
Abstract
Background:
For the treatment of acute Achilles tendon rupture, early rehabilitation after surgical repair is believed to be a useful method. The purpose of this study was to evaluate the outcome of open tenorrhaphy followed by early rehabilitation.
Methods:
A total of 112 patients who underwent open repair and early rehabilitation for acute Achilles tendon rupture from January 2003 to March 2015 were retrospectively reviewed. These 112 patients (80 men, 32 women) had an average age of 43.1 years (22–62 years), and the mean follow-up period was 91.8 months (12–171 months). A short leg cast was applied postoperatively for an average of 16.5 days (12–20 days). The mean duration of bracing was 6.9 weeks (6–8 weeks). Each patient was assessed based on range of motion, single heel raising test, calf circumference compared to the contralateral limb, ability to return to previous activity, the Arner–Lindholm scale, and the American orthopaedic foot and ankle society (AOFAS) hind foot scale. Isokinetic plantar flexion power was also checked.
Results:
All patients were fully satisfied (AOFAS ≥ 90) with the treatment results, and 96 patients were able to return to their previous athletic activities. As assessed by the Arner–Lindholm scale, 103 cases were rated as excellent and the other 9 cases were rated as good. At the 1-year follow-up period, single heel raise and hopping was possible in every patient. Compared to the contralateral side, 10 subjects (8.9%) had minor limitation of dorsiflexion motion, and an average of 1.6 cm calf circumference difference without functional disabilities. There were no major complications such as re-rupture, nerve injury, or infection.
Conclusion:
For acute Achilles tendon ruptures, open surgical repair with optimal length restoration, followed by earlier rehabilitation results in good functional outcomes and a successful return to pre-injury levels of physical activity without major complications.
Level of evidence:
Level IV.
Introduction
An increasing number of people are participating in high-activity sports. Coincidently, the number of reported Achilles tendon rupture patients is also rising every year. 1 The treatment for acute Achilles tendon rupture is still a hotly debated issue. The options for treatment include nonoperative treatment, traditional open repair surgery, mini open technique, and percutaneous repair. The traditional conservative treatment method is known to have a relatively higher re-rupture rate. 2,3 Recently, however, studies have shown that re-rupture rates in nonoperative treatment can be decreased by following a proper rehabilitation protocol. 2
The most important goal in Achilles tendon rupture treatment is that the patient should be able to return to their previous level of athletic activity, without re-rupture or tendon elongation. However, only around 60% of patients are able to return to their pre-rupture functional capacity. 4,5 The cause for such a low rate depends not on whether an operative or nonoperative treatment was performed but rather on how the patient was rehabilitated. The key points to consider during rehabilitation are when to permit full weight-bearing, how long to maintain the cast, and when to start active dorsiflexion range-of-motion (ROM) exercises. 2,3 When considering surgical treatment options, the advantages of open repair include lower rate of re-rupture, restoration of optimal length, and an earlier rehabilitation, which consequently lead to an expeditious return to daily activities. The purpose of this study is to provide guidelines for early rehabilitation after open Achilles tendon repair surgery.
Materials and methods
Patient demographics
From 2003 to 2017, 112 patients who underwent open surgical repair for acute Achilles tendon rupture were retrospectively reviewed. The diagnosis was based on a physical examination (Positive Thomson squeezing test, palpable skin dimpling of rupture site) 6,7 and medical history taking. All patients received open repair surgery (tenorrhaphy) and early rehabilitation. The mean follow-up period was 91.8 months (12–171 months).
The mean age of the patients was 43.1 years (22–62 years), and there were 32 female and 80 male subjects. The main cause of rupture was exercise (95 patients were injured while playing sports). The activities at the time of injury included foot-volleyball (31), soccer (24), tennis (13), badminton (9), basketball (6), baseball (2), and others (10). Other causes included slip down injury (15) and direct blow to the Achilles tendon (2). The average interval between the start of sports activity and Achilles tendon rupture was 27 min (5–120 min), and the average duration between injury and surgery was 4.3 days (1–10 days). The location of tendon rupture was on average 4.9 cm (3.3–7.9 cm) above the tendon insertion site. Cases of insertion site avulsion fracture of calcaneus, neglected rupture, or preexisting chronic tendinitis were excluded. Patients who had short term (<1 year) follow-up (8 cases) or simultaneous rupture of both Achilles tendons (1 case) were also excluded. Patient demographic data are presented in Table 1.
Demographics of patient characteristics.

