
Abstract
Purpose:
Our primary objectives were to create a reliable, noninvasive method for three-dimensional morphometry of deep bony parameters within the sigmoid notch of the distal radius, to identify its morphological patterns, and to identify any significant variation between the left and the right wrists. Our secondary objectives were to obtain morphometric values that could represent our population and to identify any possible ethnic variations.
Methods:
Computed tomography scans of 102 wrists from 51 healthy individuals were analyzed using a virtualization software. Four anatomical parameters at the distal radius sigmoid notch, namely, the radius of curvature, depth, version angle, and sagittal slope were measured. Morphological patterns of the sigmoid notch surface were identified. The results were statistically analyzed to assess the reliability of the technique and were compared with previously published literature.
Results:
Comparing our findings with previously published values, our study revealed a slightly larger radius of curvature and sagittal slope, while revealing a smaller depth and version. We identified the S-type, C-type, and ski-slope morphological variants. The flat-face morphological variant, however, was not identified. The sigmoid notch at the left and right wrists were similar, except for the radius of curvature.
Conclusion:
This study demonstrates a noninvasive, fast, reliable, and reproducible technique for analyzing the sigmoid notch of the distal radius. In wrist injuries with intact distal radius sigmoid notch but involving comminuted fractures of the ulnar head, ulnar head replacement may be indicated. In such cases, analysis of the ipsilateral intact sigmoid notch would allow us to prepare an ulnar head prosthesis of appropriate size.
Introduction
The rotation and stability of the forearm depends on the anatomical integrity of the proximal radioulnar joint, the interosseous membrane, and the distal radioulnar joint (DRUJ). DRUJ is a complex joint formed by the concave sigmoid notch of distal radius articulating with the convex ulna head. Distal radius fractures involving the DRUJ are complex injuries, wherein the management is often a challenge. A detailed understanding of the anatomical parameters at the DRUJ is important. Fractures involving the distal radius often result in the alteration of the biomechanics of the DRUJ and has a profound negative impact on long-term clinical results achieved, often resulting in post-traumatic arthritis. 1,2
Geissler et al. 3 discussed that the most common cause of residual wrist disability after fractures of the distal radius is the DRUJ. The radioulnar pain and limitation of forearm rotation are caused by three basic mechanisms, namely, DRUJ instability, DRUJ incongruency, and ulnocarpal abutment. The last two entities initiate irreversible cartilage damage that eventually leads to degenerative joint disease.
However, a literature review by Giannoudis et al. 4 of 36 articles for critical analysis related to intra-articular injuries of distal radius, acetabulum, distal femur, and tibial plateau concluded that the extent of articular displacement of various joints only weakly correlated with radiographic evidence of post-traumatic arthritis and patient outcome, and the authors suggested that different joints and even different areas of the same joint appear to have different tolerances for post-traumatic articular step-offs.
A recent study by Vitale et al., 5 compared the Disabilities of the Arm, Shoulder and Hand (DASH) scores in 33 patients with intra-articular distal radius fractures (19 with sigmoid notch involvement and 14 without sigmoid notch involvement). There was a trend toward DRUJ arthritis and poorer average DASH scores in those with sigmoid notch involvement, but this was not statistically different. In the sigmoid notch group, patients with >1 mm step-off in the coronal plane demonstrated poorer upper extremity function as measured by the DASH score (p < 0.05). No significant correlations were observed between sigmoid notch step-off, diastasis or DRUJ subluxation, and either Kellgren Lawrence grade of arthritis or DASH scores. Because of their limitation of small sample size, they recommended that further studies may be necessary to better identify the effect of DRUJ incongruity on patient outcomes and development of post-traumatic arthritis.
Variations in the radius of curvature of the sigmoid notch and that of ulnar head result in incongruency of their contact surfaces as discussed by Ekenstam and Hagert. 6 The angle between the contact surfaces varied with the degree of rotation of the forearm. The DRUJ is stabilized by the bony anatomy of the contact surfaces and augmented by numerous soft tissue stabilizers as described by Lawler and Adams. 7 The in vivo gliding and contact characteristics of the sigmoid notch and the ulnar head was studied by Chen and Tang. 8 The maximum sliding of the sigmoid notch over ulna was 7.4 mm in the forearm pronation and 9.2 mm in the forearm supination. Most of the motion occurred between 30° pronation and 60° supination. The contact site between the ulnar head and the sigmoid notch translated proximally 0.7 mm during supination and distally 1.6 mm during pronation. This demonstrates that the sigmoid notch translates significantly on the ulnar head during forearm rotation.
