
Abstract
Purpose:
The aim of this study was to evaluate short-term clinical and radiological results of extensor carpi radialis longus (ECRL) tendon ball arthroplasty for treatment of late-stage Kienböck’s disease.
Methods:
We retrospectively reviewed data of 19 patients suffering from Kienböck’s treated with ECRL tendon ball arthroplasty between December 2014 and December 2016. Patients’ clinical functions were assessed using grip strength, range of motion (ROM) of the wrist, QuickDASH, Mayo wrist score, and visual analog scale score. Radiological examination was performed to assess carpal height ratio and progression of arthritis.
Results:
The median follow-up was 30 months (range, 12–36 months). At final follow-up, ROM of operated wrist was 71% of the nonoperated side. Thirteen (86.6%) patients were pain free. Carpal height ratio was statistically significantly reduced compared with preoperative values. All patients declared their satisfaction with the results due to their preoperative status.
Conclusions:
ECRL tendon ball arthroplasty is a new and good option for treatment of late-stage Kienböck’s disease with low complication rate.
Introduction
Although Kienböck’s disease has been described for over 100 years, the exact etiology is still unknown and optimal treatment is contoversial. 1 Traumatic, anatomic, morphological, mechanical, vascular, and systemic factors have been attributed as potential risk factors that can cause Kienböck’s disease. 1 –3
Lichtman classification is the most commonly used staging system. 4 Numerous treatment modalities have been suggested based on the stage of disease. 1 –4 In stage I, wrist immobilization with cast, splint, pins, or external fixator is a suggested treatment. 4–5 In stage II, pedicled or free vascularized bone grafts, radial metaphyseal core decompression, ulnar lengthening, capitate or radial shortening can be employed. 2,6 –12 In stage III, radial shortening, open or arthroscopic intercarpal arthrodesis, interposition arthroplasty, and proximal row carpectomy (PRC) have been advocated as surgical procedures. 1,2,13 –19 In stage IV, PRC and wrist arthrodesis are the most common treatment options. 2,19
Tendon ball interposition arthroplasty for treatment of late-stage (stages III and IV) Kienböck’s disease has been reported in literature with good results. 16,17,20 –25 In all of these articles, palmaris longus or pronator quadratus tendon was used. 20 –25 In 2013, Karalezli et al. reported a biomechanical cadaveric study using extensor carpi radialis longus (ECRL) tendon for interposition arthroplasty for treatment of Kienböck’s disease. 26 The purpose of our retrospective study was to assess radiological and clinical results following ECRL tendon ball interposition arthroplasty in late-stage Kienböck’s disease.
Materials and methods
Between December 2014 and December 2016, 19 patients with stage 3B Kienböck’s disease were treated by lunate excision and tendon ball interposition arthroplasty using the ECRL tendon. After ethical committee approval had been obtained, we retrospectively reviewed patients’ data. All patients gave written informed consent before surgery.
Patients treated with ECRL tendon ball arthroplasty, using the technique described by Karalezli et al., 26 for stage 3B with at least 1-year follow-up were included in the study. Four patients were excluded due to lost to follow-up. There were eight males and seven females with a mean age of 37.13 (range, 25–50) at the time of surgery. Eight right side and seven left side were operated. Twelve of 15 (75%) were dominant side. Negative ulnar variance, positive ulnar variance, and history of trauma on the affected wrist were present in five, one, and three patients, respectively. Major symptom was pain especially during working or doing housework. Mean duration of complaint was 20.3 months (range, 9–60 months). Two patients underwent surgery in early stage of disease; one was treated with metaphyseal core decompression 3 years ago and the other was treated with vascularized bone graft 2 years ago. In both patients, the disease progressed further. The demographics of patients were presented in Table 1. Patients’ grip strength and range of motion (ROM) of the wrist were compared with the nonoperated side. QuickDASH, Mayo wrist score, and visual analog scale (VAS) score were assessed at final follow-up. Radiological examination on preoperative and final follow-up radiographs was performed to assess carpal height ratio (method of Youm et al. was used 27 ) and progression of arthritis.
Demographics of patients.