Surgical management
The patient was positioned prone on the operating table. A pneumatic tourniquet was applied. According to the rupture gap, a 6–10 cm longitudinal incision was made on the medial side of the Achilles tendon. The tendon was repaired using one-strand Krackow suture technique using the absorbable PDS (polydioxanone, Ethicon, New Brunswick, New Jersey, USA, 40 mm). Additional surrounding suture was done using no 2-0 Vicryl at the repaired tendon. The key element of the operation was restoration of optimal length of the Achilles tendon. As a method of reference, the tension of the Plantaris tendon was compared. In 20 patients without the Plantaris tendon, the dorsiflexion angle of the contralateral ankle was measured preoperatively for reference. We also attempted to repair the paratenon surrounding the Achilles tendon. A short leg splint was applied in neutral position postoperatively.
Postoperative rehabilitation
The patient’s limb was placed in a short leg splint or cast with a neutral ankle position for 2 weeks after tendon repair. Immobilization with neutral ankle position was more suitable than plantar-flexed ankle position for weight-bearing walking exercise. Around 2–4 days after surgery, tolerable weight-bearing ambulation using crutches was permitted. The cast was replaced with a customized, below-the-knee walking brace 2 weeks postoperatively, and full weight-bearing ambulation with the brace was allowed. The brace had an adjustable ROM of the ankle joint, from 0° to 45°, adjustable in 5° increments (Figure 1). For the first 3 weeks after applying the brace, dorsiflexion was restricted to 0°, while full plantar flexion was allowed. During the next 3 weeks, dorsiflexion was restricted to 10° with free plantar flexion. Patients were encouraged to perform self-exercise with the theraband frequently during the daytime for plantar flexion strengthening exercise without the brace. In addition, muscle strengthening exercise of the quadriceps, hamstring, and hip abductor muscles with the brace applied was encouraged. At the 8th–10th weeks postoperatively, after removal of the brace, the patients were encouraged to perform indoor cycling, single leg stance exercise, and both heel or single heel raising exercise depending on the patient’s performance. At the 10th–12th weeks postoperatively, dorsiflexion exercise and frictional massage of calf muscle and repaired tendon were encouraged. Twelve weeks postoperatively, the patients underwent single leg standing on the form pad and soft pad to recover proprioception (Table 2). 8,9

Ankle brace with adjustable range of motion.
Postoperative rehabilitation protocol.

Clinical evaluation
At 1-year postoperatively, physical parameters such as the calf circumference and ankle ROM (plantar flexion and dorsiflexion) were assessed. The calf circumference at the widest level from the heel was measured with the ankle in the neutral prone position. The calf circumference and ROM were measured by two orthopedic doctors, and the mean measurement by the two different doctors was used in this study. The calf circumference and ROM were compared with those of the contralateral side. Also, the patient’s ability to perform a single-limb heel raise, hopping, and return to preoperative activity levels was checked. Patients were evaluated using the AOFAS score, the Arner–Lindholm scale (which takes into account functional discomfort), muscle strength abnormalities, and ankle ROM. The results are divided into excellent, good, and poor (Table 3). 10 Postoperative isokinetic plantar flexion power was also measured in 34 patients using the CYBEX770 (CYBEX) at a mean follow-up of 19.8 months (ranging 12–30 months). Fifty-seven patients who surpassed the 1-year follow-up period, but were unable to attend the scheduled hospital appointment in person, were contacted via phone and were asked to answer a questionnaire that mainly assessed the patient’s functional capabilities.
Arner–Lindholm scale for evaluation of acute Achilles tendon rupture.

PF: plantar flexion; DF: dorsiflexion.
To evaluate for any complications, all incidences of re-rupture, nerve injury, and wound infection were assessed.
Statistical analysis
Paired t-test was used to determine the statistical significance of factors such as calf circumference, dorsiflexion angle, and the cybex results compared to the contralateral side. All data were analyzed using the IBM SPSS statistics version 12 (Copyright IBM Corporation(s) 1989, 2012). The statistical significance level was set at a p < 0.05.
Results
Postoperative physical findings
Every repaired tendon healed without re-rupture or infection. Compared with the uninjured contralateral side, there was no difference in ROM in 102 of the 112 patients. Dorsiflexion deficit of less than 5° was observed in 10 patients (8.9%), and there were no cases of hyper-dorsiflexion due to overlengthening of the Achilles tendon. There were no cases of plantar flexion limitation or hyper-plantar flexion. Calf circumference decreased by an average of 1.6 cm (0.5–4 cm) on the injured ankle when compared with the normal calf. Most of the repaired tendons thickened, but no patient complained of pain of the thickened tendon site at the last follow-up period.
Functional results
All patients were able to walk normally without pain. At 3 months postoperatively, 87 patients were unable to perform single-limb heel raise. However, the ability to perform single heel raise was achieved in all patients 6 months after surgery. In an isokinetic study at a peak torque of 30° s−1, mean plantar flexion power deficit of 16% (range 0–21%) was seen compared to the contralateral side at the mean follow-up period of 19.8 months (12–30 months). Even with the deficit of plantar flexor torque seen in the isokinetic study, single heel raise was possible in all patients (Tables 4 and 5).
