
Abstract
Objective:
To examine the effect of an alternative wound closure method after tumor arthroplasty of the hip compared to routine wound closure with skin staples.
Method:
Single center, frequency matched cohort study. We reviewed all patients who underwent tumor resection and endoprosthetic reconstruction of the proximal femur for pathologic fracture due to metastatic bone disease or malignant hematologic bone disease at our center between 2010 and 2014. All patients treated with occlusive wound closure (OWC), a combination of intradermal suture, Steri-Strips™, and an occlusive skin adhesive, during this period (n = 35), were compared to an equally sized frequency matched group of patients having undergone routine wound closure with conventional skin staples.
Results:
Patients with OWC were significantly faster to achieve dry wound status and consequently had significantly shorter administration of antibiotics and hospital stay. Compared to the patients with conventional wound closure with staples, their wounds were already dry after a mean 3.4 days (vs. 6.7 days [95%CI: 3–3.8 vs. 5.5–7.9], p < 0.0001), they received antibiotics for a mean 4.2 days (vs. 6.8 days [95%CI: 3.7–4.8 vs. 5.5–8.0], p < 0.0003) and their mean hospital stay was 6.3 days (vs. 8.0 days [95%CI: 5.5–7 vs. 6.8–9.3], p < 0.015). Prolonged wound discharge (PWD) for 7 days or more was observed in 34% of patients (n = 12) in the conventional group, whereas this complication was completely absent (n = 0) in the investigational group. For every three patients treated with OWC, one complication of PWD over 7 days is avoided (number needed to treat = 3).
Conclusion:
Compared to conventional staples, OWC appears to significantly reduce wound complications, use of antibiotics, and hospital stay in patients undergoing tumor arthroplasty procedures of the hip. As such, it may also contribute to a reduction of the substantially increased risk for prosthetic joint infection in this patient population.
Keywords
Introduction
Prosthetic joint infection (PJI) remains one of the major complications of endoprosthetic reconstruction surgery and is particularly common (10–11%) 1,2 when performed in conjunction with resection of malignant bone tumors. It is a serious complication per se and typically requires further single-stage or multistage revision surgery, prolonged hospitalization, antibiotic treatment, and rehabilitation. Moreover, PJI predisposes patients with bone tumors to particular further risks and complications, such as amputation, 1 –3 and may interfere with adjuvant radio- and/or chemotherapy, which can compromise local tumor control and overall survival. The substantial cost associated with the treatment required for these complications is also well-known. 4 Prolonged wound discharge (PWD) is a well-documented predisposing risk factor for surgical site infection 5 –9 and may result in prolonged hospital stay and delay of adjuvant therapy. While reported to be a relatively uncommon complication of conventional hip arthroplasty (4%), 10 PWD appears to have a considerably higher incidence in orthopedic tumor patients (48%). 11 Our routine practice has therefore been to pre-emptively treat all our patients undergoing tumor resection and endoprosthetic reconstruction with prolonged prophylactic intravenous antibiotics until the surgical wound is completely dry. 12 In an effort to address the substantial rate of PWD in this patient population, identified in a previous study, 11 one surgeon (WH) changed his wound closure method in 2013, while three other senior surgeons initially continued their usual technique with conventional skin staples. This study was conducted to investigate the clinical effect of an alternative wound closure method on the incidence of PWD and possible secondary effects on the duration of administration of postoperative intravenous antibiotic prophylaxis and the length of the hospital stay after endoprosthetic reconstruction of the proximal femur performed in patients with a secondary or hematologic malignancy of bone.
