
Abstract
Objective:
Intra-articular displaced calcaneal fractures are common fractures and are often treated with surgical interventions. Sinüs tarsi approach provides secure access to lateral wall and joint facets. The aim of the study is to compare cannulated screw (CS) fixation and mini-plate (MP) fixation via sinus tarsi approach with Sanders types 2 and 3 fracture of calcaneus.
Methods:
Sixty patients with Sanders types 2 and 3 calcaneal fracture underwent surgical intervention were randomly allocated into two groups as group MP fixation and group CS fixation regarding osteosynthesis method for 5-year period. Open reduction via sinüs tarsi approach was performed in both groups. Demographic variables, time to surgery (TS), operation duration (OD), length of hospital stay (LOS), surgical complications, and reoperations were recorded. Pre- and postoperative Gissane and Böhler angles; calcaneal length, height, and width; ankle anterior-posterior (AP) and lateral X-rays; and computed tomography were also recorded for radiological evaluation and fracture characteristics. Maryland Foot Score (MFS) was used to evaluate functional outcomes.
Results:
Preoperative age, type of fracture, calcaneal length, height, and Gissane and Böhler angles, TS, LOS, and OD were not different between the groups. The postoperative calcaneal widening was significantly better restored in group MP compared with that of group CS. The incidence of reoperation and algoneurodystrophy was statistically higher in group CS than group MP. MFS in group MP was also higher than group CS at final visit.
Conclusion:
MP fixation via sinus tarsi approach is superior to CS fixation in Sanders types 2 and 3 calcaneal fractures.
Introduction
As the most common type of fracture in tarsal bones, calcaneal fractures constitute up to 60% of all tarsal fractures. About three-fourth of these showed intra-articula displacement. Calcaneal fractures usually occur secondary to high-impact trauma such as fall from height or traffic accidents.
In intra-articular displaced fractures, the therapeutic aim is to establish anatomic reduction and subtalar joint alignment, to restore calcaneal width and height, and to prevent lateral impingement, 1 where the standard surgical method is open reduction and internal fixation via extensile L-shaped incision. Nevertheless, it is often associated with several problems that may predispose the patients to serious comorbidity such as postoperative hematoma, wound edge necrosis, wound dehiscence, or deep infection. On the other hand, minimal invasive interventions to reduce these soft tissue complications have become increasingly widespread: osteosynthesis with percutaneous cannulated screw (CS) and closed reduction, osteosynthesis with arthroscopically assisted screw, external fixator applications, and osteosynthesis with plate or CS through minimal invasive sinus tarsi approach. Despite a lower rate of complications, closed methods in particular might not provide sufficient reduction and stable fixation in displaced comminuted fractures. 1,2 In addition, calcaneal widening after fracture might not be sufficiently reconstructed with closed osteosynthesis, which may lead to the lateral impingement syndrome, that is, peroneal tenosynovitis. 2
Sinus tarsi approach is a minimal invasive technique that provides access to the subtalar joint and assessment of joint facets. 3 This approach not only reduces the duration of the surgery and the rates of soft tissue complications like percutaneous techniques, but also offers direct visualization of the calcaneal posterior facet and lateral wall. 4 Osteosynthesis in this approach is usually achieved with CS, plate, or a combination thereof. 5 –7
The aim of this study is to compare osteosynthesis methods performed either with CS or mini-plate (MP) in terms of pain, function, union time, and complications in patients with Sanders types 2 and 3 calcaneal fractures treated with minimal invasive sinus tarsi approach.
Materials and methods
The power analysis was conducted with a Power Analysis and Sample Size software package (NCSS, Kaysville, Utah), using simulation under Poisson distributions with Mann–Whitney U test and a target ≥ 0.05.
A total of 67 subjects who applied to our center between January 2012 and January 2016 with intra-articular calcaneal fractures were prospectively randomized to undergo either open reduction and CS fixation or open reduction and MP fixation, allocated into CS and MP groups, respectively. Random number generator (MedCalc 11.5.1 Seoul, Republic of Korea) was used in order to assign internal fixation method. Seven subjects who met exclusion criteria of being <18 years old, pathological or open fracture, Sanders type 4 or bilateral fractures, congenital foot deformity, lower extremity involvement of rheumatic or systemic condition (rheumatoid arthritis, diabetes, neuropathy, etc.), prior foot/ankle surgery, or unwillingness to accept allocated study treatment modality were excluded to the study.
