
Abstract
Purpose:
Sacral insufficiency fractures (SIFs) can cause severe lower back pain and immobility, which have limited therapeutic options. No previous studies have compared clinical outcomes and radiographic findings of sacroplasty with or without balloon assistance for the treatment of SIFs.
Methods:
Forty-five patients with SIFs were divided into two groups. One group had 18 patients treated using sacroplasty with balloon assistance, and the other had 27 patients treated without balloon assistance. The operation time and cement injection volume were compared between these two groups. Clinical outcomes were evaluated using visual analog scale (VAS), Oswestry Disability Index (ODI), and Odom’s criteria. Cement leakage rate was examined by postoperative radiography and computed tomography.
Results:
Sacroplasty with balloon assistance was associated with significantly longer operative time (p = 0.003) and larger cement injection volume (p = 0.038). Cement leakages were found in 4 of 18 patients (22.2%) with balloon assistance and 15 of 27 patients (55.6%) without balloon assistance, which showed significant difference (p = 0.027). No significant differences were observed between sacroplasty with and without balloon assistance with regard to clinical outcomes including improvement in VAS, ODI, and Odom’s criteria.
Conclusions:
Sacroplasty with balloon assistance was shown to achieve greater cement injection with longer operation time and can decrease the risk of cement leakage. Both sacroplasty with and without balloon assistance showed good-to-excellent clinical outcomes for the treatment of SIFs.
Introduction
Sacral insufficiency fractures (SIFs) are very painful, debilitating, often missed, and typically atraumatic sacral pathologies. 1 –5 They are associated with significant morbidity, economic impact, and prolonged hospitalization. 5 Conservative treatment consists of modified bed rest, physical therapy, percutaneous interventions, and analgesics. 6 –8 A poly(methyl methacrylate) (PMMA) bone cement injection procedure called sacroplasty has been recently described as an optional method for the treatment of SIFs. However, the correct placement of bone cement in the complex anatomical structure of the sacrum remains a surgical challenge. 9
The precise deposition of cement in the sacrum is the main challenge for surgeons in sacroplasty, particularly to avoid neural injuries by an exothermic reaction during the hardening of extraosseous cement. 10,11 Similar to percutaneous vertebroplasty for the treatment of vertebral compression fractures, cement leakage is the most common complication of sacroplasty. The kyphoplasty procedure is known to be superior to vertebroplasty for the treatment of osteoporotic vertebral compression fractures because it decreases the possibility of cement leakage. 12 The proposed mechanism of sacroplasty with balloon assistance is similar to that of balloon kyphoplasty.
The rate of cement leakage outside the SIFs could be lower in sacroplasty with balloon assistance due to the use of expandable balloons to create a presized hole and compact the fracture chips. 13 However, to our knowledge, no clinical study has compared the outcomes of sacroplasty with and without balloon assistance. The aim of this study was to compare the intraoperative findings and associated clinical outcomes of sacroplasty with and without balloon assistance for the treatment of patients with SIFs.
Materials and methods
This study was approved by the Institutional Review Board (IRB) of E-DA Hospital, I-Shou University, Taiwan, a 1200-bed tertiary referral center (IRB number: EMRP-105-040). A total of 2091 patients with severe lower back pain undergoing radiography and magnetic resonance imaging (MRI) of thoracolumbar spine examination between January 2008 and December 2015 at our university hospital were screened in this study. Sixty-seven (3.2%) patients with SIFs were noted. SIFs was diagnosed on the basis of clinical signs and symptoms and demonstrated by MRI findings. Patients with a combination of nonunion lumbar or thoracic compression fractures, neurologic deficit, the other disorders of the lumbar or hip region, infection, and tumor were excluded from our study, as these comorbidities may confuse the origin of the pathogen or influence clinical outcomes. Of the 67 patients, 45 (67.2%) patients who had poor response to conservative therapies underwent sacroplasty with or without balloon assistance by senior surgeons of our orthopedic department (Figures 1 to 6). The poor response to conservative therapies was defined as intractable pain with visual analog scale (VAS) ≥7. The detailed procedures and comparison of sacroplasty with or without balloon assistance was explained in detail to the patients and their families. The patients were divided into two groups, sacroplasty with and without balloon assistance, according to their choice of the procedure types.