Materials and methods
Study design and patient population
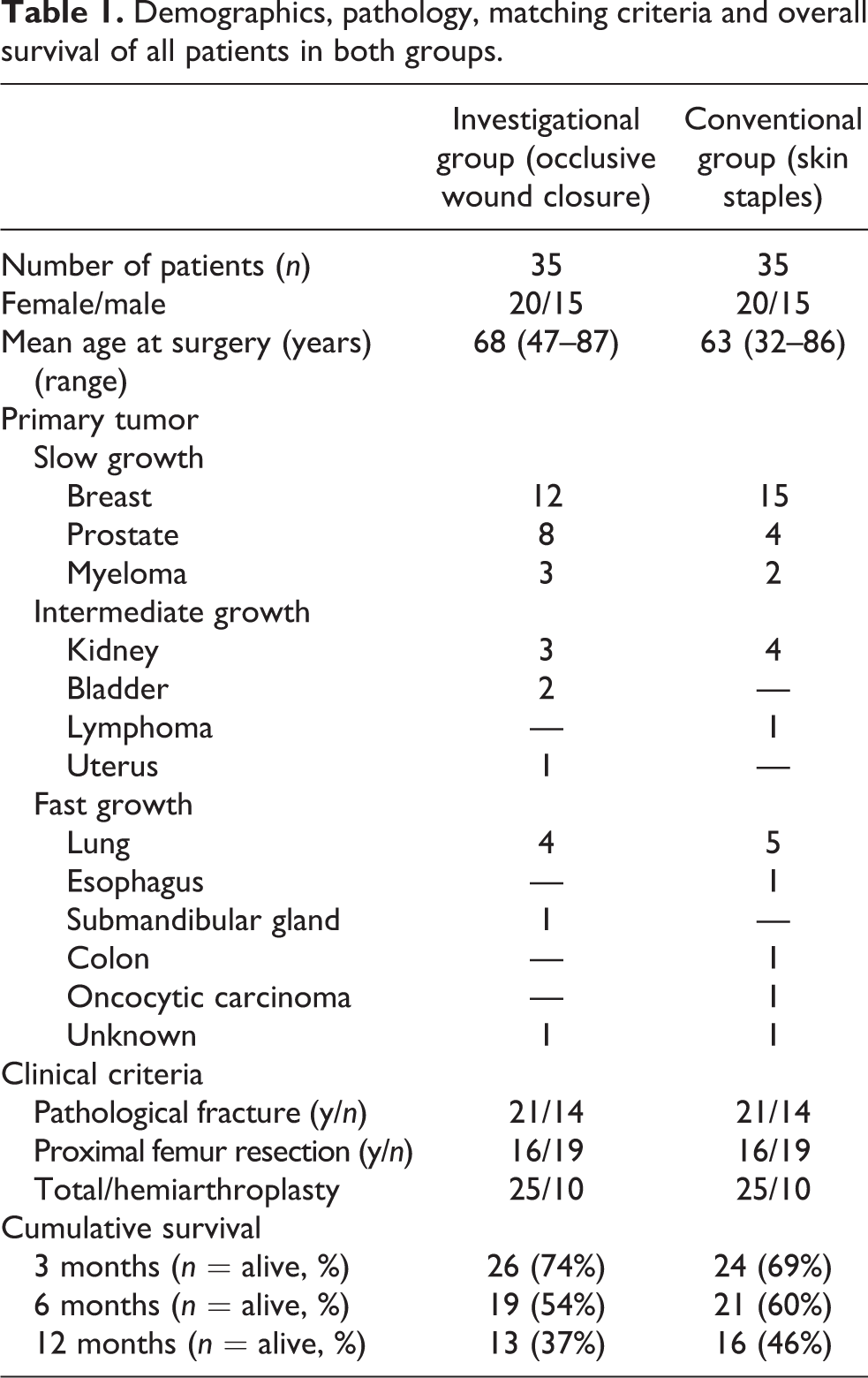
We retrospectively reviewed the medical records of all patients with metastatic bone disease and malignant hematologic bone disease who underwent endoprosthetic reconstruction of the proximal femur in our specialized orthopedic oncology unit between 2010 and 2014. All vital data (age, gender, nature and location of pathology, tumor type and growth rate, details of the surgical procedure, implants used, method of wound closure, time to dry surgical wound, duration of antibiotic treatment, and length of hospital stay) were collected from the patient files. We identified 42 patients having received occlusive wound closure (OWC) with a combination of intradermal suture, Steri-Strips™, and an occlusive skin adhesive. Six patients were excluded on the basis of either primary pathology (bone sarcoma, n = 3) or extent of the surgical procedure (pelvic reconstruction, n = 3), as we have previously identified these variables to be independent risk factors for PWD. 11 One patient was not included due to immediate postoperative death following cardiac arrest. This left us with a group of n = 35 consecutive patients treated with OWC after tumor resection for metastatic or malignant hematologic bone disease and endoprostetic reconstruction of the proximal femur in our department between December 2012 and October 2014 (investigational group). We then identified a matching group of (n = 35) patients with corresponding surgical intervention except for conventional wound closure with staples (conventional group) from the primary patient population described above, such that the distribution of the relevant demographic characteristics (age, gender, tumor growth rate, and overall survival) and matching criteria (age, gender, extent of resection, hemiarthroplasty vs. total endoprosthesis, and presence or absence of a pathological fracture) were similar, respectively identical to the distribution in the patients in the investigational group (Table 1). The indication for surgical treatment was de facto pathological fracture in 21 patients and impending pathological fracture in 14 patients in either group. Conventional femoral neck resection was performed in 19 patients as opposed to proximal femoral resection in 16 patients per group and 25 patients per group received a total joint arthroplasty with both femoral and acetabular components, whereas 10 patients in each group received a cemented hemiarthroplasty. As the extent of resection (proximal femur vs. conventional neck cut) had proven not to be a significant confoundig factor for PWD (p = 0.46) in a previous study, 11 we did not divide our relatively small study population into further subgroups. None of the patients received active chemotherapy during their hospital stay or at least 2 weeks prior to surgery. All patients with renal cell cancer metastases underwent pre-operative embolization to reduce intraoperative blood loss. Complete data without missing observations were available for postoperative survival, wound status, duration of antibiotic administration, and duration of hospital stay, in all 70 cases.
