
Abstract
Introduction:
Open reduction and internal fixation using plates is the gold standard for the treatment of displaced forearm bone fractures in adults. The ulna being subcutaneous throughout has a constant approach. However, the radius is approached from either the dorsal or the volar side. Both the dorsal and the volar approaches to the radial shaft involve meticulous dissection and preservation of important neurovascular structures. The posterior interosseus nerve is at risk in the dorsal approach and the radial artery and its branches in the volar approach. Dissection of these structures also adds to the operative time. The possibility of a third alternate approach was perceived, which could decrease the potential risks of the conventional approaches.
Patients and Methods:
Sixteen patients with radial shaft fractures in the middle third were operated on using the lateral approach: 6 of them had isolated radius fracture and 10 had both-bone fractures. There were 13 males and three females with a mean age of 37.9 years. Limited contact dynamic compression plate or locking compression plate of 3.5 mm was used to fix all fractures. All patients were operated on within 36 h of injury and then followed up till union. Union was assessed using serial radiographs and functional outcome using Anderson et al.’s criteria. The final functional outcome was assessed at an average 6 months after surgery and the results compiled.
Results:
The mean operative time in isolated radius fractures was 37.5 min and that for plating of both bones was 80.7 min. Primary bone grafting of the radius was done in one case and secondary bone grafting in another patient with delayed union of the radius. Union was achieved in all cases at a mean time of 17.25 weeks. The functional outcome was excellent in 10 patients, satisfactory in 5 patients, and unsatisfactory in 1 patient.
Conclusion:
The lateral approach is a simple approach with low operative complexity and complications. We found this approach to provide a reliably good exposure of the middle third of the radius, enabling lateral plating without complications.
Introduction
Forearm diaphyseal fractures in adults account for about 1% of all fractures. 1,2 In the presence of significant deforming muscle forces, it is very difficult to maintain acceptable alignment in these fractures by nonoperative methods. 3,4 Open reduction and internal fixation with plates is generally accepted as the best method of treatment for displaced diaphyseal fractures of the forearm in adults. 5,6 Traditionally, plating of the radial shaft is carried out using one of the two approaches: the volar (Henry) and the dorsal (Thompson). The ulna being subcutaneous is approached by a direct incision over it. For the radius, the dorsal or Thompson approach is generally used for fractures of the upper two-thirds. 7 The volar or Henry approach is an extensile approach that gives access to the entire length of the radius and is nowadays considered the preferred approach. 8,9 Although both these approaches have stood the test of time, they require a good level of expertise and a meticulous surgical technique to carry out the procedures safely. Both are known to be associated with operative difficulties and potential complications. The posterior interosseus nerve (PIN) is endangered in the posterior approach proximally. Although the nerve runs through the supinator muscle and can be protected by reflecting it from the bone along with the supinator, in 25% of cases, the PIN runs juxtaperiosteally and is still liable to injury. 10,11 Identification and protection of the nerve adds to the surgical time and operative complexity. Also in both-bone fractures, the dorsal incision for the radius is at times too close to the ulnar incision endangering the intervening skin bridge and making wound closure difficult. 12,13 In the volar approach, the radial artery is encountered all along and can be injured if sufficient time and effort are not devoted to protect it. 14 The PIN can also be injured in the proximal part of this approach. All these complications are more likely if the surgeon is less experienced.