Sixty patients with unilateral Sanders type 2 or 3 intra-articular calcaneal fractures were included to the study. A written informed consent was obtained from all the subjects. After being approved by the local ethics committee of our hospital, the study was performed in accordance with ethical principles set by 1964 Helsinki Declaration.
All patient data were evaluated preoperative, postoperative third week, and postoperative 1-year follow-up visit.
Surgical technique
Mini-calcaneus plate
Under spinal anesthesia, the subjects were put into the lateral decubitus position under ankle tourniquet whose pressure was set at 100 mmHg above the systolic blood pressure. A 4–6-cm straight incision extending from the tip of the fibula to the base of the fourth metatarsal bone was performed (Figure 1). Posterior facet was exposed by retracting extensor digitorum brevis proximally and peroneal tendons inferiorly (Figure 2). 8 The joint was restored by lifting the posterior facet fragment via the elevator. The Steinman pin introduced from the tuber calcanei provided correction of calcaneal varus, length, and width, which was fixed by temporary K-wires. 3 Spongious allografts were used in patients with excessive bone defects. After verifying calcaneal length, height, width, and Gissane and Böhler angles, anatomical calcaneal locked plate (Mini-Calc plate, Acumed, Hampshire, United Kingdom) was inserted in appropriate position under the guidance of C-Arm fluoroscopy (Figure 3). Spongious screws of 2.7 mm were delivered after passing through single cortex guided by the fluoroscopy (Figure 4). The layers were appropriately closed after placing a drain.

The skin incision of sinüs tarsi approach.

Lateral view of the displaced posterior calcaneal facet.

Lateral view of the calcaneus after open reduction and internal fixation with mini-calcaneus plate.

Pre- and postoperative AP and lateral X-rays of mini-plate fixation.
Cannulated screw
The patient was prepared under tourniquet in the same way as mentioned above, after which sinus tarsi incision was performed. Posterior facet was reduced by the same open fashion. After confirming calcaneal length, height, width, and Gissane and Böhler angles, two K-wires that allowed passage of CSs within were introduced from lateral calcaneus to the medial calcaneus through subchondral bone and two other temporary K-wires were introduced from tuber calcanei anteriorly under the guidance of C-Arm fluoroscopy. 9 Afterward, permanent osteosynthesis was acquired with 6.5- and 4.5-mm CSs (Figure 5). The layers were then appropriately closed after placing a drain.
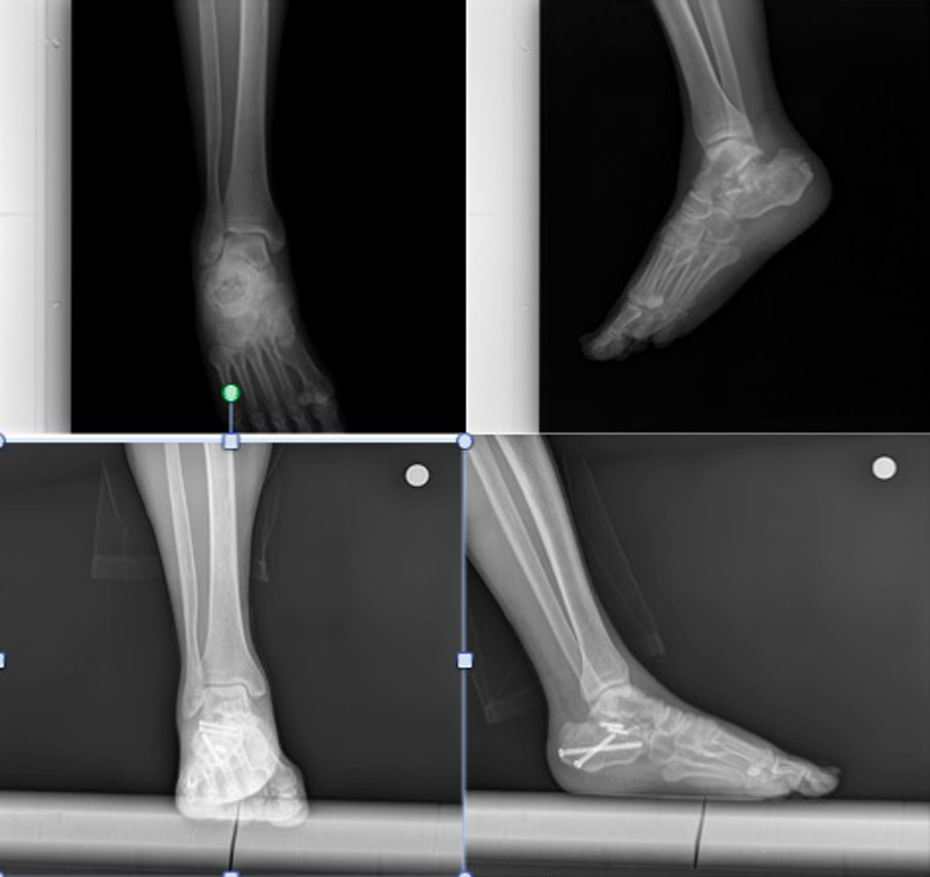
Pre- and postoperative AP and lateral X-rays of cannulated screw fixation.
