
Abstract
Introduction:
The prevalence of radial nerve injury during surgery is as high as the prevalence of radial nerve injury due to trauma. The aim of this study is to minimize the risk of iatrogenic injury of radial nerve.
Materials and Methods:
Fifty patients with middle or distal diaphysis fractures of humerus and 18 patients with pseudoarthrosis at the same localizations were treated with surgery. Plate-screw fixation was performed with anterior approach in 43 patients. Eleven patients had minimally invasive plate osteosynthesis, and 14 patients had intramedullary nailing. The localization of the radial nerve was determined with nerve stimulator at the area of dissection.
Results:
Iatrogenic radial nerve injury did not occur in patients treated with open reduction or minimally invasive approach.
Discussion:
Nerve stimulator may be a method that decreases radial nerve injury, an iatrogenic complication. This method may be used in anterior approach and minimally invasive procedures.
Keywords
Introduction
Simultaneous injury of humerus and radial nerve is frequently seen due to their close neighborhood. 1 –3 Surgical trauma and trauma-causing fractures may cause radial nerve dysfunction. 2,4 –9 Surgical techniques have different probabilities for iatrogenic radial nerve injury. Iatrogenic radial nerve injury is seen in 6% of the cases that had intramedullary fixation; however, it was reported up to 21% in the ones who had open reduction and plate fixation. 9 Radial nerve injury due to trauma (primary injury) is seen approximately in 12% of the patients. 2,10 Radial nerve injury does not always heal spontaneously. It was reported that nerve functions did not improve spontaneously in 12% of the patients with primary radial paralysis and in 7% of the patients with iatrogenic radial nerve paralysis, and those patients had surgical treatment of peripheral nerve injuries. 2
In this study, we used nerve stimulator while performing surgery on humerus. We determined the localization of the radial nerve with nerve stimulator. In this way, we avoided excessive dissection of the radial nerve.
In this study, we aimed to determine iatrogenic radial nerve injury rates in anterior approach with use of nerve stimulator, minimally invasive plate osteosynthesis (MIPO), and intramedullary nailing (IMN). We hypothesized that use of nerve stimulator decreased the rate of iatrogenic radial nerve injury.
Patients and methods
We treated 102 patients with diaphysis fracture, pseudoarthrosis, or pathological fractures of humerus between January 2011 and 2015. Open reduction and internal fixation with anterior approach was performed in patients with 1/3 middle and distal (middle and middle distal diaphysis) humerus diaphysis fractures, and locking plate-screws were used for fixation. In the fractures that were fixated with MIPO technique, anterolateral or deltoid split incisions were used proximally, and anterior or lateral incisions were used distally, and locking plate-screws were used for fixation. Distal fixation was done using distal part of the anterior approach while making IMN. The presence of the nerve in distal lateral or anterior dissection planes was controlled with nerve stimulator in MIPO and IMN approaches. Humerus pseudoarthrosis was fixated with bone graft + plate-screw or intramedullary nail.
The protocol of this retrospective study was approved by the Ethics Committee. Data were obtained from the records of emergency, operating room, and epicrisis records of the patients. The demographic data, diagnosis, classification of the fracture, and presence of neurological deficit before and after surgical procedure were determined from those records. Nine patients who had radial nerve deficit before surgery and the ones who were treated with lateral and posterior approaches were excluded.
Surgical technique
The patients had surgery under general anesthesia. Neuromuscular blocking agents were not used to see the muscle contraction after stimulation of the nerve. The patients had surgery, while they were in supine position. The forearm was supported to keep the elbow at 45° flexion. The ground electrode of the stimulator was adhered to the skin of the patient in the non-sterile area.