Functional results and isokinetic measurements for plantar flexor torque.

AOFAS: American orthopaedic foot and ankle society.
Functional results between normal power group and plantar flexion power deficit group.
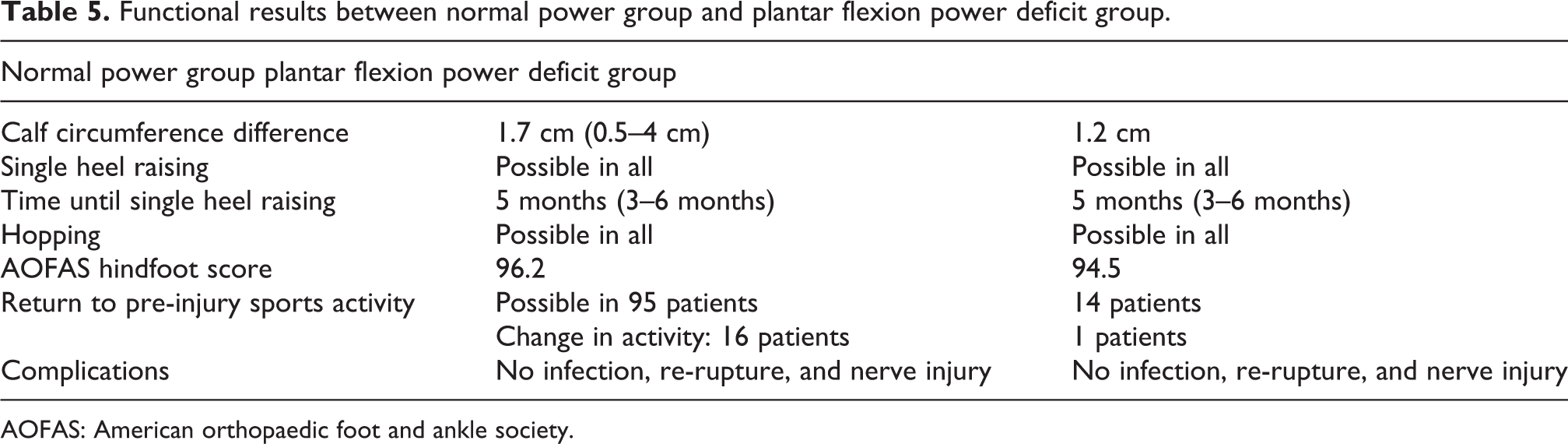
AOFAS: American orthopaedic foot and ankle society.
The AOFAS scores of the patients were all fully satisfactory (95.7). According to the Arner–Lindholm scale, 103 patients were rated as excellent and the other 9 patients as good.
At the last follow-up, return to pre-injury levels of sports activity was possible in 96 patients (86%). Sixteen patients changed their main sports activity because of knee pain (2 patients), fear of re-rupture (4 patients), or busy personal schedule (10 patients). Activities the patients began engaging in included jogging (25), foot-volleyball (19), soccer (11), tennis (10), hiking (9), swimming (6), golf (6), basketball (4), baseball (1), and fencing (1). The earliest return to sports was a patient who was able to play tennis just 10 weeks after surgical tendon repair. No patient experienced major complications such as infection, re-rupture, or sustained nerve injury.
Discussion
There has been controversy regarding whether to treat Achilles tendon injury conservatively or surgically. In the modern age where the popularity of active physical sports continues to grow, the general public is becoming more interested in sports-related injuries and how fast the recovery will be. In line with this trend, recent focuses of Achilles tendon rupture treatment tend to aim for earlier and quicker return to pre-injury levels of physical activity.
The numerous surgical options for tendon repair include open repair, mini open technique, and even percutaneous repair. Open repair typically show the highest durability but also has a higher risk of wound infection. Mini open and percutaneous methods have lower rate of infection, but some reports have highlighted an increased incidence of potential sural nerve damage and re-rupture rate due to difficulty in performing suture firmly connecting the edges exactly end to end. 11 Recent studies have shown that no matter which of the abovementioned three surgical technique was applied, there was no difference in functional outcome or patient satisfaction. 12,13
Conservative treatment usually consists of applying a cast for a set period of time. While this has the distinct disadvantage of a higher re-rupture rate, the advantages include lower rate of infection, avoidance of nerve injury, and cheaper medical costs.
According to Bae et al., who performed complete excision of tendon in patients who experienced postoperative infection after Achilles tendon surgery, rehabilitation and restoration of function were possible even though no additional tendon transfer was performed on the site of the removed tendon. 14 Mounting evidence suggests that in acute Achilles tendon rupture, conservative treatment can be a treatment option.