Demographics, pathology, matching criteria and overall survival of all patients in both groups.
Ethical considerations
As a purely retrospective review of patient records without involvement of any direct patient contact, this study was not considered notifiable to the ethical board. Danish Data Protection Agency approval was obtained prior to commencement of data collection (J.no: 2013-412591)
Surgical procedure
A routine posterior approach to the hip was employed in all patients. Confinement of the tumor to the femoral head or neck allowed a conventional neck resection, preservation of the abductor mechanism and endoprosthetic reconstruction with a standard (Biomet Bimetric (n = 5)) or a long (200 mm or longer) femoral stem (link: SP2 (n = 18) or MP (n = 2)) (implantcast: long stem (n = 10), RS (n = 1) or Mutars (n = 1)) or Zimmer CPT (n = 1) in 19 patients per group (n = 38)). The remaining 16 patients in each group (n = 32) required an extended posterior approach to accommodate the necessary proximal femoral resection (mean resection length 141 mm (range 120–220 mm) in group 1 versus mean resection length 140 mm (range 110–216) in group 2) and subsequent endoprosthetic reconstruction with a dedicated segmental tumor prosthesis (Zimmer Segmental (n = 30)) or a modular revision stem (Link MP (n = 2)). All femoral components were cemented, whereas treatment of the acetabular side was treated according to local condition of the joint surface and surgeon preference. The majority of patients received a cemented acetabular component (Lubinus Excentric (n = 47)), 10 patients per group had a hemiarthroplasty (Zimmer Multipolar (n = 20)) and 3 patients in the control group had an uncemented cup (Zimmer Trilogy (n = 2), Biomet Ranawat (n = 1)).
Wound closure and postoperative routine
After reattachment of residual musculature to the prosthesis using nonabsorbable suture (Nr.5 Fibrewire, Arthrex GmbH, Munich, Germany), a deep submuscular drain was inserted if considered necessary. Fascia and deep subcutaneous layers were then closed using nr1. Vicryl (Ethicon, Somerville, New Jersey, USA) interrupted sutures with particular attention to leaving minimal residual dead space and to obtain level skin edge approximation. Superficial closure followed with a neat, skin edge adapting layer of interrupted 2-0 Vicryl (Ethicon) subdermal sutures placed in inverted fashion. The skin was then either closed with a meticulous intradermal running horizontal matress suture (3-0 Vicryl RapidTM; Ethicon), tightly adjacent Steri-Strips™ (3 M Health Care, St Paul, Minnesota, USA) for fine adaptation and optimal skin approximation before final application of a flexible occlusive skin adhesive (2-octyl cyanoacrylate, Liquiband Flex; AMS Ltd, Plymouth, UK; group I, interventional group), or conventional staples (Appose ULC Slim Body Skin Stapler, Covidien, Massachusetts, USA; group II, control group) and covered with a sterile wound dressing (Mepilex Border Post-Op; Mölnicke Health Care, Göteborg, Sweden) and soft compressive bandage. Postoperatively all patients were mobilized, weight bearing as tolerated, from postoperative day 1. The sterile compressive dressing applied at conclusion of the procedure was left unchanged until day 2 or 3 to coincide with removal of any surgical drains still present. Prophylactic intravenous antibiotics (cefuroxime, 1.5 g × 3) were started 15–30 min prior to incision and not discontinued before a senior member of the surgical team considered the wound dry. Thromboprophylaxis with tinzaparin 3500–4500 IE × 1 sc. was maintained until the patients were well mobilized, at least until discharge from hospital.