A longitudinal incision was made through the lateral border of the biceps muscle. Skin, subcutaneous tissues, and fascia were incised. Biceps muscle was found, and then lateral cutaneous antebrachial nerve was identified on its inferior surface. The groove between brachialis and brachioradialis muscles was found, but it was not dissected. The needle of the nerve stimulator was inserted into this groove (Figures 1 and 2). The voltage of the device was adjusted to 1 mA. The position of the needle was changed until wrist extension was seen with stimulation of the nerve. The voltage of the stimulator was incrementally decreased after extension of the wrist was observed. Extension of the wrist with a stimulation voltage of 0.3 mA indicated close proximity of the needle to the nerve. The localization of the radial nerve was determined. The intermuscular groove was not dissected, and the radial nerve was not suspended. Retractor pressure was not applied to the radial nerve since its localization was determined. Then, the midpoint of the brachialis muscle was found. Absence of the nerve was shown using nerve stimulator. The muscle was dissected parallel to the muscle fibers, and the bone was exposed. There were extensive adhesions and granulation tissue in the patients who had surgery with the same incision before. In this case, nerve stimulator facilitated finding the radial nerve in the groove between brachialis and brachioradialis muscles. Anterior approach performed after identification of the radial nerve provided an exposure until the proximal border of the coronoid fossa distally. Since we identified the localization of the radial nerve and the groove was not dissected, entrapment risk of the nerve between the plate and the bone was eliminated. Muscle relaxants were used by the anesthesia team after the procedures related to the nerve were completed.

(a) The incision is made parallel to the lateral border of the biceps muscle. (b) Lateral cutaneous antebrachial nerve is found inferior to the biceps muscle.
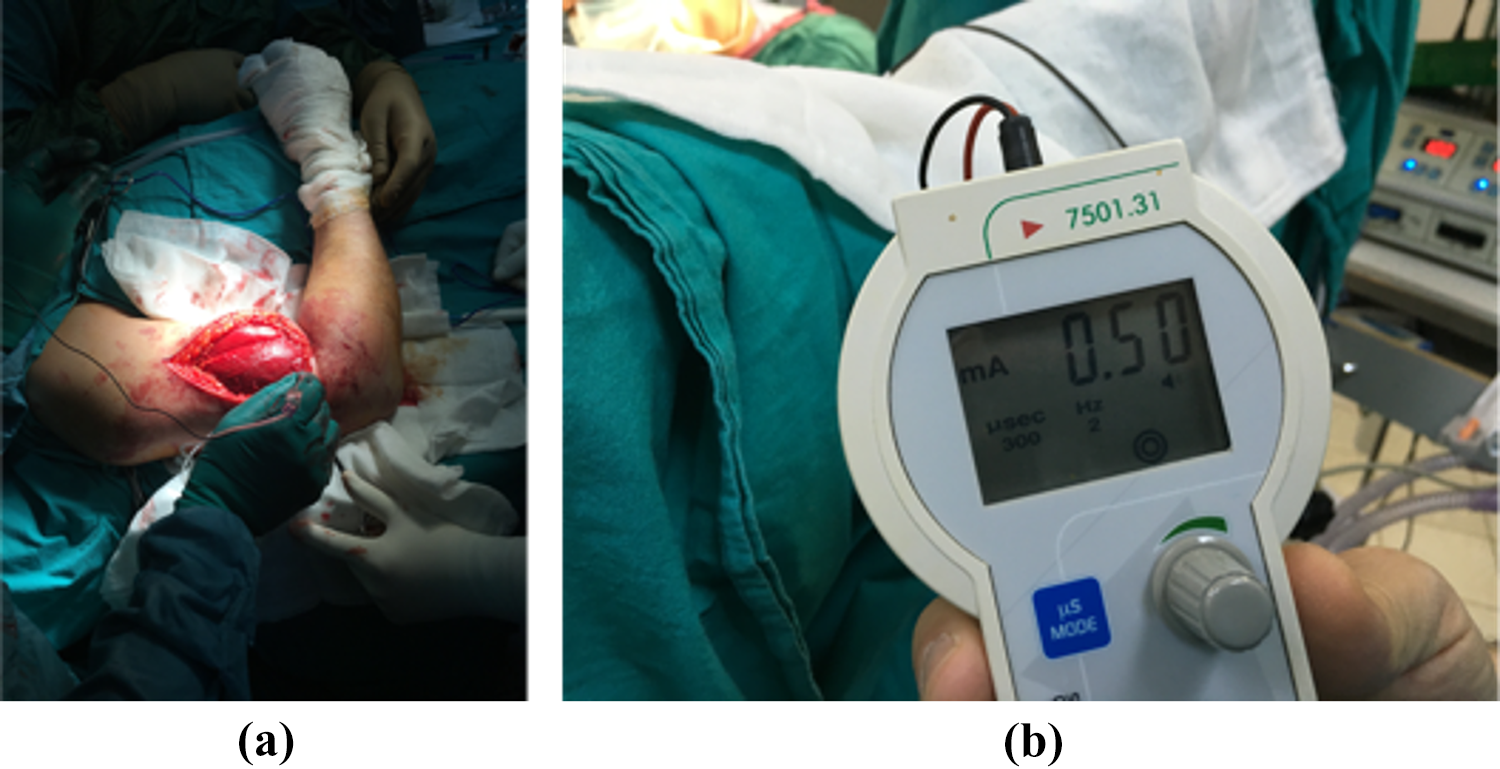
The nerve is stimulated by the nerve stimulator to find the localization of the nerve. The stimulation starts with 1 mA. If the wrist dorsiflexes with a stimulation of 0.3 mA, it is considered that the radial nerve localization is identified.