The anatomical parameters as well as the morphology of the sigmoid notch play an important role in the biomechanics and stability of the DRUJ. A study by Tolat et al., 9 involving 50 cadaveric wrists, described 4 morphological patterns of the sigmoid notch in the axial plane. These were the S-type, C-type, ski-slope, and the flat-face variants. The distal radius sigmoid notch was also studied by three-dimensional analysis of computed tomography (CT) scans of freshly frozen cadaveric hands, followed by anatomical dissection and analysis of the sigmoid notch, in a more recent study by Collins and Vossoughi. 10 They published their mean values for the radius of curvature, depth, version angle, and sagittal slope of the sigmoid notch.
Materials and methods
We performed an analysis of CT scans of both wrists of 51 volunteers (27 females, 24 males), none of whom had any previous history of wrist trauma or infection. All the volunteers were free of any clinical symptoms at both wrists. A total of 102 wrist CT scans were analyzed. Medical Ethics Committee approval had been obtained prior to performing the CT scans on healthy volunteers (University of Malaya Medical Ethics Committee approval no. 714.7). All selected individuals had no previous history of trauma or any deformities of their wrists. They were aged between 24 years and 45 years, with a mean age of 30 years.
The CT scan data were analyzed using Mimics® version 17 (Materialise, Belgium) to obtain measurements of four parameters at the distal radius sigmoid notch, namely, the radius of curvature (Figure 1(a)), depth (Figure 1(b)), version angle (Figure 1(c)), and sagittal slope (Figure 1(d)). The measured values were compared to those reported from the previous cadaveric study by Collins and Vossoughi 10 and Daneshvar et al. 11 We also identified the sigmoid notch morphological patterns in our samples and compared them to those reported by Tolat et al. 9

(a) The radius (R) of the best fit sphere (shaded red) provides the approximate radius of curvature of the sigmoid notch of distal radius. (b) The depth of the sigmoid notch (blue line), measured by the perpendicular distance between the line connecting the volar and dorsal lips of sigmoid notch (line A) and the line passing tangential to the deepest part of the sigmoid notch (line B). (c) The sigmoid notch version angle (area shaded red) is the angle formed by the line connecting the volar and dorsal lips of the sigmoid notch (line A) with the tangent from the dorsal lip to the sigmoid notch surface (line B). (d) The line C denotes the anatomical axis of radius. Line A is parallel to line C. The line B is a tangent along the articular surface of the sigmoid notch in midsagittal plane. The angle formed between the lines A and B displays the sigmoid notch sagittal slope (area shaded in red).
Finally, we compared the measured parameters between the right and the left wrists. We believed that if the parameters were comparable at both sides, then the CT scan analysis of the contralateral sigmoid notch and ulnar head would be beneficial in preoperative planning and implant selection where sigmoid notch reconstruction or ulnar head replacement may be necessary.
