
Abstract
Background:
Congenital pseudoarthrosis of the clavicle (CPC) is rare and may require treatment, usually because of an unacceptable appearance or occasionally because of pain in an adolescent patient. Spontaneous union is unknown, and consequently any desired union requires open reduction and bone grafting. Many authors recommend performing the operation at the age of 3–5 years and using different fixation methods. We present our experience with three cases and literature review in an attempt to further elucidate the appropriate timing of the procedure and the fixation method.
Methods:
This was a retrospective review of three cases presenting with pseudoarthrosis of the clavicle. All cases were treated by curettage of the pseudoarthrosis, with the void filled using full-thickness ileac crest autologous bone graft and bridging plate—one compression and two anatomical, at different ages. We performed a literature review with emphasis on timing of the procedure, fixation method and complications.
Results:
All patients healed with good callus formation. One patient (5-year-old female treated using a compression plate) experienced overlying skin irritation and underwent removal of the plate. There were no restriction of movement, pain or any other complaint on the final follow-up. We did not find any difference in the operating complexity at different ages, but when a compression plate was used, it had to be removed later due to bulging of the plate.
Discussion:
No clinical difference was observed between earlier and late operation. Therefore, we suggest performing a curettage of the pseudoarthrosis, gapping the void using autologous bone graft, and using an anatomical bridging plate.
Background
Congenital pseudoarthrosis of the clavicle (CPC) is rare, first reported in 1910 by Fitzwilliams, 1 and so far around 200 cases have been reported worldwide.
As the name suggests, CPC is present at birth and usually occurs in the middle third of the right clavicle. Differential diagnoses include acute fracturing of the clavicle at birth, neurofibromatosis and cleidocranial dysostosis. 2 The function of the shoulder is not impaired, although a non-aesthetic and at times painful deformity or rarely thoracic outlet syndrome may occur during and/or after the growth period. 3
CPC may require treatment, usually because of an unacceptable appearance or occasionally because of pain in an adolescent patient. 4 Spontaneous union is unknown, and consequently, any desired union requires open reduction and bone grafting. Most surgeons agree that the ideal time for grafting is between 3 years and 5 years. Although grafting can be done at any age, according to some authors—the older the patient is, the more difficult the procedure. Simple resection of the prominent ends of the bone will result in pain, prominence of the ends during movement of the shoulder, and asymmetry of the shoulder girdles. 2
The type of fixation used varies in the literature: different plates (reconstruction, compression, or anatomical) and screws, screws alone, Kirschner wires (KW), fully threaded pins, Steinmann intramedullary pins, and external fixation. Following the operation, very few complications have been described: synthesis material fail, 3 pain and weakness in the operated limb, 4 lack of consolidation, 5 and superficial infection and neuropraxia of the brachial plexus. 6
In this study, we present a retrospective review between 2002 and 2014 of three patients who presented with the condition, were treated in our ward and were followed up for outcomes and literature review focus on the surgical timing and fixation method.
Methods
The cases reviewed were of a 5.5-year-old female, a 4-year-old male, and a 7.5-year-old male (Table 1). All cases were referred by a family physician for further evaluation due to cosmetic reasons (Figure 1), and all patients received treatment by a single orthopedic surgeon. At follow-up, the patients were interviewed and physically checked by the operating surgeon. The range of movements of the shoulder, visual analog score, and operative wound and cosmetic appearance were recorded. X-Ray of the clavicle was taken, and the patients were asked about their general satisfaction with the outcome.
Demographic and clinical data at presentation.


Clinical picture of the pseudoarthrosis of Patient 3.
We performed the literature review in the MEDLINE database using the descriptors pseudarthrosis, congenital, and clavicle. We found 126 articles published till April 2016, of which 85 were single-case reports. The articles were reviewed by two orthopedic surgeons separately and then only articles in English (and one in French) that included description of the case, type of the surgical procedure performed, and type of outcomes were included (Table 2).
Literature review and summary.

Operative technique
All cases were treated by excision of the pseudoarthrosis. After performing a direct supero-anterior approach to the clavicle with a longitudinal cut, the pseudoarthrosis was identified and removed with a marginal resection of the normal bone (using a small jigsaw). The periosteum was also removed as in the treatment of pseudoarthrosis of the tibia. 18 After measuring the missing length of the clavicle, we harvested a matching length of full-thickness ileac crest autologous bone graft (Figure 2), and fixated using a bridging plate. The female patient was operated using a standard 4.5 mm limited contact dynamic compression plate (LC-DCP; Synthes [Canada] Ltd, Mississauga, Ontario, Canada) The two male patients were operated using an anatomical 3.5 mm clavicular plate (Synthes [Canada] Ltd) (Figure 3). All the patients were then fitted with a shoulder sling for 2 weeks, with tolerated allowed movement.
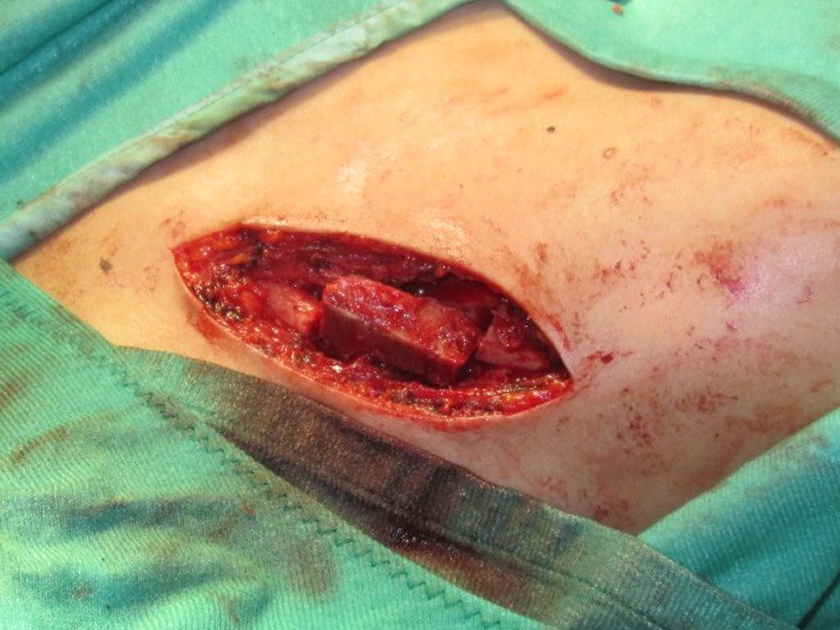
In theater—after removal of the pseudoarthrosis with the ileac autologous bone graft in place and before applying the bridging plate.