An 89-year-old woman suffered from intractable back pain after a fall. Radiography showed multilevel vertebral compression fractures.

Sagittal T1- and T2-weighted magnetic resonance imaging revealed sacral insufficiency fracture with bone marrow edema.

This patient underwent sacroplasty with balloon assistance. Postoperative radiography revealed adequate distribution of poly(methyl methacrylate) bone cement.

A 75-year-old woman suffered from severe buttock pain after a slip. Radiography revealed sacrum 1 and 2 fractures.

Sagittal T1- and T2-weighted magnetic resonance imaging revealed sacral insufficiency fractures with bone marrow edema.
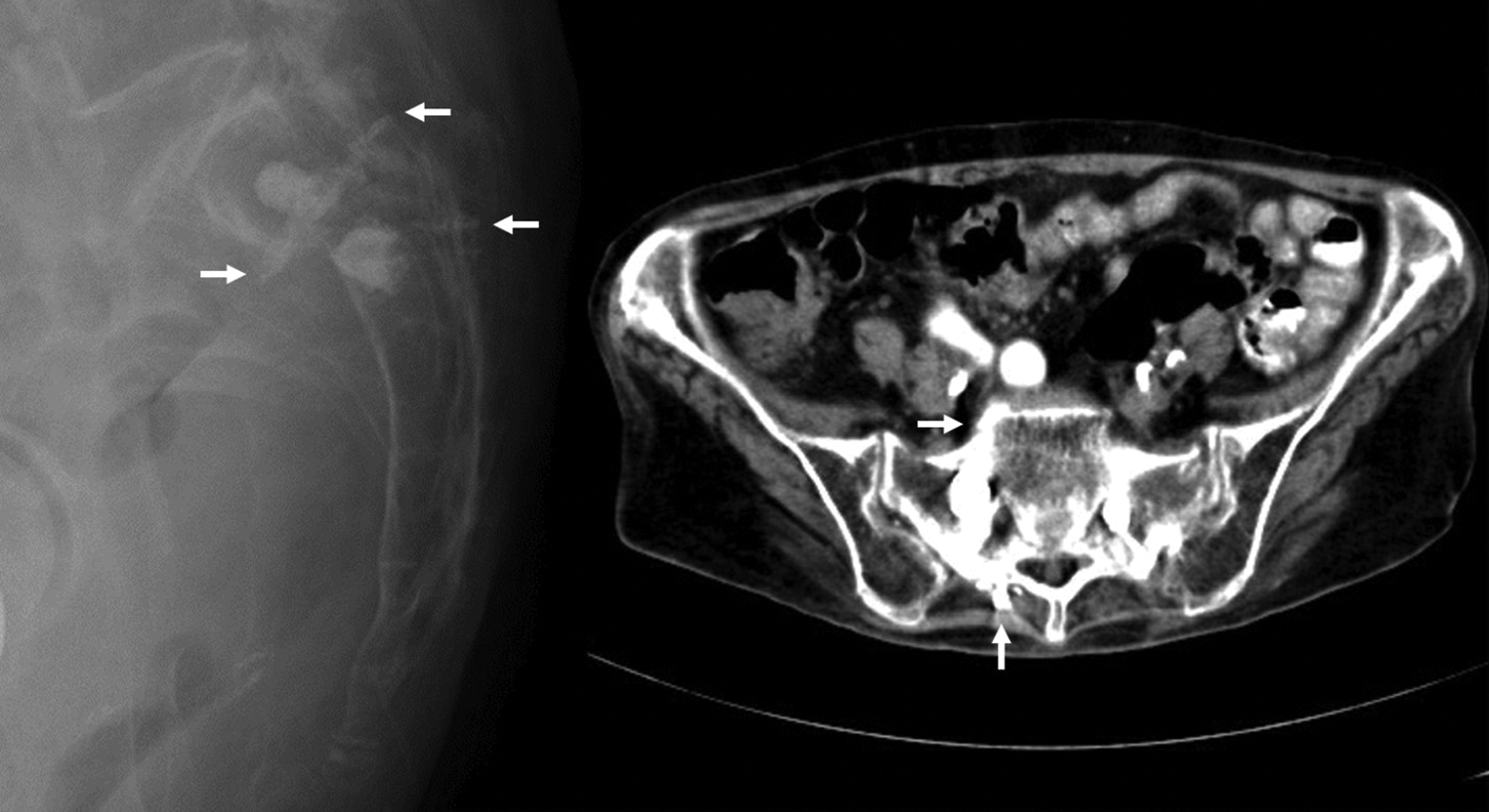
Sacroplasty without balloon assistance was used to treat this patient. Both postoperative radiography and follow-up computed tomography revealed good distribution of bone cement with asymptomatic leakage (indicated by arrows).