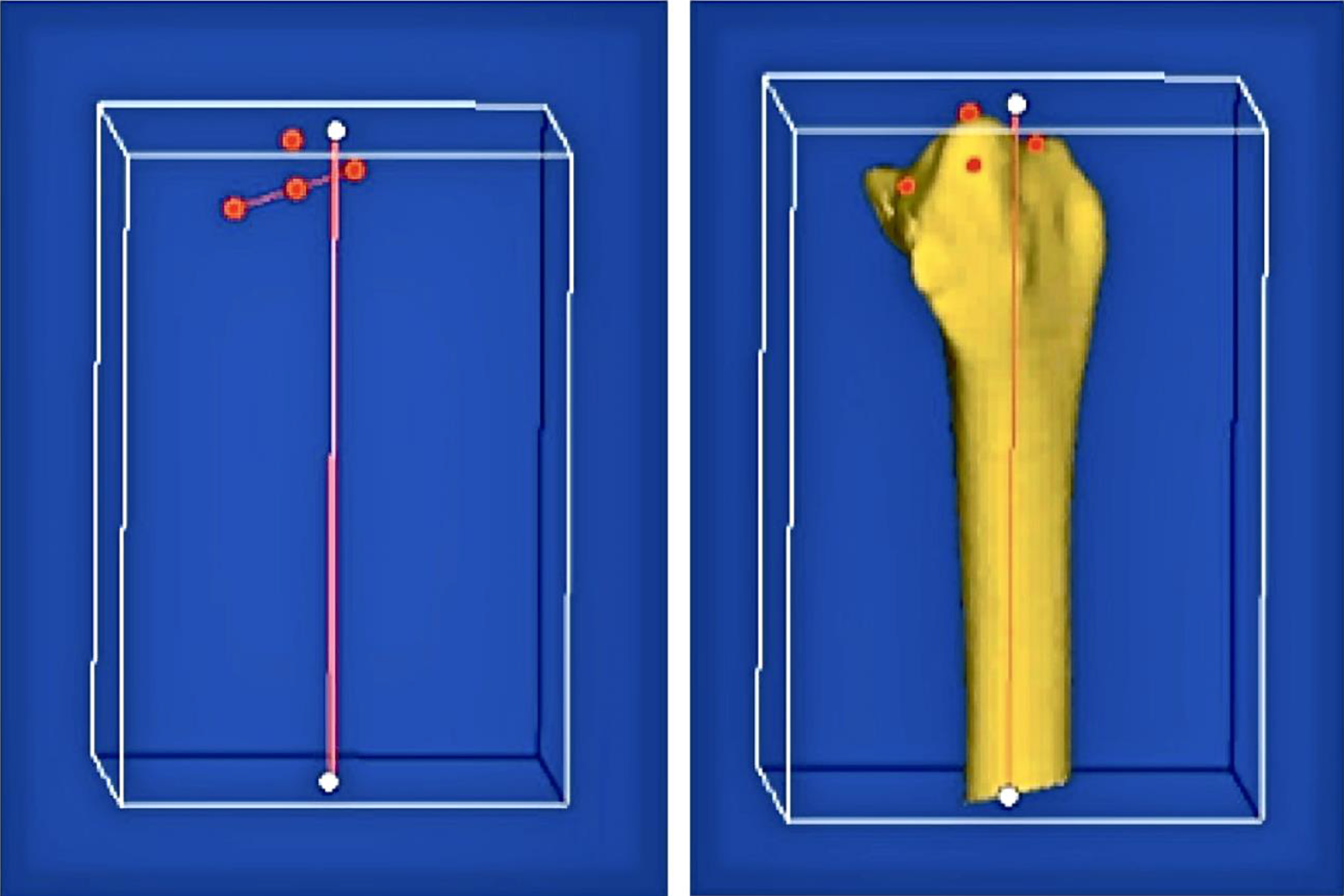
The CT Digital Imaging and Communications in Medicine (DICOM) files were imported into Mimics version 17.0 (Materialise). The DICOM files were then converted into high-resolution three-dimensional Mimic image files. As the study focused on the sigmoid notch of distal radius, the carpal bones and ulna were excluded, isolating the radius (Figure 2). The position of the forearm rotation had not been standardized at the time when CT scans were performed. Furthermore, the lengths of forearms included in the scans were variable. Due to this, the radius from all 102 scans had to be aligned on a standard plane of reference, before we could start taking measurements of the parameters. A “plane of reference” was thus defined, based on the distal bony landmarks such as tip of the radial styloid process, the dorsal and volar lips of the sigmoid notch of the distal radius, and the anatomical axis of radius (Figure 3).

The carpus and ulna were excluded, and the radius was isolated.