Postoperative management
After removing Hemovac drain on postoperative day 2 in both groups, active and passive exercises of plantar flexion and extension were initiated. In group MP, partial weight-bearing was started with 5 kg in average for 30 min daily on the third week, where full weight-bearing was achieved around 12th week after fracture healing was confirmed radiologically. In group CS, partial weight-bearing was begun at sixth week as described by Abdelazeem et al. and Park et al. 10,11 Full weight-bearing was acquired after 12th week that featured signs of clinical and radiological fracture healing.
Pre- and postoperative Gissane and Böhler angles, calcaneal length, height, width, ankle anterior-posterior (AP) and lateral X-rays, and lateral and axial computed tomography were used for radiological evaluation and fracture characteristics. The normal values of Gissane and Böhler angle vary between 120°–145° and 20°–40°, respectively. 9 Fracture healing and radiologic parameters were assessed by two independent musculoskeletal system radiologists.
The two osteosynthesis methods were compared in terms of several parameters, including time to surgery (TS), the operation duration (OD), postoperative soft tissue infection and wound problems, length of hospital stay (LOS), and incidence of reoperation. Superficial wound dehiscence and wound site necrosis were accepted as minor soft tissue complications. 10 The lesions that had positive wound culture results and managed with nonsurgical modalities (oral antibiotics and dressing) were assessed as superficial wound infection, whereas those associated with osteomyelitis, colonized implant or removal of implant, or presence of fistula requiring debridement and/or parenteral antibiotics were regarded as deep wound infection. 12 Implant removal was indicated in the case of the implant failure and its penetration into the joint, or posterior heel pain that was refractory to medical treatment, or deep infection.
Maryland Foot Score (MFS) was utilized to evaluate functional outcomes at 1-year follow-up visit. 13 MFS of 90–100 was rated as excellent, 75–89 as good, and 50–74 as fair. The excellent and good results are accepted as satisfactory.
Statistical analysis
IBM SPSS Statistics 22 program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, minimum, and maximum) were used analyze data. Spearman’s correlation test was used to assess correlation between calcaneal widening and MFS. χ 2, independent samples t-tests were utilized for parametric values. p < 0.05 were assessed as statistically significant.
Results
There were 7 female and 53 male patients, with a mean age of 39.2 ± 12.0 years. All cases were divided into two groups as group MP (n = 31) and group CS (n = 29). None of the patients were dropped out during postoperative 1-year period. Group MP was consisted of 28 male and 3 female patients; group CS was 25 male and 4 female patients. The mechanism of the fracture was falling down from height in 54 patients (90%), compared with traffic accident in the remaining six cases. The study groups did not differ in terms of preoperative age, type of fracture, calcaneal length and height, and Gissane and Böhler angles, respectively (p = 0.824, p = 0.448, p = 0.813, p = 0.772, p = 0.752, and p = 0.453; Table 1). Additionally, preoperative Böhler and Gissane angles were restored to normal degrees postoperatively. Postoperative calcaneal height and length was also reconstructed Figure 6. The postoperative calcaneal widening was significantly better restored in group MP compared with that of group CS at immediate and final follow-up (p = 0.002 and p = 0.016, respectively; Figure 7). The correlation between calcaneal widening and MFS was not found statistically significant (p = 0.619).