Surgical technique
All operations were performed after a diagnosis of SIFs with no symptom relief after conservative therapies. The patient received total intravenous anesthesia with propofol and fentanyl for spontaneous respiration during the surgery. The vital signs of the patient, including heart rhythm, blood pressure, and pulse oxygenation levels, were continually monitored by an anesthesiologist. The patient was placed in the prone position on the operating table. After careful skin sterilization and local anesthesia, an eight-gauge bone biopsy needle (Stryker Instruments, Kalamazoo, Michigan, USA) was gently inserted into the collapsed and fractured sacrum based on the results of MRI under fluoroscopic guidance. The needle tip was advanced until it reached the anterior one-third of the fractured sacral body. The sacral body was augmented with PMMA bone cement bilaterally with or without balloon assistance. In the group treated with sacroplasty with balloon assistance, a 15-mm balloon was then inserted through the trocar and inflated with 3 ml of contrast agent to create an intramedullary void. The balloon pressure was maintained below 200 psi throughout the procedure. The balloon was deflated and removed until the mixed bone cement was ready for injection.
Forty grams of bone cement (Simplex-P; Stryker Instruments) was mixed with barium sulfate (Barytgen, Fushimi, Kagawa, Japan) for delivery into the fractured sacral body. The bone cement mixture was polymerized at room temperature until it had the paste-like consistency necessary for controlled injection. The PMMA bone cement was then slowly and continually injected through a 10-ml plastic syringe inside a screw syringe compressor. The injection of the PMMA bone cement was stopped when the cement filled the posterior one-third of the sacral body or when the syringe compressor presented unusual resistance. Once the injection was completed, the needle was removed, and hemostasis was achieved at the puncture site by applying gentle pressure.
Most patients were discharged 1 or 2 days after the operation. Patients were allowed to ambulate with a walker after the operation. All patients wore a rigid orthosis for protection for at least 3 months.
Follow-up evaluations
After discharge, the patients received regular follow-up at 1, 3, 6, and 12 months and annually thereafter. Clinical outcomes and radiographic findings were evaluated, and data were collected by the senior author (S-CY), who was the operating surgeon. Clinical outcomes were evaluated by asking the patients to quantify their pain on a VAS at each follow-up appointment, with 0 indicating no pain and 10 indicating the most pain possible. The Oswestry Disability Index (ODI) and Odom’s criteria were also used to evaluate the clinical outcomes, including functional daily activities and satisfactory results at each follow-up appointment. Computed tomography (CT) scans were performed at the 1-month follow-up visit at an outpatient clinic to evaluate the possibility of bone cement extravasation outside the sacrum.
Statistical analysis
The differences between the two groups in terms of operating time, volume of cement injection, hospitalization days, postoperative Odom’s criteria, and improvement in VAS and ODI at the 1-month follow-up appointment were compared with the Mann–Whitney U-test. The rates of cement leakage in the two groups were compared with the χ 2 test. Nonparametric statistics were used because some variables did not have normally distributed data. Statistical Package for Social Science version 13.0 software (SPSS Inc., Chicago, IL, USA) was used for data analysis. A value of p < 0.05 was considered statistically significant.