X-Ray 1 month postoperatively of Patient 2.
Results
At 1-month follow-up, all the patients healed with good callus formation, and there was no restriction of shoulder movement. At 1-month follow-up, the 5.5-year-old female patient with LC-DCP plating experienced an overlying skin irritation and discomfort. Therefore, the plate was removed. At 3 months after the initial operation, full healing of the pseudoarthrosis was achieved and the symptoms resolved. The two male patients (4 years and 7.5 years) with anatomical plates healed with no complaints and no skin irritation. All patients were satisfied with the final cosmetic result, and the scar “exchanging” the bulging clavicle was minimal. No other sequela was reported on the final follow-up at 6 years (female), 10 years (4-year-old male) and 1 year (7.5-year-old male) postoperatively (Table 3). In our literature review, we found 26 relevant articles, with 143 patients (of which 105 were treated operatively). Most cases were operated under the age of 6, but 15 cases (approximately 14.3% overall) were operated after the age of 9 years, 4,8,9,11,17 of which 4 were due to thoracic outlet syndrome, 15,19,22,28 one case following a traumatic dislocation, 31 and the rest were late presentations. Importantly, no adverse effects were reported in all these patients. Overall, 7 cases were treated with excision alone 4,12,19,20 ; 23 cases were treated with excision and bone grafting 4,12,20,23 ; 24 cases were treated with excision, bone graft, and KW or Steinman pinning 4,7,15,17,20,21,23,25,27,29 ; 7 cases were treated with excision, bone graft, and fully threaded pin 3,20 ; 9 cases were treated with excision, bone graft, and compression plate 9,11,20,22,25 ; 17 cases were treated with excision, bone graft, and reconstruction or Sherman plate 3,8,10,13,16,29,31 ; 9 cases were treated with excision and reconstruction or third tubular plate 26,29 ; 1 case was treated with excision, bone graft, and anatomical plate 28 ; 4 cases were treated with excision and compression plate 25 ; 2 cases were treated with excision and KW pinning 25,29 ; 1 case was treated with excision, bone graft, and screw fixation 14 ; and 1 case was treated with excision and external fixation. 30 In 11 cases, the plating was removed, and the reason was not specified 9,12,22 ; 5 cases suffered from pin tract infection 9,18,25 ; and in 1 case, the plate was removed due to prominence of the plate. 3
Clinical data at last follow-up.

ROM: range of motion; VAS: visual analog score.
a Refer to text for details.
Discussion
Our patients presented with bothering cosmetic appearance that prompted medical treatment, with no other medical complaint. Lorente Molto et al. 14 recommended early surgical treatment, citing good results in five children who were treated from 18 months to 4 years. Grogan et al. 32 reported the treatment of eight children. He suggested that early resection probably does not require the extensive grafting and internal fixation that are recommended for older children. Others reported good results even when the operation was performed at ages 19–20 years and even 48 years. 9,19,28 About 9.5% of cases were older than 9 years, and there were no additional complications reported compared to the younger cases. Our experience with three cases resulted in no clinical difference between earlier versus late operation as the surgeon did not report a more demanding procedure in the older patient.
Anatomical clavicular plates are relatively new, and fixation of the clavicle was performed using Kirschner wires, Steinman pins, compression plating, or reconstruction plating with various outcomes (Table 2). Of the 158 patients recorded, 31 were operated using nonanatomical plating (i.e. compression, reconstruction, etc.) and in 12 patients—39% of cases (approximately 7.6% overall) some complication was reported regarding the fixation method: in 11 cases, the plating was removed, and the reason was not specified; in one case, the plate was removed due to prominence of the plate. We performed an excision of the pseudoarthrosis, filling the void using an autologous full-thickness ileac bone graft and internal fixation. One case—treated with compression plating—was complicated with an overlying skin irritation, and so the plate was removed; we attribute this to the fact that the compression plate used was thicker than the anatomical plate (4.5 mm vs. 3.5 mm) as well as the fact that the compression plate, even if contoured, does not have an anatomical fit to the clavicle.
We acknowledge the weaknesses of our case studies by their retrospective nature. The follow-up of the cases and the treatment by a single surgeon may lead to treatment bias. As stated, CPC is very rare and we base our recommendations on our anecdotal experience and a literature review, and so should be approached with caution.
In the light of our experience with three cases and the literature review, we suggest that there is no clinical difference between earlier versus late operation. We recommend performing an excision of the pseudoarthrosis, filling the void using autologous bone graft, and using an anatomical bridging plate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.