To help avoid the potential neurovascular complications of the dorsal and the volar approaches and to add another tool to the armamentarium of the upper limb trauma surgeon, we devised an alternate, simpler approach for the middle third of the radial shaft. This “lateral” approach to the mid-radius is also quick and provides a safe skin bridge between the radial and ulnar incisions in case of both-bone fractures.
Patients and methods
After approval from the Institutional Ethics Committee, between September 2014 and March 2016, 16 patients were operated on using this approach: 13 were men and 3 women with a mean age of 37.9 years (18–62 years). Ten patients had fractures of both the forearm bones and 6 had fracture of the radius only. Two of the patients with isolated radius fracture and one with both-bone fractures had distal radioulnar joint disruption (Galeazzi fracture dislocation). There were 15 closed fractures and 1 grade 2 open fracture. Patients below 18 years of age, open grade 3 fractures, fractures with preoperative neurovascular deficits, compartment syndrome, and other major ipsilateral upper limb injuries were excluded from the study. The mode of trauma was as follows: motor vehicle accident, 7; fall on the hand, 7; assault, 1; and torsional injury due to loss of control over heavy drilling equipment, 1. All the radial shaft fractures were in the middle third of the bone. All patients were operated on within 36 h of injury. The radius was approached first in all cases, using the described technique, while the ulna was accessed using the standard incision over its subcutaneous border.
Surgical technique for the radius
After anesthesia, and application of the arm tourniquet, the limb is positioned on the side table with the patient supine. Painting and draping is done in the standard fashion. Prophylactic antibiotics are administered, and the tourniquet is then inflated. The forearm is next placed in 90° of flexion and mid-prone. The incision is made over the straight line joining the tip of the radial styloid distally and the lateral epicondyle of the humerus proximally, centering it over the fracture (Figure 1). After superficial dissection, the deep fascia is incised along the line of the incision. The interval is then developed between the brachioradialis (BR) on the volar and the extensor carpi radialis longus (ECRL) on the dorsal side; the fracture can now be clearly visualized (Figure 2). We do not routinely try to identify the superficial radial nerve apart from the BR, unless it is seen crossing the surgical field, in which case it is isolated and secured (Figure 3). Dissection around the fracture is kept extraperiosteal as much as possible. The fracture is manipulated into reduction, and the lateral surface of the radius is prepared for plate placement. The pronator teres is attached to the lateral and dorsal surface of the proximal fragment in most cases, and it is cleared off the lateral surface by passing a hemostat beneath and sharply dissecting it off the bone. The dorsal attachment is kept intact, thus creating a tunnel under which the plate can be slid (Figure 4). If exposure necessitates, the pronator teres insertion can be divided altogether, as done in the classic Henry approach. A template is then placed over the lateral surface at the fracture site to assess the normal lateral bow of the radius. Accordingly, a 3.5-mm limited contact dynamic compression plate (LC-DCP) or locking compression plate is contoured for application onto the lateral surface. Definitive fixation is completed using three bicortical screws on both sides of the fracture (Figure 5). The distal radioulnar joint (DRUJ) is assessed in Galeazzi-type injuries and addressed accordingly. Removal of the retractors causes the ECRL and BR to fall back on and covers the radius and the implant. The wound is approximated with two or three temporary skin sutures so as to facilitate good placement of the ulnar incision. The ulna is fixed in the routine manner, and final closure is done after both bones have been fixed. A suction drain may be used.