Results
Patient and epidemiological profiles
After applying exclusion criteria, a total of 45 patients were enrolled in our study (4 men and 41 women). The average age was 80.2 years (range 72–89 years). Eighteen patients received sacroplasty with balloon assistance (one level at S1 in 17 patients and two levels at S1 and S2 in one patient), and 27 patients (one level at S1 in 25 patients and two levels at S1 and S2 in two patients) received sacroplasty without balloon assistance. Asymptomatic cement leakages diagnosed by postoperative CT scans were found in 19 patients, including 4 patients in the sacroplasty with balloon assistance group (22.2%) and 15 patients in the sacroplasty without balloon assistance group (55.6%). The demographic data of the enrolled patients are provided in Table 1.
Patient demographic data.

IF: insufficiency fracture; S: sacrum; n: number of patients.
Intraoperative findings
The mean operation time was 29.00 ± 1.59 min (range 25–36 min) in the sacroplasty with balloon assistance group and 18.33 ± 1.46 min (range 12–27 min) in the sacroplasty without balloon assistance group, reflecting a significant difference (p = 0.003). The mean volume of cement injection was 7.83 ± 0.6 ml (range 6–10 ml) in the sacroplasty with balloon assistance group and 5.67 ± 0.55 ml (range 4–8 ml) in the group without balloon assistance, also reflecting a significant difference (p = 0.038). The rate of cement leakage showed a significant difference between these two groups (p = 0.027). The details of the intraoperative findings are presented in Table 2. No major surgery-related complications occurred, such as spinal cord compression, pulmonary embolism, and infection.
Comparison of intraoperative findings between sacroplasty with or without balloon assistance for SIFs.

SIF: sacral insufficiency fracture; SD: standard deviation.
a Statistical analysis with Mann–Whitney U-test.
b Statistical analysis with χ 2 test.
Clinical outcomes
At the 1-month follow-up, the average VAS score decreased from 7.73 (range 7–9) preoperatively to 2.86 (range 2–4) postoperatively. Both groups demonstrated significant improvement in the VAS score; the improvement of VAS was 5.00 ± 0.52 in the sacroplasty with balloon assistance group and 4.78 ± 0.32 in the sacroplasty without balloon assistance group. No significant difference was observed in the extent of improvement in VAS score between these two groups (p = 0.902). The steady pain control of both groups in the VAS scores during 1-year follow-up is shown in Figure 7. The improvement in ODI was 49.67 ± 3.48 (range 40–50) in the sacroplasty with balloon assistance group and 48.89 ± 2.14 (range, 38–58) in the sacroplasty without balloon assistance group, also reflecting no significant difference between groups (p = 1.000). The good functional daily activities recovery of both groups in ODI during 1 year is shown in Figure 8. Odom’s criteria yielded 12 excellent and six good outcomes in the sacroplasty with balloon assistance group and 18 excellent and nine good outcomes in the sacroplasty without balloon assistance group (p = 1.000). The detailed clinical outcomes are presented in Table 3. All patients were satisfied with sacroplasty with or without balloon assistance for the treatment of buttock pain and responded that they would undergo the procedure again if indicated. Most patients in both groups were discharged 1–2 days after sacroplasty. The duration of hospitalization also showed no statistically significant difference between the two groups (p = 0.897, Table 3).

The VAS scores of both groups during 1-year follow-up. VAS: visual analog scale.

The ODI of both groups during 1-year follow-up. ODI: Oswestry Disability Index.
Comparison of clinical outcomes between sacroplasty with or without balloon assistance for SIFs.a

ODI: Oswestry Disability Index; SIF: sacral insufficiency fracture; VAS: visual analog scale.
a Odom’s criteria: P = poor, F = fair, G = good, E = excellent. VAS: 0 means no pain and 10 means the most pain possible. ODI: 0–20% = minimal disability; 21–40% = moderate disability; 41–60% = severe disability; 61–80% = crippling back pain; 81–100% = these patients are either bed-bound or have an exaggeration of their symptoms.
b Statistical analysis with Mann–Whitney U-test.