The major goal of Achilles tendon rupture treatment is symptom relief, recovery of normal gait, and restoration of adequate tendon length and muscle power, all in order to return the patient to their previous levels of physical activity. Recent treatment methods have focused on making this recovery as early as possible, and thus early rehabilitation was commonly utilized.
Regardless of whether the acute injury was surgically or conservatively managed, the traditional method of rehabilitation is to apply a short leg cast for 6 weeks. This method is based on the concept of a hematoma forming on rupture site, which then aids tendon healing with its copious supply of collagen fibers. 15 –17 But prolonged immobilization results in calf muscle atrophy, muscle weakness, loss of motion, deep vein thrombosis, skin necrosis, ankle contracture, and a higher re-rupture rate. When applied for 6–8 weeks, cast immobilization resulted in functional decrease ranging from 10%, 18 to 13–20%, 19 and to 12–15%. 20 Taking this into account, our subjects had their casts removed after 2 weeks and prompt rehabilitation was performed.
Many recent studies have revealed that early ROM exercises and early weight-bearing yielded better functional results and higher patient satisfaction. 21 Mortensen et al. 22 compared two groups, 8 weeks cast versus 2 weeks cast, followed by early ROM using an ROM-walker brace. The Early ROM group had less muscle atrophy, less tendon adhesion, and a higher rate of patients returning to previous physical activities.
Dorsiflexion of the ankle joint has the effect of increasing the force applied on the Achilles tendon, which can lead to elongation or even re-rupture. By using an adjustable orthotic brace, which limits ankle dorsiflexion for around 8–10 weeks until restoration of optimal strength, we prevented possible tendon elongation and re-rupture.
The role of early weight-bearing is also of fundamental importance, as it influences not only the treatment results but also the patient’s self-care ability. Two reports have evaluated the effect of weight-bearing in the treatment of acute Achilles tendon rupture. Costa et al. 23 concluded that early weight-bearing rehabilitation resulted in quicker return to walking and stair climbing in surgically treated patients, but not in nonoperatively treated patients. Suchak et al. reported that patients who underwent early weight-bearing exercises had a higher degree of satisfaction with the treatment. 1
In most studies, postoperative ankle position was aligned at the plantar flexion position during casting or orthosis. Re-rupture occurs at the time of transition from plantar flexion position to dorsiflexion (6–8 weeks after treatment) does not occur and after 3 months. However, in this study, the neutral ankle position was preferred rather than the plantar-flexed position because it allows earlier full weight-bearing, and the risk of re-rupture at the time of weight-bearing could be reduced. Ecker et al. reported that re-rupture occurs 6–8 weeks after treatment. 24
The CYBEX770R (Cybex International Inc., Medway, MA, USA) instrument was used to evaluate the patient’s power and endurance. Previous studies have utilized isokinetic assessments, but no standard protocol has been established. The Cybex instrument is commonly and widely used to objectively assess muscle strength after Achilles tendon repair. Patients who received repair surgery showed little discomfort when performing daily activities, but showed limitations during sprinting or jumping exercises. For these motions to occur, the muscular contractions and strength of the ankle plantar flexors are crucial. In our study, the plantar flexor muscle power was decreased by 16% and 25% when the angular velocity was 30 and 120, respectively. In the Cybex study, the lower angular velocity is used to assess maximum muscle power, and higher angular velocity is used to assess required muscle strength during rapid joint movement. Patients complained of pain during instances of rapid joint movement than during daily activities. Considering the fact that an 80% recovery of isokinetic muscle strength is used as a benchmark for determining when to return to sports activities, our subjects had an optimal isokinetic muscle strength recovery rate and subsequently a satisfactory return to physical sports. However, the Cybex results did not show a meaningful correlation with other clinical parameters. Although isokinetic tests using Cybex are the most widely used method following Achilles tendon repair, its results are simply a value of measurement and does not completely reflect the patient’s satisfaction or clinical outcome.
One study reported the rate of wound infection after Achilles tendon open repair as between 0.2% and 3.6%. 25 To reduce risk of infection, many attempts have been made using the mini open and percutaneous methods, but while this may have lowered infection rates, the incidence of nerve injury has increased. 10,20 In our study, we have made diligent efforts to repair the paratenon and cover the synovium in addition to the ruptured tendon during open repair. In all our subjects, there was no postoperative infection or nerve injury.
The limitations of this study are that a comparative study with patients who received nonoperative treatment with early function rehabilitation. Additionally, the Cybex test was not performed on all patients.
Conclusion
For acute Achilles tendon ruptures, open surgical repair that achieves optimal length, followed by early weight-bearing and active rehabilitation, results in good functional outcomes and a successful return to pre-injury levels of physical activity, without major complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.