Midprone position and incision; the brachioradialis on the volar side and the ECRL dorsal are visualized. ECRL: extensor carpi radialis longus.

The interval is developed the fracture exposed; the pronator teres is found attached to the proximal fragment in this case.

Sometimes the superficial radial nerve is encountered and secured.

A tunnel is created beneath the pronator teres for the plate.

Fracture is reduced; the required plate is contoured and applied to the lateral surface of the radius.
Postoperatively, a long-arm plaster splint was used in patients with DRUJ disruption for 6 weeks. In patients without DRUJ injury, no postoperative immobilization was used, and active hand, wrist, and elbow exercises were encouraged from the first postoperative day. Antibiotics were given for 3 days, and only one dressing change was done on the third day. All patients were examined for signs of nerve injury and wound complications before being discharged. Stitches were removed at 2 weeks in the clinic. Activity was gradually increased depending on patient comfort, and the patients were followed up clinicoradiologically at 4-week intervals for the first 3 months and at 6-week intervals thereafter till union. Final follow-up was done at an average 6 months following surgery, and scoring was done at this time (Figures 6 –9).

Radial shaft fracture approached and plated laterally.

Union and outcome in the patient in Figure 6.

Fracture of both forearm bones with DRUJ disruption. DRUJ: distal radioulnar joint.
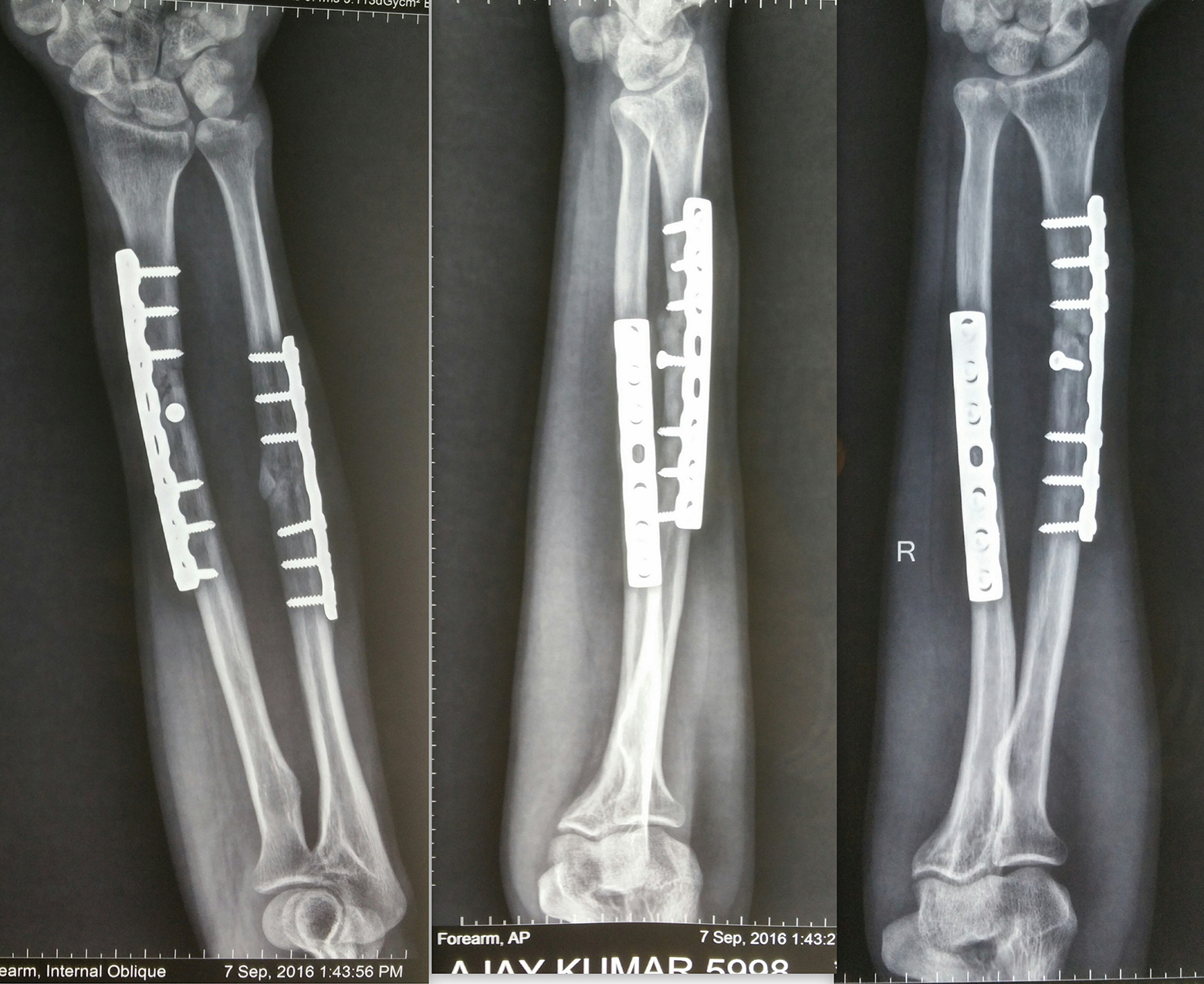
Radiographs of the patient at union. This patient had an unsatisfactory outcome with severe restriction of rotations.
Union was assessed by gradual disappearance of the fracture line and/or development of bridging callus at the fracture site. Functional outcome was determined using Anderson et al.’s criteria 15 (Table 1).
Anderson et al.’s criteria for the assessment of functional outcome.

