quadriceps recovery were, on average, 0.6 years (95% confidence interval: 0.2–1.1 years) older than patients who recovered function. There was a higher proportion of female patients (64% vs 52%) in the group that did not recover quadriceps function (Table 1).
Differences in age, sex, and body mass index category by quadriceps and hamstring muscle recovery status in 330 pediatric patients after anterior cruciate ligament reconstruction.

a Expressed as mean ± standard deviation.
b Body mass index values at or above the 85th percentile for age and sex.
Hamstring muscle recovery took significantly longer in the obese/overweight group (mean: 5.7 ± 2.2 months) versus the normal-weight group (mean: 5.1 ± 2.1 months; p = 0.025). Quadriceps muscle recovery was not significantly slower in the obese/overweight group (mean: 6.5 ± 2.6 months) versus the normal-weight group (mean: 5.9 ± 2.1 months; p = 0.173).
For patients with meniscal tears, time to muscle recovery after ACLR was 6.1 ± 2.2 months for the quadriceps and 5.3 ± 2.2 months for the hamstring compared with 6.1 ± 2.5 and 5.3 ± 2.1 months, respectively, for patients without a meniscal tear. For patients with collateral ligament tears, time to recovery was 6.3 ± 1.9 months for the quadriceps and 4.9 ± 1.9 months for the hamstring compared with 6.0 ± 2.4 and 5.4 ± 2.2 months, respectively, for patients without collateral ligament tears. Time to muscle recovery in patients with cartilage damage was 5.9 ± 1.9 months for the quadriceps and 5.1 ± 2.2 months for hamstrings, compared with 6.3 ± 2.5 for the quadriceps and 5.5 ± 2.1 for hamstrings in patients without cartilage damage. Patients with concomitant PCL injuries were not compared with patients with isolated ACL injuries because of the small number of patients with PCL injuries (N = 10).
For patients with a hamstring autograft, time to muscle recovery was 6.0 ± 2.3 months for the quadriceps and 5.3 ± 2.2 months for the hamstring. Patients with hamstring allograft recovered at 6.9 ± 1.8 (quadriceps) and 5.6 ± 2.5 (hamstrings) months, whereas patients with a hybrid hamstring allograft and autograft recovered at 6.5 ± 3.1 (quadriceps) and 5.8 ± 1.6 (hamstrings) months. The two patients with bone-patella-bone autograft and the one patient with iliotibial band autograft were not included in the analysis of graft types because of the limited sample size. A one-factor ANOVA showed no statistical difference between these three graft types (p = 0.332 (quadriceps); p = 0.643 (hamstrings)). Mann–Whitney tests showed that differences between meniscal tear status, collateral ligament tear status, and cartilage damage were not statistically significant in relation to recovery rate (p > 0.05) (Table 2). A subgroup analysis in terms of age, sex, and proportion of obese/overweight patients is shown in Table 3.