Discussion
SIFs were originally described by Lourie in 1982 and have become an increasingly important clinical entity due to both their social and economic significance as the elderly population has continued to grow. 1,14 SIFs may also result from radiation (postradiotherapy osteoporosis), osteomalacia, chronic steroid usage, renal osteodystrophy, chronic bed rest, Paget’s disease, calcium deficiency during pregnancy, and rheumatoid arthritis. 15 The major symptoms of SIFs are lower back pain with groin, buttock, and inguinal pain. These complaints are often confused with sacroiliac dysfunction, lumbar disc herniation, osteoporotic vertebral compression fracture, degenerative lumbar disorder, or facet arthropathy. Careful physical examination is necessary to exclude more common osteoporotic vertebral compression fractures of the thoracolumbar spine and degenerative disorders of the mobile spine and for differential diagnosis of the sacroiliac dysfunction. Differential diagnosis between SIFs and sacroiliac joint disorders is challenging because of their similar pain location without root sign. The diagnosis of sacroiliac dysfunction requires abnormalities on at least three of five sacroiliac tests (Gaenslen’s, compression, distraction, thigh thrust, and sacroiliac joint injection) and positive sacroiliac joint blockage with groin pain when sacral MRI is normal. The pain resulted from SIFs is mostly located in the waist, which increases with sacral palpation and decreases with rest. The physical examination of the sacroiliac joints is normal, and sacral imaging shows sacral wing fracture-related changes. 16 Furthermore, sacral MRI is still considered the gold standard for the correct diagnosis of SIFs.
The conservative treatment of SIFs includes analgesics, bed rest, and sacral orthoses. Patients who are unresponsive to this management and who have intractable pain are candidates for sacroplasty, another type of vertebroplasty. The first description of a fluoroscopy-guided sacroplasty for the treatment of painful, osteoporosis-associated SIFs was reported in 2002. 17 The sacroplasty procedure requires the injection of bone cement into the fractured area in the sacral wings. The proposed mechanism of this procedure is similar to that of vertebroplasty. In patients with SIFs, pain is due to microfractures and associated inflammatory-related mediators. The interdigitalization of the bone cement has a stabilizing effect that can reduce pain via stabilization of the microfractures. The inflammatory process is thus ameliorated.
Several studies have emphasized the pain relief and early satisfactory outcomes of patients with SIFs treated with sacroplasty. Frey et al. studied 52 patients and found that the average VAS scores were reduced from 8.1 to 0.8. 7 In a meta-analysis, Bayley et al. reviewed the results of sacroplasty in 108 patients reported in 15 published articles and found a significant reduction in VAS scores from 8.9 to 2.6 following sacroplasty. 18 Andresen et al. applied balloon sacroplasty to treat 30 patients with SIFs and suggested that the risk of cement leakage was reduced via the use of a balloon and that the observed change in VAS scores (from 8.8 to 2.7) matched well with those observed in other studies. 19 In the current study, both sacroplasty with and without balloon assistance were associated with a significant reduction in VAS and ODI and good-to-excellent outcomes using Odom’s criteria, which all are similar to most published studies.
Radiological presentation is one of the most important aspects for evaluating the results of vertebral augmentation techniques. Restoration of vertebral body height and associated sagittal alignment should be addressed in thoracolumbar osteoporotic compression fractures. However, vertebral height restoration is not the aim of sacroplasty for SIFs. A good radiological outcome involves adequate cement distribution and avoidance of bone cement leakage, especially into the sacroiliac joint. Theoretically, sacroplasty using balloon catheters and intraoperative fluoroscopic assistance can achieve a controlled and reliable cement introduction. Therefore, bone cement leakage and neurological complications can be mostly prevented. The compaction of the fractured and destroyed bone and subsequent filling with bone cement to increase the stability of the fractured sacrum appears to be the most important mechanism for prompt reduction of pain. 20 In the lumbar or thoracic region, a recent systematic review and meta-analysis demonstrated that balloon kyphoplasty was associated with lower odds of new fractures, less extraosseous cement leakage, and greater reduction in kyphotic angle. However, no significant difference was found between vertebroplasty and balloon kyphoplasty in either short-term or long-term pain and disability outcomes in patients with osteoporotic vertebral compression fracture. 21 The results of the present study also demonstrated that sacroplasty with balloon assistance resulted in a lower rate of extraosseous cement leakage, but similar improvements in pain and clinical outcomes compared to sacroplasty without balloon assistance.