Results
All fractures were fixed within 36 h of injury. The mean surgical time in isolated radius fractures was 37.5 min (30–45), whereas in both-bone fractures it was 80.7 min (70–95 min). Primary bone grafting of the radius was done in one case with considerable fracture comminution, while one case of delayed union of the radius required late bone grafting at 18 weeks. All fractures united at a mean time of 17.25 weeks (10–28 weeks). According to the Anderson et al.’s criteria, 10 patients had excellent results, 5 had satisfactory results, and 1 had unsatisfactory result; there were no failures. There were no nerve or vessel injuries, infections, or wound healing problems in our series (Table 2).
Patient profiles and outcome.
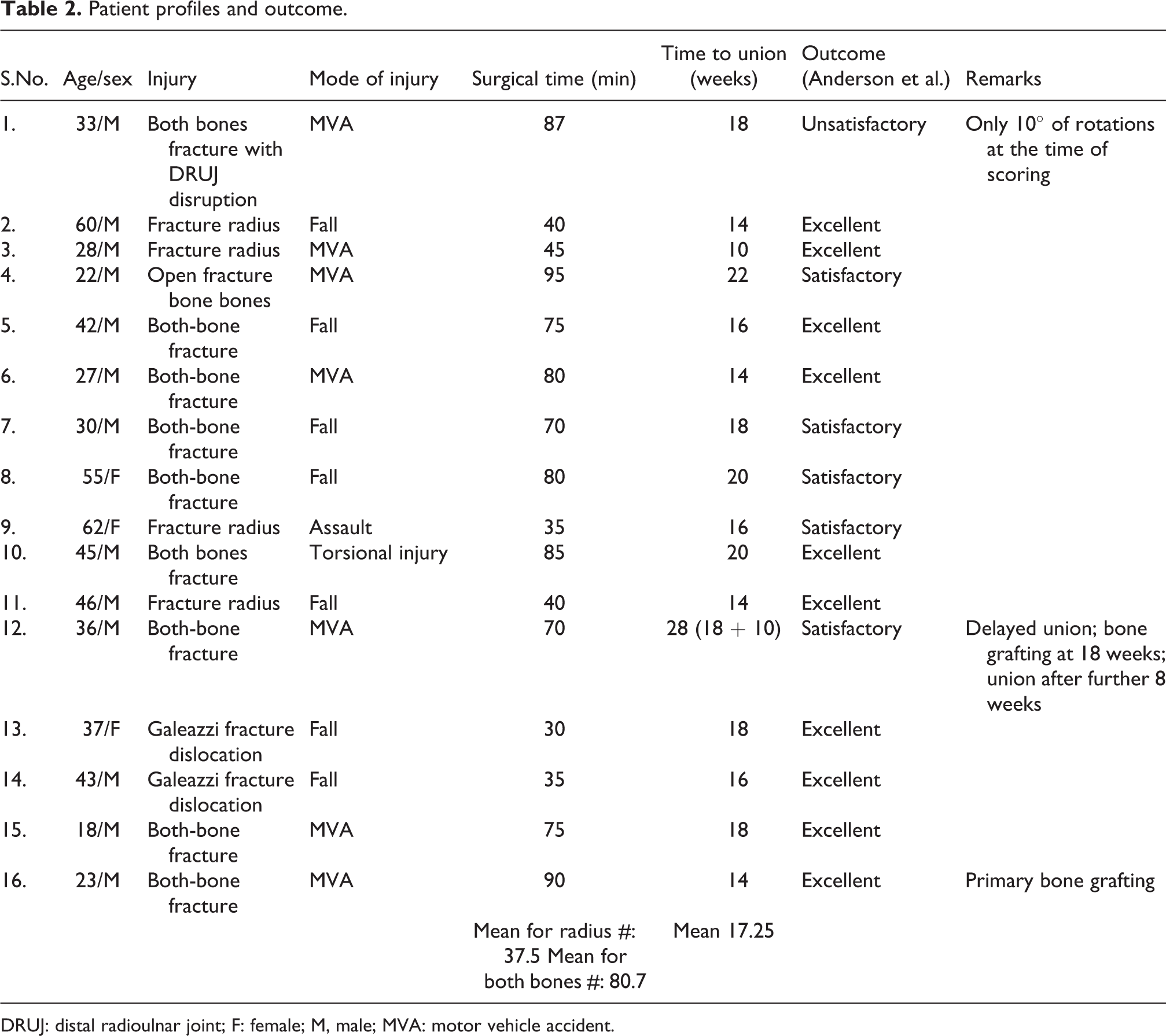
DRUJ: distal radioulnar joint; F: female; M, male; MVA: motor vehicle accident.
Discussion
Fracture of the forearm bones in adults is a relatively common injury, and open reduction and plate fixation is the standard of care for such patients. 5,6,16 The approach for the ulna is uniform; however, traditionally, the radial shaft is approached using either a volar (Henry) or a dorsal (Thompson) approach. Barring the distal third of the radial shaft which uniformly approached from the volar side, the choice of approach for the rest of the radius is mostly surgeon specific. 17 Both approaches have their advantages. Proponents of the volar approach argue that it helps avoid iatrogenic injury to the PIN, besides being extensile and giving access to the entire radial shaft. Dorsal platers on the contrary cite risk to the radial artery, recurrent radial artery and PIN, and irritation of the biceps tendon proximally in volar plating. 18,19 Further, we feel that identifying and securing these vital structures may prolong the operative time, especially with the limb under tourniquet.
The lateral approach that we devised was an attempt to address some of the difficulties in these two conventional approaches and to provide the orthopedic surgeon with a third option while making the plan to operate. The middle third of the radius was chosen because of it being relatively less covered. After superficial dissection, the interval between the ECRL and BR is readily identified, and access to the fracture is easily achieved. However, this interval can be extended distally and, with effort, proximally as well. Proximally the supinator is encountered and is dealt with in the same way as in the Thompson approach. Plating is done on the tensile lateral surface.