Recoverya time for quadriceps and hamstring muscles after anterior cruciate ligament reconstruction in pediatric patients by body mass index category, concomitant injuries, and graft type.
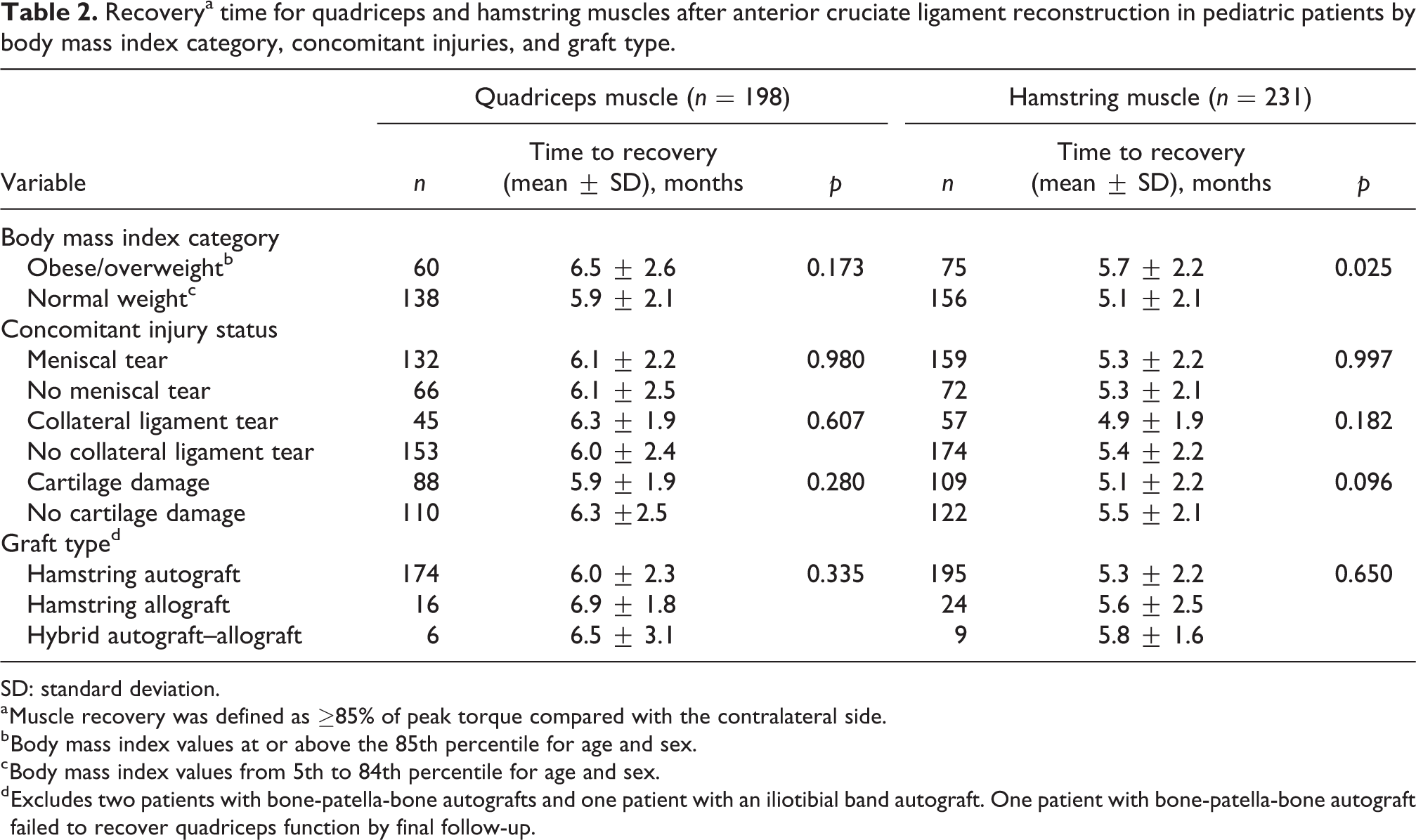
SD: standard deviation.
a Muscle recovery was defined as ≥85% of peak torque compared with the contralateral side.
b Body mass index values at or above the 85th percentile for age and sex.
c Body mass index values from 5th to 84th percentile for age and sex.
d Excludes two patients with bone-patella-bone autografts and one patient with an iliotibial band autograft. One patient with bone-patella-bone autograft failed to recover quadriceps function by final follow-up.
Differences in age, sex, and body mass index category between subgroups of pediatric patients who achieved quadriceps and hamstring muscle recovery after anterior cruciate ligament reconstruction.a

NA: not applicable; SD: standard deviation.
a Muscle recovery was defined as ≥85% of peak torque compared with the contralateral side.
b Body mass index values at or above the 85th percentile for age and sex.
c Body mass index values from 5th to 84th percentile for age and sex.
d Excludes two patients with bone-patella-bone autografts and one patient with an iliotibial band autograft. One patient with bone-patella-bone autograft failed to recover quadriceps function by final follow-up.
Discussion
Recovery of quadriceps and hamstring muscle strength is possible by 6 months after ACLR in children. Obesity/overweight was associated with a significantly longer hamstring recovery time (5.7 vs. 5.1 months for patients who were not obese/overweight). Concomitant injuries and the use of the ipsilateral hamstrings for an ACL autograft did not significantly delay muscle recovery.
This study shows that the goal of muscle recovery by 6 months is reasonable after ACLR in children. These results correlate with those of a previous study of the quadriceps muscle in a group of 55 adolescents, which also showed that quadriceps muscle strength recovery is possible at 6 months. 5 Recovery of quadriceps muscle strength was uniformly slower than hamstring recovery, illustrating the importance of addressing quadriceps strength and activation early in the recovery process.