Surgical technique
All patients were operated by the senior author. All operations were performed under general or axillary block anesthesia with patients in supine position and hand on a hand table. A non-sterile tourniquet was placed to proximal of arm and inflated 100 mm Hg over the patients’ systolic blood pressure. A transverse incision was made over the dorsum of the wrist (Figure 1). Second, third, and fourth extensor compartments were opened. Extensor carpi radialis brevis, ECRL, and extensor pollicis longus were retracted radially, and extensor tendons in fourth compartment were retracted ulnarly. Neurectomy was performed to the sensory branch of the posterior interosseous nerve. The capsule of the wrist joint was opened in U shape ulnarly. The collapsed lunate was separated by incising scapholunate and lunotriquetral ligaments and excised with care, while preserving the volar capsule (Figure 2). After excision of the lunate, two holes were drilled in the triquetrum and scaphoid using 2.7 cannulated drills (Figure 3). Then, the ECRL tendon was identified and separated from its musculotendinous origin by another incision, insertion of tendon left intact (Figure 4). The ECRL tendon divided into two strips in wide of 1/3 and 2/3 of tendon (Figure 5). The larger tendon strip was rolled around to form a tendon ball and fixed with two 21G needles (Figure 6). The tendon ball was sutured with a 2.0 Ethibond suture in U shape (Figure 7). The thinner tendon strip was passed through holes drilled in the scaphoid and triquetrum. The 2.0 Ethibond suture had passed through the palmar side of the thinner tendon strip to secure the tendon ball after insertion (Figure 8). Then, the tendon ball was inserted into the space of excised lunate. The thinner tendon strip sutured itself and over the tendon ball to prevent future dislocation of the tendon ball and mimic intercarpal ligament for stability (Figure 9). The stability of the tendon ball and ROM of wrist were evaluated. Tourniquet released. After sufficient hemostasis, the capsule was repaired. Extensor retinaculum was reconstructed. A Penrose drain was placed and the skin was closed with interrupted sutures. Wrist immobilized with a short-arm splint in wrist 15–20° palmar flexion.

Dorsal transverse incision.

Excision of the lunate, care should be taken not to harm the volar capsule.

Holes drilled in the scaphoid and triquetrum with a 2.7-mm drill.

Harvesting ECRL from its origin. ECRL: extensor carpi radialis longus.

Divide ECRL tendon into two tendon strips (2/3 and 1/3). ECRL: extensor carpi radialis longus.

Roll the larger strip to form a tendon ball and secure with 21G needles.

Suture in U shape the tendon ball with 2.0 Ethibond.

Passing the thinner tendon strip through the scaphoid and triquetrum, and put on a suture further securing the tendon ball.