Evaluation of preoperative and postoperative value of radiological parameters in group MP and group CS.a

SD: standard deviation; MP: mini-plate; CS: cannulated screw.
a Independent samples t-test. Preoperative, immediate postoperative, and final follow-up data of groups (p < 0.05 is shown in italics).
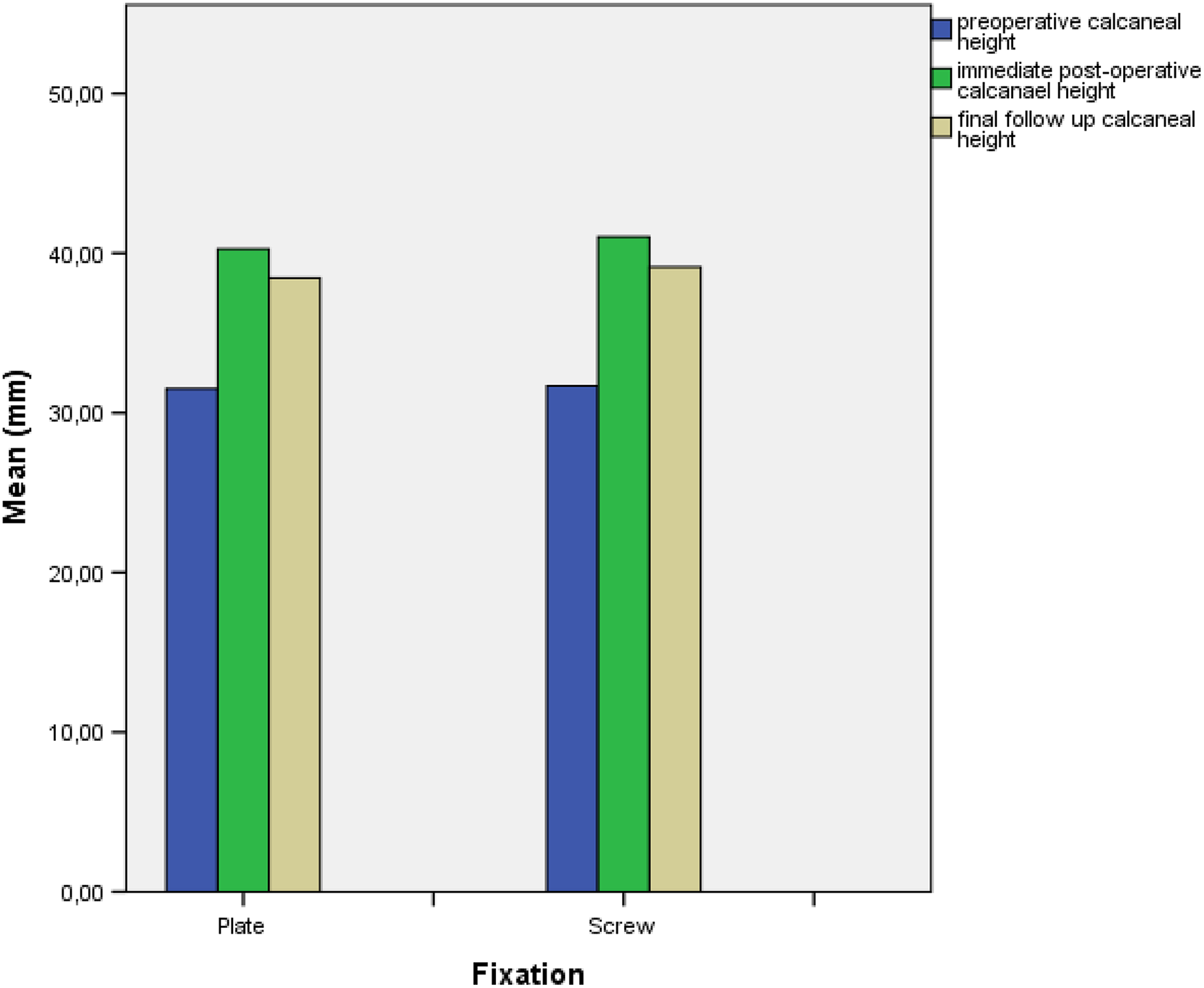
Evaluation of the calcaneal height before and after surgery.