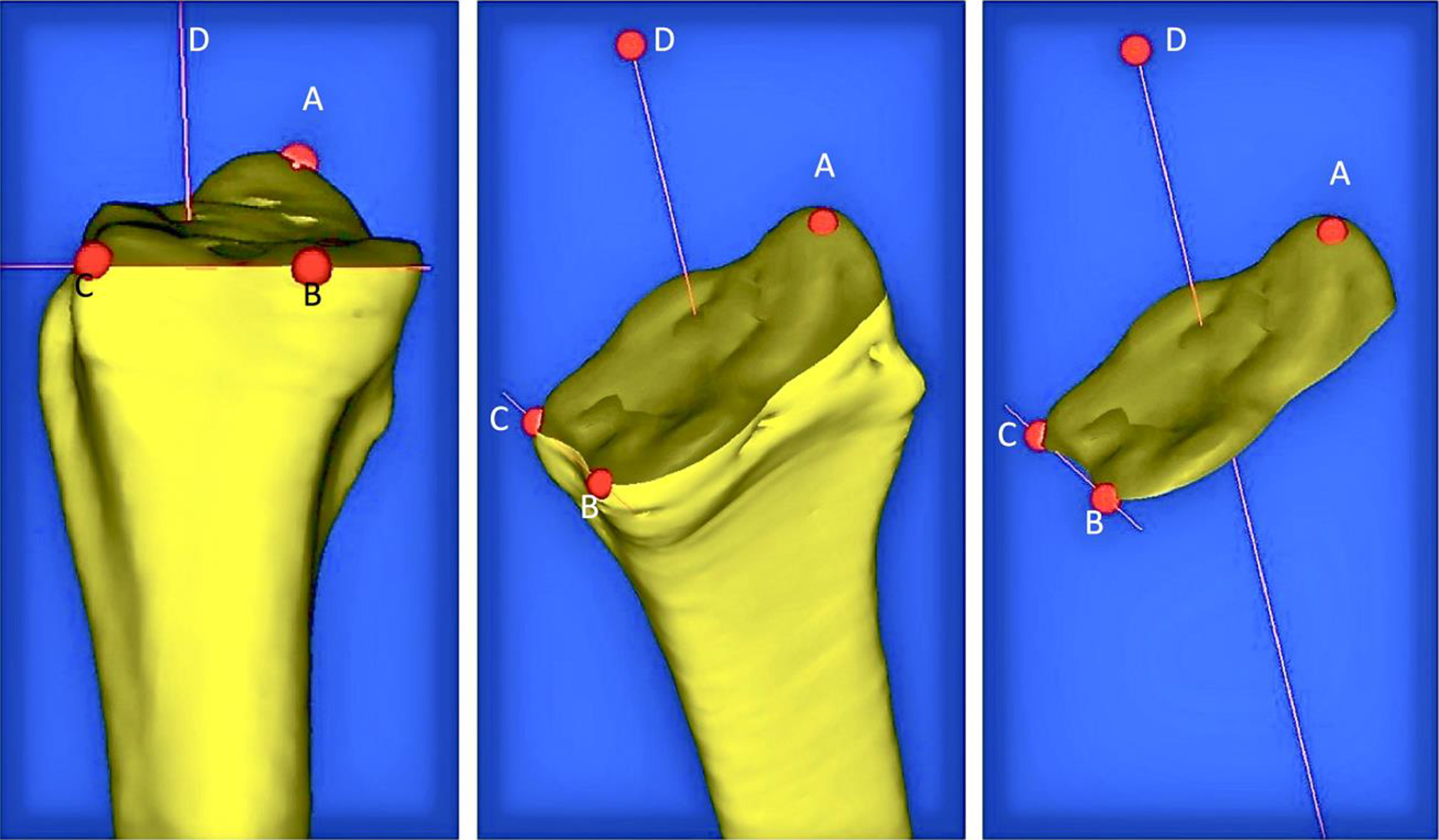
Tip of radial styloid process (A), sigmoid notch volar lip (B), sigmoid notch dorsal lip (C), and anatomical axis of radius (D) were used as anatomical landmarks.
Orientating the radius on a standard plane of reference, allowed the positioning of the radius to be reproducible, thus minimizing the errors in the measurement of the parameters. The correct orientation of the radius in coronal, sagittal, and axial planes was ensured (Figure 4). Using the MedCAD tools available within the Mimics software, four anatomical parameters were measured for each wrist: radius of curvature (Figure 5(a)), depth of notch (Figure 5(b)), version angle (Figure 5(c)), and sagittal plane slope (Figure 5(d)). In the axial plane, the morphological pattern of the sigmoid notch was assessed to identify the morphological variant. Based on this, three morphological variants of the sigmoid notch were identified: S-type (Figure 6(a)), C-type (Figure 6(b)), and Ski-slope (Figure 6(c)).
The distal radius was aligned on a standard plane of reference, allowing reliable measurements to be taken.

(a) Radius of the sphere represents the radius of curvature of the sigmoid notch. (b) Depth of the sigmoid notch (red line) obtained by the perpendicular distance to the deepest portion of the sigmoid notch from the line connecting the volar and dorsal lips of the sigmoid notch. (c) Version angle of notch is the angle formed by the line connecting the volar and dorsal lips of the notch, with a line that is tangential to the articular surface of the sigmoid notch. The angle is centered on the dorsal lip of the notch. (d) Sagittal slope was determined by an angle formed by the vertical line to the tangent along the articular surface of notch on the coronal plane.