Statistical analysis
Due to lack of generally accepted criteria of PWD, we calculated risk ratio (RR), risk differences, and number needed to treat for PWD of patients treated with OWC compared to that of patients undergoing routine wound closure with conventional skin staples according to a range of duration of drainage, respectively. Afterward, the data were modeled as time to events (outcomes) of interest, including completely dry wound, termination of antibiotic treatment, and hospital discharge, respectively. Kaplan–Meier survival analysis was applied to estimate the overall survival function for each of the outcomes of interest, which were then also analyzed using Cox proportional hazard models. The patients were followed up from the day of operation until the occurrence of the outcomes of interest, with follow-up time in days used as the underlying time scale. We verified that the assumptions for proportional hazards were not seriously violated using log–log plots. We performed crude analyses to estimate mean survival days with 95% confidence interval (95% CI) and hazard ratios (HRs) with 95% CI and then adjusted the HRs for potential confounders including gender, age, and tumor growth rate, which we categorized according to Katagiri 13 into slow, intermediate, or fast growth (Table 1). p-Values less than 0.05 are considered significant. All statistical analyses were performed using STATA version 14 (Stata Corp., College Station, Texas, USA).
Results
We found significant differences between investigational and control group for all outcome parameters (Table 2). The patients in our investigational group with OWC were significantly faster to achieve dry wound status. They also had significantly shorter duration of antibiotic administration and significantly shorter of hospital stay. The patients in the conventional group on the other hand, who had undergone wound closure with staples, required a mean of 3.3 more days (95% CI: 2.09–4.45, p < 0.0001) to achieve dry wound status, spent a mean of 2.5 more days (95% CI: 1.21–3.87, p < 0.0003) on intravenous antibiotics, and remained a mean of 1.8 more days (95% CI: 0.36–3.18, p < 0.0015) in hospital. As for prevention of PWD (Table 3), we found significantly lower and more rapidly decreasing experimental event rates in the investigational group at all time points, as well as a steadily decreasing RR with time. After 1 week, PWD was completely absent in the investigational group (0%) but still present in 12 patients (34%) in the conventional group. No more than three patients needed to be treated (NNT ≤ 3) to avoid one occurrence of PWD over 4 or more days. Not surprisingly, we also found evidence of very strong correlation between all outcome variables in the conventional group (r = 0.9 –1 [95% CI: 0.81–1], p < 0.0001). However, in the investigational group, the evidence of correlation was only weak to moderate (r = 0.34–0.58 [95% CI: 0.02–0.08], p < 0.0003–p < 0.048). Comparison of Kaplan–Meier survival estimates of time to event showed significant differences between investigational and conventional group for time to dry wound (p < 0.0001), time to cessation of antibiotics (p < 0.0001), and time to hospital discharge (p = 0.01) at all time points (Figures 1 to 3). Cox regression analysis, adjusted for gender, age, and tumor growth rate, revealed identical unadjusted and adjusted Cox model HR estimates of 3.7 for type of wound closure (95% CI: 2.13–6.52, p < 0.0001 vs. 95% CI: 2.10–6.60, p < 0.0001) and 2.3 for duration of antibiotic administration (95% CI: 1.37–3.93, p < 0.002 vs. 95% CI: 1.37–3.93, p < 0.005). For time to hospital discharge, the unadjusted Cox model HR estimate of 1.8 (95% CI: 1.07–2.90, p < 0.02) was slightly attenuated to 1.7 (95% CI: 1.03–2.80, p < 0.07) when adjusting for gender, age, and tumor growth rate.
Effect of wound closure method on PWD.