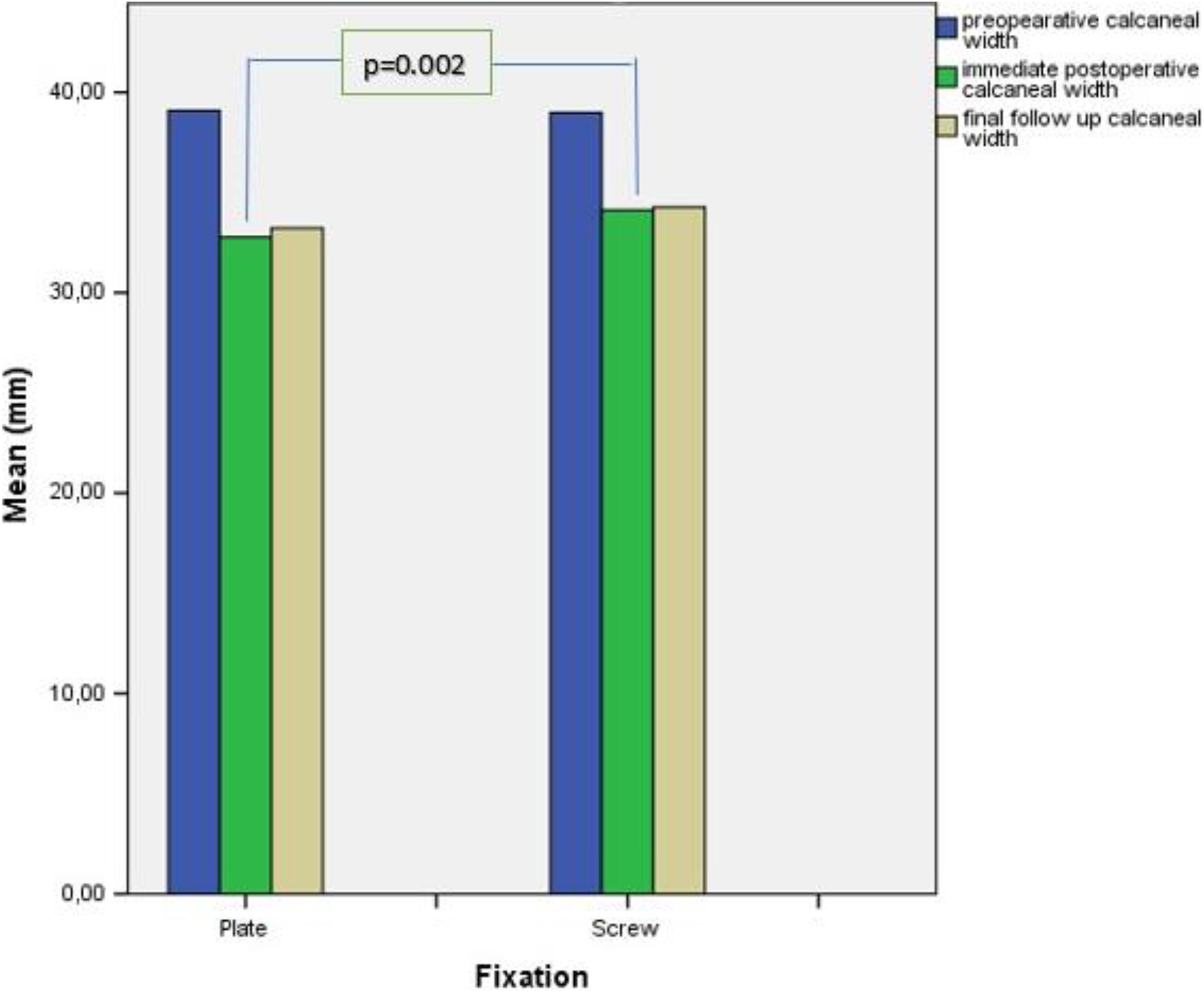
Comparison of pre- and postoperative calcaneal width in group MP and group CS.
The groups did not differ in terms of the TS, OD, and LOS (Table 2). Two cases of minor wound site problem were observed in each of the both groups, which were managed by dressing and medical treatment. No patient developed superficial or deep infection. Two cases with refractory heel pain, three cases with implant failure, and one case with screw penetration to talocalcaneal joint underwent implant removal in group CS. None of the patients in group MP underwent reoperation. The incidence of reoperation in group CS was significantly higher than the group MP (n = 6, 21%; n = 0, 0%; p < 0.008). One case in each group had temporary sural nerve lesion. Four patients in group CS and one patient in group MP developed algoneurodystrophy that responded well to the medical treatment and rehabilitation. The incidence of algoneurodystrophy in group CS (n = 4, 13.7%) was significantly higher than that of group MP (n = 4, 13.7%, n = 1, 3.2%; p = 0.0139; Table 3).