Tendon ball placed into cavity and tendon strip sutured over.
The day after surgery, the Penrose drain was removed and the patient was discharged from hospital. The short-arm splint was removed 3 weeks after surgery and physiotherapy was begun for active and passive wrist exercises. Strengthening exercises started at 6 weeks.
Statistical analysis
Statistical analysis was carried out using the SPSS version 22.0 (SPSS Inc., Chicago, Illinois, USA) software. Paired sample t test and Wilcoxon signed-rank test were used to compare the measurement results. A p value of <0.05 was considered statistically significant.
Results
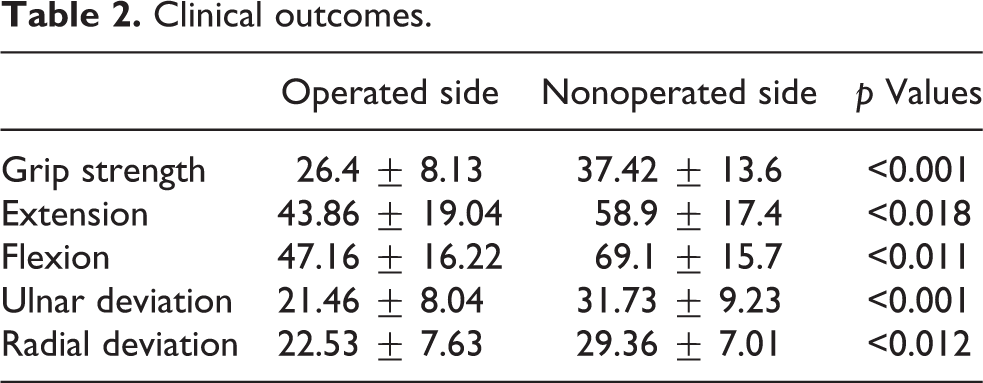
The median follow-up was 30 months (range, 12–36 months). At final follow-up, 13 (86.6%) patients were pain free, while one patient had occasional pain and one patient complained of pain during heavy construction works. Median VAS score was 0.85 (range, 0–5). Grip strength and ROM of the operated wrist were statistically significantly reduced compared with the nonoperated side (p < 0.05; Table 2). Carpal height ratio was statistically significantly reduced compared with preoperative values; 0.49 (range, 0.43–0.58; SD ±0.0487) to 0.43 (range, 0.34–0.52; SD ±0.0489) (p < 0.001). Mean Mayo wrist and QuickDASH scores were 78 (range, 60–100) and 9.83 (range, 0–30), respectively. No further radiological progression of carpal arthritis was observed in final radiographs.
Clinical outcomes.
Complications occurred in two patients. One of the patients had persistent pain after surgery due to insufficient neurectomy which resolved after second intervention to complete neurectomy. The patient was pain free in 28-month follow-up. The other patient had reflex sympathetic dystrophy, which resolved with medical treatment and physiotherapy. At final follow-up, all patients reported they are satisfied with the results and none of the patients changed their preoperative occupation.
Discussion
Treatment of Kienböck’s disease is still controversial. Many surgical interventions with good clinical results were described in the literature. 1 –3,6 –12 In this study, we presented a new surgical technique using the ECRL tendon in late-stage Kienböck’s disease with short-term results. To the best of our knowledge, this is the first clinical study using the ECRL tendon ball for treatment of Kienböck’s disease.
In late-stage Kienböck’s disease, the excision of lunate and replacement with silicone or tendon ball was described previously in the literature as a treatment option. 16 –25 Silicone replacement caused foreign body reaction with severe reactive synovitis and carpal instability which led to unsatisfactory results. 20,28,29