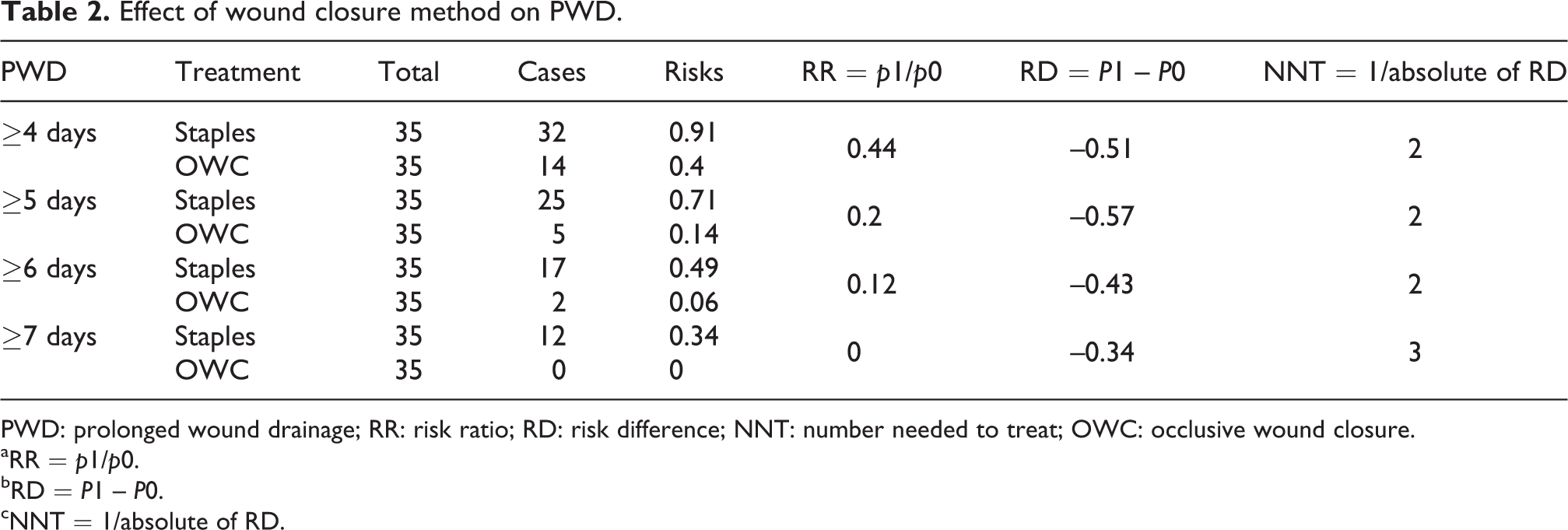
PWD: prolonged wound drainage; RR: risk ratio; RD: risk difference; NNT: number needed to treat; OWC: occlusive wound closure.
aRR = p1/p0.
bRD = P1 – P0.
cNNT = 1/absolute of RD.
Outcomes according to method of wound closure.

OWC: occlusive wound closure.

Kaplan–Meier survival function estimates for time to dry wound status.

Kaplan–Meier survival function estimates for duration of antibiotic administration.

Kaplan–Meier survival function estimates for time to discharge from hospital.
Discussion
Optimal soft tissue and wound management are essential components of any orthopedic reconstructive procedure and are critically important, particularly in joint replacement surgery, if the increased rate of wound-related complications associated with PWD is to be kept to a minimum. 14 There is clear evidence that closure of the subcutaneous tissues significantly decreases the amount of wound discharge 15 as well as the incidence of wound complications 16 ; however, the optimal skin closure method for arthroplasty procedures in particular is more controversial. Skin adhesives have some obvious advantages similar to absorbable intra-cutaneous sutures, such as avoidance of trauma associated with staples and a dedicated removal procedure. However, several randomized prospective trials have been unable to show clinically relevant differences in wound complications, length of stay, patient satisfaction, 17 –20 or cosmesis. 19,20 A recent systematic review has even found low-quality evidence suggesting that sutures may be significantly better in minimizing wound dehiscence compared to skin adhesives. 20 While almost all authors recognize that most evidence originates from studies with substantial methodological limitations, a meta-analysis comparing sutures versus staples for skin closure in orthopedic surgery could nevertheless conclude that the risk of wound infections was significantly higher with staples and recommends against their use, especially in patients undergoing hip or knee surgery. 21 There is also emerging evidence that the combination of an absorbable intra-cutaneous suture with a skin adhesive may be beneficial in patient populations that are particularly prone to postoperative wound complications and infection, such as acetabular fracture surgery. 22 This study is the first description of a skin closure method (OWC) combining three established individual techniques in a synergistic fashion, with a specific aim toward maximal stable wound edge approximation and early wound occlusion in order to reduce PWD. Our study is also the first report of the efficacy of this new skin closure method in a well-documented, high-risk patient population, where it achieved highly significant and more importantly, clinically relevant reductions of the primary and secondary outcome measures (PWD, length of antibiotic administration and length of hospital stay) in comparison to conventional closure with staples. The rates of PWD observed with conventional skin staples in our study population (34%) compare well with a previous study, 11 which identified even higher PWD rates associated with skin closure with staples (48%), as it also included patients with bone sarcoma, total femur replacement, or pelvic reconstruction for pathologic acetabular fractures, which proved to be independent risk factors for PWD. Both studies indicate that the use of conventional skin closure with skin staples may predispose to significant risk of PWD in tumor arthoplasty procedures involving the hip. Although the primary objective of this study was to determine the clinical effect of OWC on the primary outcome measure PWD, our results also showed that OWC indirectly affected both secondary outcome measures in a different fashion. While a very strong correlation of PWD with duration of administration of postoperative intravenous antibiotics is not surprising, it is a direct function of consequent application of our institutional policy not to discontinue prophylactic intravenous antibiotics before the surgical wound is completely dry; a lesser degree of correlation between PWD and length of hospital stay was likewise to be expected, since