Morphological patterns of the sigmoid notch: (a) S-type notch, (b) C-type notch, (c) Ski-slope notch.
Results
All four morphological parameters were measured in each of the 102 wrists. We identified three morphological variants of the articular surface of the sigmoid notch in the axial plane: the S-type (52%), C-type (26.4%), and ski-slope (21.6%). The flat-face variant was not identified. The mean measured values of the four anatomical parameters for each of the three morphological variants were as displayed (Table 1). The C-type notch was noted to be the deepest, with the lowest sagittal slope. The ski-slope variant had the largest radius of curvature but was the shallowest, with the lowest version angle and the highest sagittal slope.
The mean values of the four parameters for each of the three morphological variants.a

SD: standard deviation.
a Values are displayed as mean (SD).
The measured values were then analyzed for variations between the right and the left wrists (Table 2), with a statistically significant difference set at a p value <0.05. A power analysis was performed by comparison of two means, using G Power software version 3.1.9.2, which revealed that the number of wrists analyzed were sufficient to identify overall variations in measurement of parameters between the left and the right wrists. The mean radius of curvature was significantly higher on the left side, contributed by the larger number of the ski-slope variant on the left side (Table 3). The version angle, depth, and sagittal slope of the sigmoid notch were comparable on both sides. However, data were not correlated between dominant and nondominant hands. Subsequently, 20 wrist CT scans were randomly selected, and measurements were repeated by the principal and second investigators to assess intra-observer and interobserver correlations. The internal consistencies in the intra-/interobserver measured values were statistically analyzed by calculating Cronbach’s α (Figure 7).
Comparison of parameters at both sides.a
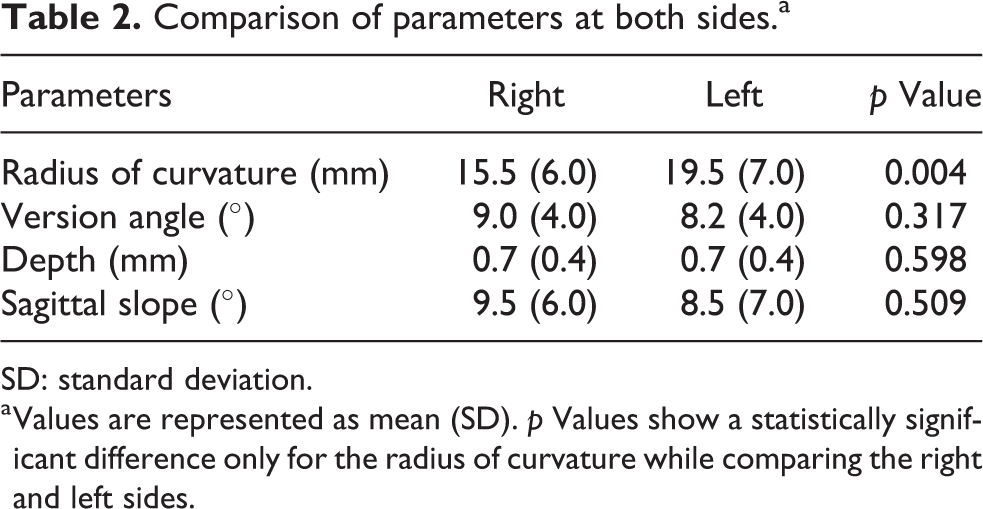
SD: standard deviation.
a Values are represented as mean (SD). p Values show a statistically significant difference only for the radius of curvature while comparing the right and left sides.