Comparison of age, TS, OD, and LOS of mini-plate and cannulated screw groups.a

SD: standard deviation; TS: time to surgery; OD: operation duration; LOS: length of hospital stay.
a Independent samples t-test. p < 0.05 is significant.
Comparison of reoperation, algoneurodystrophy, and Maryland Foot Score of the patients.
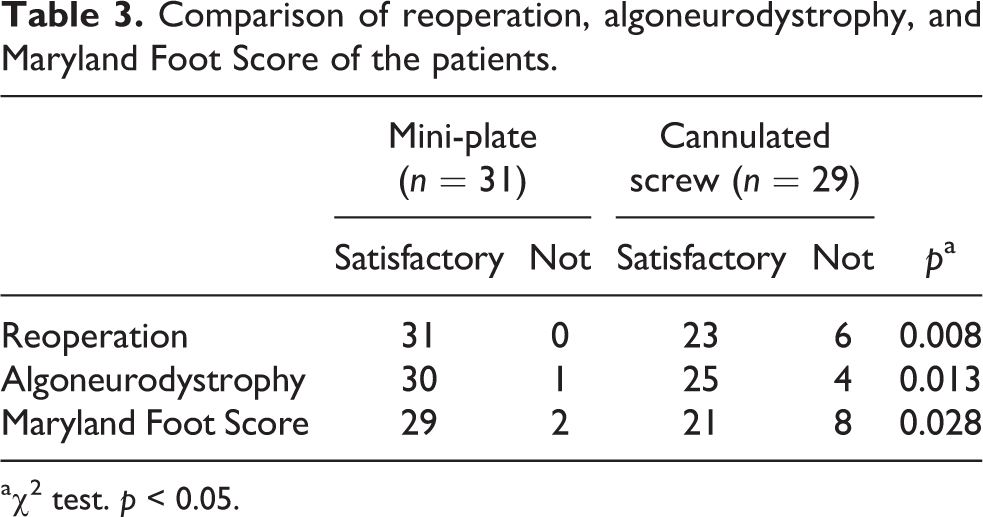
a χ 2 test. p < 0.05.
The incidence of satisfactory results of MFS in group MP was significantly higher than group CS at 1-year follow-up (n = 29, 93.5%; n = 21, 72.4%, respectively; p = 0.028).
Discussion
Most important findings of current study were better functional outcomes with lower complication rates in osteosynthesis with MP fixation compared to CS fixation in cases who underwent open reduction through sinus tarsi approach. Xia et al. in their randomized prospective study of 2014 compared 59 patients with open reduction + plate fixation by extensile L-incision to 49 patients with open reduction + percutaneous CS fixation by sinus tarsi approach, reporting better radiologic reconstruction of fracture in the former group. 14 Another randomized prospective study compared cases who underwent osteosynthesis with open reduction + plate fixation by extensile lateral incision to those who underwent percutaneous fixation with minimally invasive intervention; where no significant radiologic difference was found with superior functional outcomes and complication rates in the minimally invasive group. 15 Differing findings might be explained by the different incision and implant preferences, fracture types, and reduction techniques used in these studies.
Weber et al., comparing open reduction + percutaneous CS fixation by limited sinus tarsi approach (n = 24) to open reduction + plate fixation by extensile L-incision (n = 26), reported absence of hematoma, soft tissue complications, or nerve lesion at the expense of the need for secondary operations due to pain or implant failure in 42% of cases in the CS fixation group. 16 In another study, Stulik et al. detected no implant failure or reoperation in 38 patients with Sanders types 2 and 3 calcaneal fracture, during the period of at least 1-year follow-up after undergoing open reduction + plate screw by sinus tarsi approach. 17 Consistent with the literature, current study exhibited significantly higher reoperation rates in group CS by sinus tarsi approach than that group MP. While no implant failure or fracture, severe pain, and penetration into the joint was seen in group MP, these were observed in six cases in group CS, which might be attributed to enhanced stability and strengthened fixation offered by calcaneal plate compared to the CS.