There was no case of vascular injury or postoperative hematoma in our series. Postoperative hematoma formation is a well-known complication associated with the volar approach and results mostly from injury to the recurrent radial artery. 14 We did not encounter any nerve injuries in our patients. Mehdi Nasab et al. reported PIN palsies in 5 of the 70 plated radii (three volar and two dorsal). 19,20 Saikia et al. reported one transient radial nerve palsy in 18 radii fixed with LC-DCP. 21
The lateral approach also provides good separation between the two incisions for fixing the radius and ulna, especially when compared with the Thompson approach. This decreases the incidence of difficult wound closure and avoids possible wound complications. 13
At the same time, union rates and functional outcomes using the lateral approach and plating the lateral surface of the radius are comparable to those reported in the literature with conventional techniques. We achieved union in 100% of our subjects (including one delayed union) with a mean time to union of 17.25 weeks. These figures are in keeping with those reported by Leung and Chow (union rate, 100%; mean time to union, 17 weeks with LCDCP), Stevens and Ten Duis (union rate, 100%; mean time to union, 22 weeks with DCP), Anderson et al. (union rate in radius, 97.8% using DCP), and Hertel et al. (98.5% union rate including two delayed unions). 6,15,22,23
If plate removal is done using the conventional approaches, the same structures are at a greater risk than in primary surgery because of scarring. Mekhail et al. warned against plate removal from the radius through the posterior approach because of the high risk to the PIN. Reusing the lateral approach for implant removal again is safer in this regard. 18,24
Our study is not without limitations though. We have a small sample size and that too from a single center. Although we have used this approach for proximal third fractures in two patients, they were not included in the present series to keep the data uniform and to increase our own expertise in the proximal area before drawing meaningful conclusions. Further, it was observed that in a few patients the plate was palpable in the distal part; however, no patient complained about it. We think that ours is an early report of this novel approach, and more studies with additional study dimensions need to be done to further validate its applicability and its place in modern forearm surgery. As of now, we have added another tool to the armamentarium of the upper limb surgeon whose utility will become clearer over time.
Thus, at this stage, we can conclude that the lateral approach is a reasonably safe and reliable route to the radial shaft and should be considered as the third alternative to Thompson and Henry approaches when operating on fractures of the middle third.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.