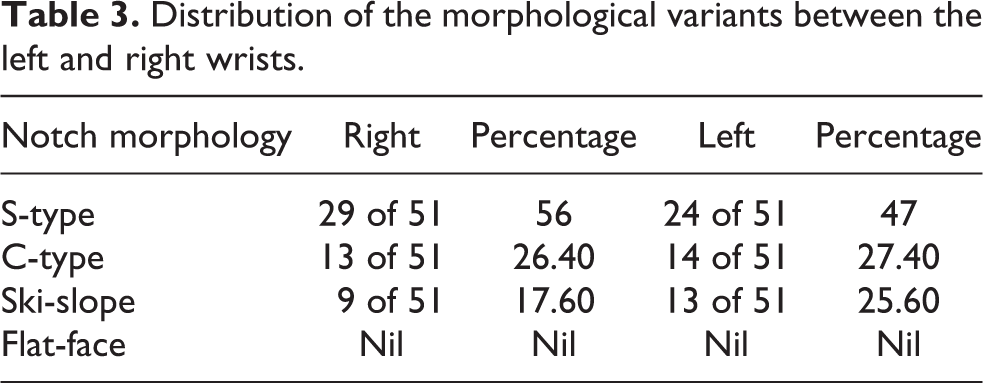
Distribution of the morphological variants between the left and right wrists.
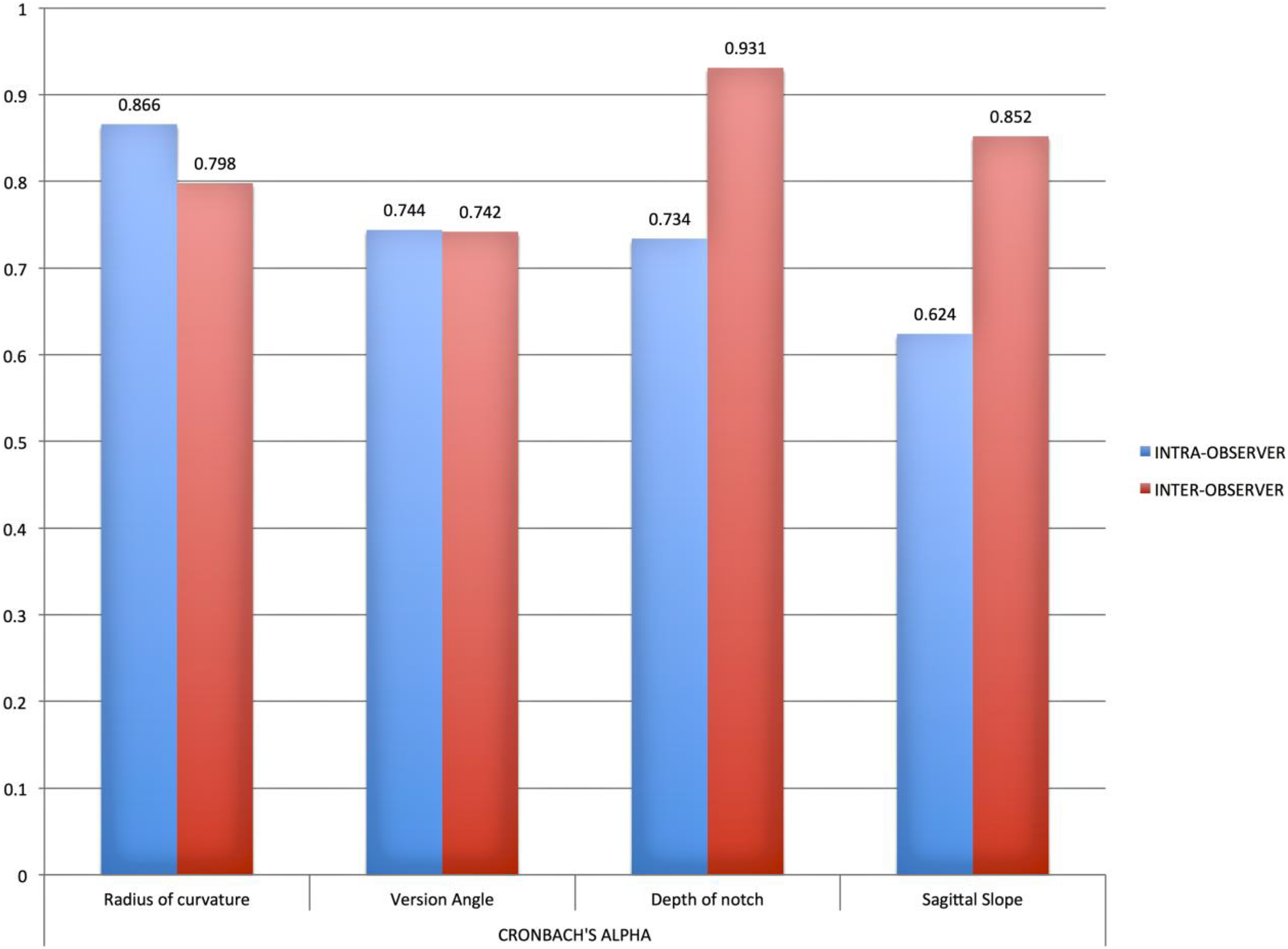
Cronbach’s α values showing the consistency in the intra-/interobserver correlation for each of the four measured parameters. Cronbach’s α ranges from 0 to 1, with value >0.7 indicating a good reliability of the method.