Apart from implant failure, two patients in each group developed minor wound problem (6.6%) and one in each group had temporary sural nerve lesion (3.3%). Superficial or deep wound infection did not occur in any patient. Patients in group CS were significantly more likely to have algoneurodystrophy compared to that in group MP. Concurring with our study, minor wound site problems (0–5%), sural nerve injury (3–5%), and infections (0–8.5%) were reported in the literature. 15,18,19 All these suggest superior safety regarding complications in sinus tarsi approach compared to the conventional approach. Additionally, lower incidence of algoneurodystrophy in group MP than group CS may be related with achievement of more stable osteosynthesis and more effective rehabilitation including early weight-bearing program.
Three-dimensional reconstruction of calcaneal anatomy is very critical for foot-ankle functions and development of subtalar arthrosis. 20 A 2-mm irregularity at posterior joint surface constitutes an indication for open reduction. 21 Although minor pathologic conditions at this joint in early period did not result in much substantial alteration in functional outcomes, some studies reported serious residual injury in subtalar joint due to the irregularity at its posterior facet. 22 Restoration of the contact surface between the talus and calcaneus to its original prefracture state as much as possible should be the main objective of the surgery. Even a 2-mm incongruity at posterior facet may lead to early postoperative arthrosis in the long term, which may further require subtalar arthrodesis surgery. 23,24 Evaluation of the congruity of the joint after reduction and fixation is very difficult due to the irregular shape of posterior facet, albeit very important. In our study, both groups showed statistically significant normalization of Gissane and Böhler angles as well as calcaneal length and height compared to preoperative values. It is considered that sinus tarsi approach provided sufficient field view for anatomic reduction of all lateral structures from posterior facet to calcaneocuboid joint.
Calcaneal widening that might develop after calcaneal fracture may cause peroneal tendon impingement. 25 In order to avoid this painful condition that might even require peroneal tendon sheath relaxation, the volume of calcaneus should be able to be reconstructed close to the pre-injury status in a stabilized manner. In our study, calcaneal widening was found to be significantly better restored in MP group than that in CS group. It was reported that calcaneal widening secondary to the fracture could be further improved by the plate fixation, consistent with our findings. 18 This might be partially explained by the compressive force and better maintenance of the stabilization of the MP compared to the screw, whose clarification warrants designation of further biomechanistic comparative studies.
Calcaneal length, height, and width values were only compared pre- and postoperatively to assess the surgical affect of internal fixation methods. The normal values of these parameters may differ due to patient physical characteristics. Additionally, radiologic evaluation with CT to compare these values with contralateral side could pose patient safety. All these parameters were reconstructed postoperatively in both groups. Nevertheless, correlation between calcaneal widening and foot function was not found statistically significant.
In a study, aiming to show that early postoperative functional exercises and gradual weight-bearing reshaped subtalar joint surface and improved functional outcomes by correcting residual displacements at articular surface, patients who underwent anatomical plate and CSs were initiated exercise non-weight-bearing exercises on postoperative days 2 and 3. 26 Starting at postoperative third week with 5 kg in average for 30 min daily, weight-bearing was gradually raised to its maximum at week 12. Residual displacement at posterior joint surface was shown to be better reduced compared to the control group. 26 Consistent with this protocol, a rehabilitation program consisting of partial weight-bearing and range of motion exercises was initiated in group MP at early postoperative period in our study. Full weight-bearing was only begun after confirming radiologic fracture healing in both groups. Lower incidence of algoneurodystrophy and significantly higher 1-year MFS score in MP group might be attributed to the lower rate of implant failure or reoperation as well as to the implementation of potentially more effective rehabilitation program.
Our study has some limitations including single-center nature of the study, absence of the long-term results, relatively few number of subjects, and pooling of both male and female patients together in the study. Another weakness of the study is that we lack radiologic evidence of correction of residual displacement that is thought to occur at posterior facet regarding early weight-bearing in group MP. Although there is no radiological evidence, MFS scores suggest that early weight-bearing may have benefits in functional outcomes which may be a proof for aggressive physical theraphy.
Conclusion
MP fixation via sinus tarsi approach was shown to be associated with lower rate of implant failure and reoperations, better reconstruction of lateral calcaneal widening, and better functional outcomes in Sanders types 2 and 3 calcaneal fractures compared to CS fixation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.