In some series using tendon ball arthroplasty for treatment of Kienböck’s disease, the authors reported that they used an additional tendon and free vascularized bone graft to substitute the cavity of the excised lunate. 16,17,21 –23 Some authors used K-wires or external fixator to stabilize wrist or carpal joints. 17,22 –24 In our study, ECRL tendon ball volume was enough to fill the cavity of lunate. Additional fixation was not needed due to enough stability provided by the tendon strip used to mimic intercarpal ligaments, as previously demonstrated by Karalezli et al. 26 Carpal height ratio was decreased postoperatively compared with preoperative values in our study. Sakai et al. reported a decrease in carpal height ratio had no effect on clinical outcomes. 21
King et al. reported that wrist strength and motion was not affected after loss of ECRL tendon. 30 Also, ROM at final follow-up was not different from previously reported series 17,21 –24 in our study.
Tendon ball subluxation was reported by some authors 16,24 ; in our series, we had no subluxation of the tendon ball. We believe the tendon strip around the tendon ball and suturing tendon ball to strip prevented subluxation. In this technique, care should be taken to prevent breakage of the scaphoid or triquetrum during drilling to make holes for the tendon strip. Drilling the carpal bones can also cause avascular necrosis which we did not have in our series. We did not notice progression of wrist arthritis in any of our cases, this can be related to our short-term follow-up period (Figure 10).
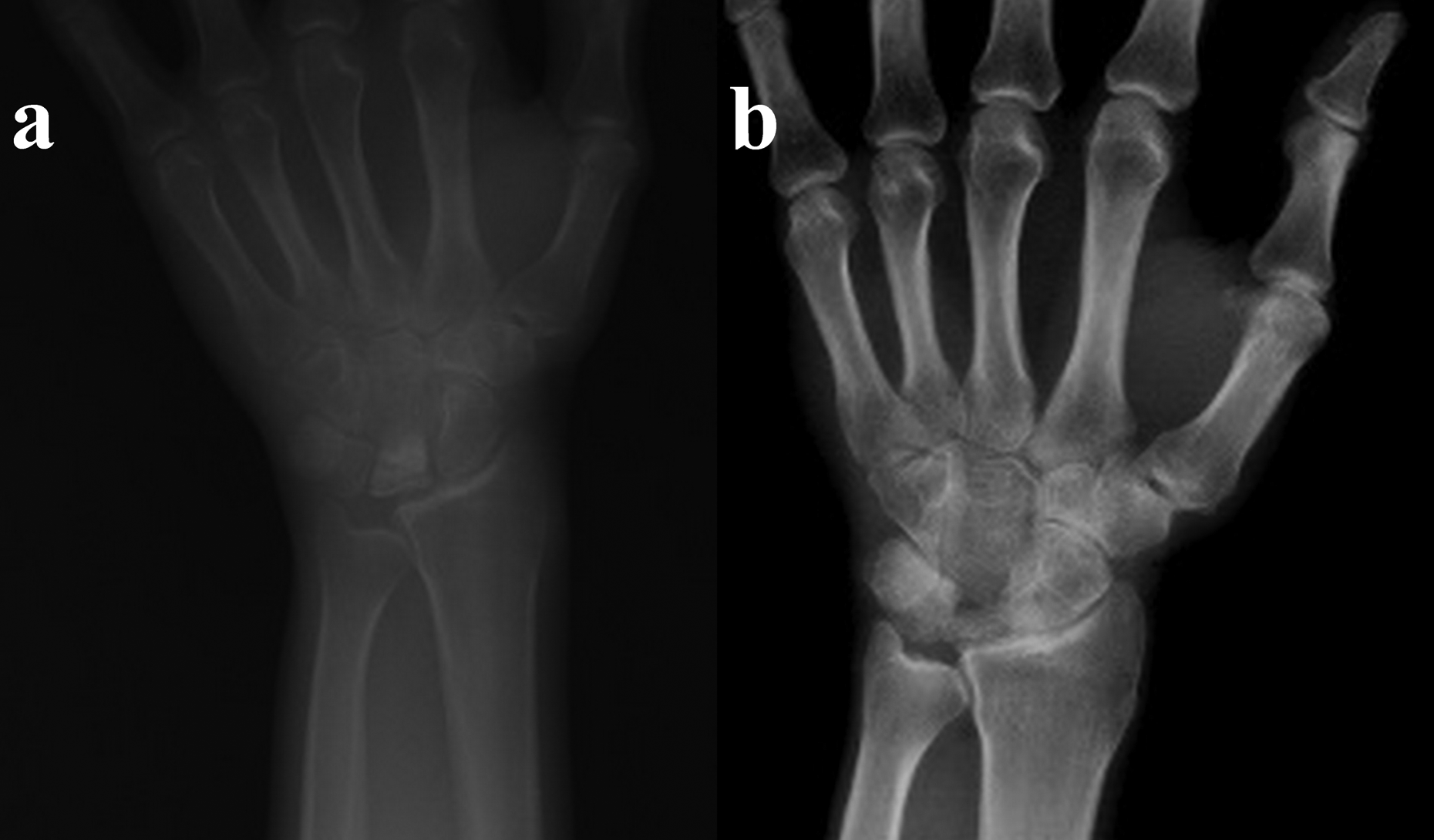
(a) Preoperative radiograph. (b) Thirty-six-month postoperative radiograph shows reduction of carpal height ratio, but no arthritic changes.
We had some limitations in this study. First, our study is retrospective so we do not have all preoperative clinical measurements to compare with postoperative values due to missing files. Second, we have a small number of patients. Third, we have a short-term postoperative follow-up. We hope to share long-term results of this new technique in future with more number of patients.
ECRL tendon ball arthroplasty for treatment of late-stage Kienböck’s disease has potential to provide satisfactory short-term outcomes for both clinicians and patients. We will continue to perform this technique and prospectively follow new patients for long-term results with larger number of patients.
Footnotes
Acknowledgment
The authors would like to thank Dr Erkay Nacar, Department of Public Health, Medicine Faculty of Inonu University, for his assistance with the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.