We found a good internal consistency in the measurement of all parameters, with the exception of the sagittal plane slope. We attribute this to the lack of visualization of the articular cartilage at the sigmoid notch, on the CT scans. This made it difficult to ascertain the exact proximal articular extent of the sigmoid notch on the coronal plane.
Discussion
Through this study, we managed to reliably measure anatomical parameters as well as morphological variants at the distal radius sigmoid notch. In the anatomical study by Tolat et al., 9 of the 50 cadaveric wrists, four shapes of the articular surface of the distal radius sigmoid notch were identified, the flat-face (42%), C-type (30%), S-type (14%), and ski-slope (14%) variants. By comparison, our study of 102 wrists revealed S-type (52%), C-type (26.4%), and ski-slope (21.6%) variants. We did not identify the flat-face variant in our samples. This could likely have been due to the limited number of wrists we studied and does not necessarily mean the absence of the flat-face variant in our population.
We compared our values with the study by Collins and Vossoughi. 10 Their values published were 14.6 mm (radius of curvature), 1.67 mm (depth of notch), 9.8° (version angle), and 1.64° (sagittal slope). By comparison, the values we obtained (Table 2) revealed a larger but shallower sigmoid notch. The version angle was comparable. However, the sagittal slope obtained in our study is larger than that obtained by Collins and Vossoughi 10 and comparable to 8° obtained by Sagerman et al. 12
Our measured values were also compared to those published by Daneshvar et al. 11 In their study, radius of curvature was 18.2 mm (SD 8.5 mm), and the mid-coronal angle of the sigmoid notch (slope in sagittal plane) was 6.0° (SD 9.9°), both of which were comparable to our results on the left side. However, their study involved measurements at the ulnar head, which was not included in our study.
Furthermore, our study did not include the effect of the articular cartilage over the sigmoid notch. While anatomical dissection was not an option in our study, this shortcoming could have been overcome by analyzing the wrists we studied, using an MRI. The effect of cartilage thickness at the sigmoid notch on inclination at the DRUJ was studied by Ross et al. 13 In their study, 100 wrists were analyzed using radiographs and MRI scans. No reverse oblique inclinations were found while analyzing the cartilage using MRI scans. A reverse oblique inclination of the articular cartilage may not be present on MRI even when bony sigmoid notch may show a reverse oblique configuration on plain radiograph, thereby removing one contraindication to ulna shortening osteotomy, where indicated.
We describe a quick and noninvasive method for performing morphometric analysis of an occult joint using CT scan images. We believe that in wrist injuries with intact distal radius sigmoid notch but involving comminuted fractures of the ulnar head, an ulnar head replacement may be indicated. In an acute setting, the excised comminuted ulnar head could still be measured for appropriate sizing. But in a chronic setting, however, measuring the excised ulnar head may be inappropriate due to malunion of the ulnar head. In such cases, analysis of the ipsilateral intact sigmoid notch would allow us to prepare an ulnar head prosthesis of appropriate size.
Conclusion
We believe that our method of analyzing and measuring is reliable, with reproducible results. However, our study did not include analysis of the ulnar head morphology. We could not evaluate the effects of the articular cartilage at the sigmoid notch as we did not couple our CT scans with MRI scans of the wrists. Furthermore, due to our small sample size, we were unable to deem our measured values to be representative of a population and identify ethnic variations. We feel a similar study could be performed on a larger sample size. This would enable identification of any significant variation in anatomical and morphological parameters, which may favorably affect the design of implants, better suited for a population.
Footnotes
Acknowledgments
The authors would like to specially acknowledge Professor Azhar Mahmood Merican, Head of Division of Joint Replacement, Department of Orthopaedic Surgery at University Malaya Medical Centre, for his guidance and technical assistance through this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.