this outcome variable obviously depends on a multitude of other factors and not only the wound condition alone. However, the modest attenuation of the Cox model HR estimate, when adjusting for typical confounders such as gender, age, and tumor growth rate, also indicates that PWD still had a significant influence on hospital stay in a relevant portion of our cohort and that OWC therefore also might have a potential cost saving effect. As formal investigation of the cost effectiveness of OWC was not part of our study, it would be interesting to conduct a formal cost-benefit analysis as part of a future study. One challenge of studies like ours is to ensure perfectly balanced samples that are appropriately stratified or matched for all conceivable variables (known or unknown) that may affect the outcome of interest when the patient population is rather inhomogeneous and the sample sizes are relatively small. Based on experience and results from a previous study on incidence and potential risk factors for PWD in a similar patient population, 11 we have chosen the methodology (frequency matching) that best possibly allowed risk stratification in advance, thereby ensuring an equal distribution of the confounding factors we considered most relevant (age, gender, extent of resection, hemiarthroplasty vs. total endoprosthesis, and presence or absence of a pathological fracture). We acknowledge that there may be other risk factors with a potential impact on surgical wound healing, such as comorbidities, duration of surgery, duration of surgical wound drainage, and so on, which we did not explicitly match for, but we believe that a substantial imbalance between our study groups in that regard is not very likely. The effect of OWC even appears to be strong enough to maintain its significant advantage over conventional skin staples despite considerably decreased usage of deep surgical wound drains in our investigational cohort, which in actual fact could be regarded as an at least potential additional risk factor for PWD in itself. The strength of this skin closure method is the synergy of its components. The absorbable intra-cutaneous suture achieves primary wound edge approximation and contributes to the overall strength of the skin closure, thereby minimizing the risk of secondary wound dehiscence. The Steri-Strips™ optimize the skin approximation, relive tension at the wound edges, and aid in maintaining the skin adhesive in situ while it is still in liquid phase. Finally, the skin adhesive seals the incision, effectively occluding the wound completely once set, that is, even before application of the sterile dressing. The disadvantages of this method are that it is time-consuming and more expensive than standard wound closure techniques. The strengths of our study are the highly consistent application of the relevant surgical technique by very experienced surgeons, the excellent comparability of both patient groups due to high conformity of relevant patient demographics and matching criteria and its adequate power due to high incidence of the primary outcome and the effect size of the intervention studied. The limitations of our study are the lack of formal randomization and blinding.
Conclusion
We describe a novel skin closure method designed to minimize postoperative wound complications. Compared to conventional staples, this novel method, which we have termed OWC, appears to significantly reduce postoperative PWD, use of antibiotics, and hospital stay in patients undergoing tumor arthroplasty procedures of the hip. It is possible that the clinically relevant reduction of postoperative wound complications achieved with this wound closure method may also translate into a reduction of the substantially increased risk for PJI in this particular patient population. Longer follow-up and larger study populations will be required to confirm this hypothesis. In the meantime, this promising wound closure technique warrants further investigation in similarly challenging patient populations and more widespread use for other indications where effective reduction of postoperative wound complications is desired.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.