Cement leakage is one of the most common complications of sacroplasty. In a cadaveric study in 2009 that compared sacroplasty with and without balloon assistance, Grossterlinden et al. reported that sacroplasty with balloon assistance is a feasible technique for correct cement placement in the sacrum after creating a void, although no difference in the leakage rate was reported. 9 In a clinical study, Onen et al. reported that the rate of cement leakage ranged from 8% to 31% in sacroplasty with balloon assistance, which is lower than in sacroplasty without balloon assistance (16.6–73%). 16 Recently, Eichler et al. 22 and Andresen et al. 23 introduced the use of radiofrequency to activate bone cement insertion and reduce cement leakage and suggested that this method was safer for sacroplasty. In the present study, cement leakage was observed in 22.2% (4 of 18) of the sacroplasty with balloon assistance group and in 55.6% (15 of 27) of the sacroplasty without balloon assistance group. Cement leakage outside the vertebral body during vertebroplasty is common and is usually clinically asymptomatic. The most serious complication is cement leakage into the spinal canal and compression of the neural elements that could result in neurological injury necessitating urgent surgical intervention. Because the end of the cauda equina exists rather wide and tolerable spinal canal in sacral area, all enrolled patients with posterior cement leakage during sacroplasty in the current study were asymptomatic and could be treated conservatively.
We observed a higher rate of cement leakage in the group without balloon assistance compared to the group with balloon assistance, which also showed statistically significant difference in this rather small patient population (p = 0.027). Additionally, much more cement was introduced into the SIFs in the sacroplasty with balloon assistance group compared to the sacroplasty without balloon assistance group (p = 0.038). In theory, better interdigitation and stability can be achieved with a larger volume of bone cement. However, there was no significant difference in the clinical outcomes of VAS and ODI scores between the groups. There was also no significant difference in patient satisfaction based on Odom’s criteria. In the literature, no experimental or clinical studies are available proving how much bone cement is required for SIFs. Liebschner et al. used finite element analysis to demonstrate that only a small amount of bone cement (14% fill or 3.5 ml) was necessary to restore the stiffness of the damaged thoracolumbar vertebral body to its predamage value. 24 Belkoff et al. performed a biomechanical study on osteoporotic cadaveric vertebral bodies and found that only 2 ml bone cement was required to restore the strength of compressed vertebral bodies. 25 They also found that restoration of vertebral stiffness required varying amounts of bone cement, depending on the location of the vertebral body. Therefore, even if we did not completely fill the vacuum cleft or adequately distribute the SIFs, the patients still experienced some degree of pain relief because of partial augmentation of the vacuum or SIFs.
This study has several limitations. First, the sample size in the current study was not large enough for the authors to perform meaningful multivariate analyses to identify predictor variables accurately. These results are promising, but a larger cohort study is necessary to confirm our findings. Second, the retrospective nature of this study lacked a random assignment of subjects and did not allow for the enrolled patients to undergo different treatment methods, including either conservative trigger point injection with steroid or more invasive open surgery, for subsequent comparisons of clinical outcomes. Third, we did not design a placebo group for comparison in the current study. The feasibility and benefits of sacroplasty with and without balloon assistance for the treatment of SIFs need to be rigorously evaluated in a large patient population with prospectively controlled comparison groups.
Conclusion
Sacroplasty with balloon assistance was associated with a longer operation time but also shown to introduce more cement volume than sacroplasty without balloon assistance. A lower cement leakage rate was also found in the sacroplasty with balloon assistance group. However, both sacroplasty with and without balloon assistance could achieve good-to-excellent clinical outcomes for patients with SIFs.
Footnotes
Authors’ contribution
S-CY and T-TT have contributed equally to the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.