Although obese or overweight children have shown a higher likelihood to experience more severe traumatic injuries, they have also shown similar recovery times to the normal-weight population. 6,7 For fracture recovery, healing times were the same for obese versus nonobese patients, and return to activity after healing was also similar. 8 We show here that in the setting of ACL tears in children, overweight or obese patients are able to achieve muscle recovery within a similar time period to their normal-weight counterparts. Quadriceps muscle recovery was not delayed in the 34% of the population who were obese/overweight. Although hamstring muscle recovery was delayed in obese/overweight patients compared with normal-weight patients (5.7 vs. 5.1 months, respectively; p =0.025), in the context of a 9- to 12-month rehabilitation period, 18 days is unlikely to alter the ability to return to sports during a particular season. There was no difference between the percentage of obese/overweight patients who achieved muscle recovery (for both hamstrings and quadriceps) compared with the percentage of obese/overweight patients who did not, further emphasizing that obese/overweight patients are capable of achieving muscle recovery within similar timeframes as their normal-weight counterparts.
Our results show that children with ACL tears and concomitant meniscal, chondral, or additional ligamentous injuries still have the ability to meet early muscle-recovery goals. Meniscal injuries may influence early postoperative rehabilitation because patients with meniscal repairs are limited to 90° of knee flexion. However, it seems that an early delay in postoperative rehabilitation does not affect postoperative muscle recovery at 6 months. Collateral ligament or PCL injury can delay initial reconstruction as time is allowed for potential healing and nonoperative treatment. Although this time may result in an overall delay in the patient’s return to activity and sports, this was not accounted for in this evaluation of muscle recovery. Chondral injuries have an important influence on knee function in subsequent decades of life, with higher and earlier risk of developing arthritis. However, the influence on muscle recovery is likely minimal because mild chondral injuries do not typically restrict a patient’s progression through the postoperative recovery protocol.
Most of our patients underwent hamstring autograft reconstruction. There were no statistical differences in time to muscle recovery for either hamstrings or quadriceps by graft type, including hamstring autograft, hamstring allograft, and a hybrid of hamstring autograft and allograft. However, the sample sizes in the allograft and hybrid groups were much smaller than the autograft group. Other studies have reported ongoing hamstring weakness with the use of hamstring autograft. Lee et al. 9 noted hamstring strength was only 80% at 6 months and 1 year compared with that of the contralateral leg in a series of 20 adults, and a review by Petersen et al. 10 found ongoing weakness after 5 years. Our population consisted of “high-performing” patients who met recovery goals, and we excluded “low-performing” patients who did not reach recovery goals at the time of final testing, making our study populations inherently different. Furthermore, our patients were not routinely tested after meeting the strength goal of ≥85% of the contralateral leg; thus, we are unable to determine whether our patients had an ongoing strength deficit.
Our study consists of pediatric patients who were treated at a children’s hospital. Strengths are the large cohort of pediatric patients and the uniformity of the rehabilitation process because all patients were provided with the same step-by-step rehabilitation protocol. Limitations include the sample bias inherent in including only those patients who completed follow-up and met physical therapy goals. This study population represents patients who were the most compliant with our postoperative protocols, who attended postoperative visits until release, and who completed Biodex System strength assessments with physical therapy. The patients not represented in the group are those who did not recover ≥85% of strength, those were lost to follow-up, and those who did not complete Biodex System assessments. Many of these patients would have likely had delayed muscle recovery. Our study does not suggest that all children will recover muscle strength in 6 months. Instead, it indicates that muscle recovery is possible in 6 months. Our study is underpowered to detect a difference between those who underwent hamstring autograft and those who did not. This is a reflection of our preference for using hamstring autograft in pediatric patients. Also, our study does not address the functional portion of ACL rehabilitation, including dynamic balance and sport-specific movements, which is an important part in a patient’s return to activity. Six months until muscle recovery does not equate to 6 months until return to sports. However, the time to functional recovery likely correlates with the recovery of muscle strength because progression to functional rehabilitation is usually preceded by regaining adequate strength.
Conclusion
As the number of young athletes with ACL injuries increases, patients undergoing ACLR and hoping to return to sports will benefit from more accurate predictions of their recovery time and more appropriate rehabilitation goals. Standardized, objective measures of strength and function would further enable us to guide patients. Although higher BMI values were associated with slower hamstring recovery, BMI was not associated with slower quadriceps recovery. Similarly, meniscal tears, collateral ligament injuries, and graft type were not associated with delayed recovery of muscle strength in the pediatric patients who recovered strength earliest after ACLR.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.