A tourniquet was not used during surgery. All surgical procedures were performed by the same surgeon (MG). All patients had prophylaxis for venous thromboembolism. Shoulder and elbow range of motion exercises was started short after surgery.
The functions of radial extensor carpal and brachioradialis muscles were checked at the level of wrist just after surgery, when cooperation could be achieved with the patient. 11
Means and ranges of the variables were calculated for statistical analysis (Excel; Microsoft, Redmond, Washington, USA).
Results
Nerve stimulator-assisted humerus surgery was performed in 68 patients in a 4-year period (Table 1). Surgery was performed for fixation of fracture in 50 patients and for treatment of pseudoarthrosis in 18 patients. Three patients with fractures had pathological fractures. Among the study population, 74% were males and 26% were females. Fractures or pseudoarthrosis were localized in distal or middle 1/3 of the diaphysis. AO/OTA classification revealed that 27 patients were 12A, 15 were 12B, and 8 patients were 12 C. There is one fracture line in type A fracture. In type B, there are butterfly fragments in different forms. Type C is used to identify segmental or comminuted fractures. 12
Demographic and surgical data.

ORIF: open reduction internal fixation; MIPO: minimally invasive plate osteosynthesis, IMN: intramedullary nailing.
Three patients with pseudoarthrosis had surgery twice, and two patients had surgery three times before. Pathological fractures of shaft of humerus were fixated with IMN. In MIPO and IMN groups, 18 of 25 distal lockings were done from anterior, and 7 of them were done from lateral aspect. The mean blood loss was 186 mL (range: < 60–350 mL) in the fracture patients treated with anterior approach. There were no intraoperative nerve- or implant-related complications.
No patients were lost to follow-up. There was no iatrogenic radial nerve injury.
Discussion
The aim of this study was to reduce the probability for iatrogenic radial nerve injury seen in humerus fracture surgery. For this purpose, we used nerve stimulator to find the radial nerve during the surgical procedure. We did not encounter iatrogenic radial nerve injury.
The rate of radial nerve injury was reported as 2–17% in humerus fractures. 13 –15 Radial nerve injury is seen most frequently in the fractures in 1/3 middle and distal shaft of humerus, since the radial nerve courses in the radial sulcus adhered to humerus. 16,17 The radial nerve may also be compressed in the intermuscular septum. 18 Neurapraxia may be seen in 88.1% of the cases in case of low-energy traumas, and it improves spontaneously in 4–6 months. 3,18 The rate of spontaneous recovery is lower in case of high-energy traumas. 19 Surgical treatment of radial nerve is performed in late term in absence of spontaneous recovery. The success rate of those procedures is 69%. 3
Radial nerve dissection may be necessary in all surgical approaches to humerus due to close neighborhood of humerus and radial nerve. 20 –24 Therefore, transient of permanent radial nerve injury may be seen. 25,26 We choose anterior approach in humerus shaft and distal diaphysis fractures, since it was possible to perform fixation without exposing the radial nerve. In this study, we did not encounter any iatrogenic radial nerve injury with anterior approach and minimally invasive procedures.
The most frequently performed approaches in mid- and distal diaphysis fractures of humerus are anterior, posterior, and lateral approaches. 27 –29 Iatrogenic radial nerve injury may be seen in 1 of 5 patients in lateral approach, in 1 of 9 patients in posterior approach, and in 1 of 25 patients in anterolateral approach. 30 Although iatrogenic injury of radial nerve usually improves within 1 year, some patients do not improve, and they need neurolysis or nerve grafting. 2,31 Healing period needs rehabilitation due to wrist drop deformity, and a dynamic splint is used whenever needed. Time to go back to work gets longer in those patients.
Iatrogenic radial nerve injury may be due to traction, pressure of the retractor, exposure, pressure of the implant, or drilling. 32 –34 The articles that focused on the procedures that could be undertaken in order to reduce the prevalence of those complications are scarce. 35 –38 We used nerve stimulator to protect the nerve and prevent injury to the nerve during soft tissue dissection. We did not perform radial nerve exploration and identification since we identified the localization of the radial nerve. In this way, we protected the nerve in its anatomical localization. We did not injure the vessels neighboring the radial nerve. We did not apply excessive retractor pressure to this region.
Nerve stimulators are used to identify the localization of the nerve in percutaneous peripheral nerve blocks. Those devices are widely used in the daily practice of the anesthesiologists. 39 We used the nerve stimulator during soft tissue dissection, not percutaneously. It has been supposed that the tip of the needle is very close to the nerve if the electrical stimulation of radial nerve causes stimulation of the nerve at a voltage of 0.3 mA. 40,41
MIPO method is criticized since the radial nerve is not exposed. Exploration and identification of the radial nerve is not necessary in anterior MIPO approach; however, the nerve may be exposed to retractor pressure if its localization is not known. Iatrogenic radial nerve injury may be seen in open reductions after the radial nerve is explored and suspended, and its spontaneous recovery may take up to 1 year. The localization of the radial nerve may be identified with nerve stimulator. In this way, the risk of dissecting the tissues without seeing the nerve in minimal invasive procedures is eliminated. In anterior approach, finding the localization of the nerve with nerve stimulator prevents excessive dissection in the course of the nerve. Therefore, local blood supply of the nerve is protected, and the risk of injury to the nerve is minimized.
Minimally invasive procedures with plate or intramedullary nails are used in fractures and pseudoarthroses of humerus due to need for minimal dissection, a smaller surgical scar, and early rehabilitation. 42,43 Use of intramedullary nails results in less frequent nerve injury compared to use of plates. 9 The radial nerve needs to be exposed if the distal locking screws of the minimally invasive surgery are to be placed through the groove between the brachialis and brachioradialis muscles. 44 The danger zones must be kept in mind while placing screws, particularly in minimally invasive surgery, since percutaneous screwing is not safe. 13,32 Use of nerve stimulator eliminated the need for dissection of the nerve. In MIPO and IMN approaches, the localization of the nerve is determined with nerve stimulator before dissection performed for distal locking, and the dissection may be continued without dissecting the nerve. We did not encounter any nerve impairments in the nerve function after IMN, minimally invasive surgery, and distal locking approach.
Open reduction internal fixation or MIPO methods may be used in together with anterior approach in humerus surgery. 22,41 However, anterior and anterolateral approaches have not been differentiated clearly in the literature. 24,45 An incision is made parallel to the lateral border of the biceps muscle in order to place a plate to the shaft of humerus anteriorly. The intermuscular dissection may be performed through three routes after this incision. Approaching humerus lateral to brachialis muscle may be called as anterolateral approach, approaching humerus from the midpoint of brachialis muscle may be called as anterior approach, and approaching humerus medial to brachialis muscle may be called as anteromedial approach. 8
In this study, two groups were not statistically compared. Two different groups for comparison could not be identified since there was no deficit in the radial nerve function with use of the nerve stimulator. Further prospective randomized studies on larger patient series are needed.
Conclusion
Use of nerve monitor during dissection enables a safer surgery. Nerve stimulator prevents insufficient dissection of the radial nerve in minimally invasive surgery and its excessive dissection in classical anterior approach.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.