
Abstract
Introduction:
The purpose of this study was to compare acetabular cup positioning using an imageless navigation-assisted total hip arthroplasty (THA) to a case-matched control group using the conventional technique in Asian physique.
Methods:
Case matching controlled study using retrospectively collected data for THAs was done. Matching criteria were gender, age ± 5 years, and body mass index ± 5 kg/m2. Thirty patients who had navigation THAs were manually matched to a conventional group of 30 patients. After measuring anteversion and inclination on 3-D CT, final cup anteversion was calculated using the mathematical formula (anteversion = arctan [tan (anatomic anteversion) × sin (inclination)]).
Results:
No significant difference was observed between mean inclination (p = 0.420), anteversion (p = 0.697), and the mean deviation from 15° for anteversion (p = 0.649). However, there was a statistical significant difference for mean deviation from 40° for inclination (p = 0.027). There was a significant difference in the percentage of correctly placed acetabular cup in safe zones with inclination (p = 0.039).
Conclusions:
Although soft tissue overlying the pubic tubercle interfered with registration of the bony landmark and thereby induced inaccuracy of anteversion angles in the navigation group, the use of imageless navigation-assisted technique increases the placement within the safe zone for inclination and enhances the accuracy and the precision of inclination of the acetabular cup relative to the conventional THA rather than anteversion. This finding may be due to the effect of the patient’s physique on the anterior pelvic plane (APP)-based reference system of imageless navigation.
Introduction
Incorrect positioning of acetabular cup performing THA is still a problem leading to dislocation, 1,2 component impingement, 3,4 leg length discrepancy, 5 increased wear of bearing surfaces, 6 and a higher revision rate.
In the conventional technique, intraoperative methods of determining acetabular cup position have consisted of freehand techniques and the use of mechanical guides. This approach has used many anatomical landmarks, such as the transverse acetabular ligament (TAL), 7 acetabular notch, 8 and anterosuperior iliac spine (ASIS), 9 to guide the position of the acetabular cup into the safe zone. However, freehand techniques rely on the surgeon’s ability to estimate cup orientation and are affected by the patient’s position on the operating table. 3,10 Therefore, many studies reported postoperative acetabular cup placement outside the safe zone, 11 from 42% to 78%, even when THA was performed by experienced surgeons. 3,10,12 These problems demonstrate a need for a more accurate method to minimize malpositioning and to enhance the consistency of the acetabular cup placement in THA.
Navigation-assisted THA can provide more accurate position of the acetabular cup. A number of studies have evaluated the anteversion and inclination of the acetabular cup after THA using conventional techniques and using a navigation system. 13 –15 However, the debate continues over whether navigation systems provide a more reliable method of ensuring accurate placement of acetabular component than conventional techniques in Western countries. 13,16 However, a few comparisons have been made of navigation-assisted THA and conventional THA in Asian physique.
Accuracy is how close a measured value is to the actual value. Precision is how close the measured values are to each other. The evaluation of accuracy and precision of the navigation-assisted THA are essential to its clinical usefulness. The purpose of this pair-matched retrospective study was to compare navigation-assisted THA with the conventional THA with respect to postoperative cup positioning and to elucidate whether anteversion or inclination is more affected by navigation-assisted cup positioning in Asian physique.
Materials and methods
This pair-matched cohort study used retrospective data from THAs performed. Patients who had proper postoperative computed tomography (CT) of the hip and whose follow-up period was more than 3 years were included. Patients who underwent a THA revision or bilateral THA or patients whose postoperative CT were missing were excluded. Seventy-two patients were offered navigation-assisted THA, and 68 patients underwent THAs performed using conventional techniques. Sixty-six patients (66 of 72) underwent navigation-assisted THA and 38 patients (38 of 68) underwent conventional THA who met the inclusion criteria (Figure 1).

The flow chart shows the selection of matched pairs, the total number of THAs performed during the study period, and the excluded cases.
The matching criteria were gender, age ± 5 years, and body mass index (BMI) ± 5 kg/m2: the matching process was performed in that order. As a result, 30 patients who had navigation-assisted THA (navigation group) were manually pair-matched to 30 patients who had conventional THA (conventional group).
For the navigation-assisted THA, we used the OrthoPilot v 2.0, 2.1, image-free navigation system (B. BRAUN Aesculap, Tuttlingen, Germany). With the patient in the supine position, a tracking device was firmly fixed using the aseptic technique to the iliac crest approximately two finger-widths proximal to the ASIS on the ipsilateral side. A blunt metal probe equipped with optical sensing spheres was then used to superficially reference the bilateral ASIS and symphysis pubis. By referencing these landmarks, the orientation and position of the pelvis were determined and the anterior pelvic plane (APP), the referencing plane for navigation, was created. The patient was placed in the lateral position for THA. All THAs were performed in the lateral position using the posterolateral approach, regardless of whether the THA was navigation-assisted. The navigation system determined the center of the hip rotation and assisted with implantation of the acetabular cup. In conventional THA, the acetabular cup position was assessed using an alignment guide, which could be attached to the reamer handle and anatomical landmarks (TAL, acetabular wall, and sciatic notch). Cup orientation was targeted to 40° of inclination and 15° of anteversion in both groups.
The radiographic cup positioning of the navigation-assisted THAs was compared with that of the pair-matched control group who had undergone conventional THAs. The positioning was based on postoperative CT, which was obtained within two postoperative weeks (GE Healthcare, Milwaukee, Wisconsin, USA).
Three different anteversion determinations of the acetabular cup, anatomic, operative, and radiologic, were measured based on CT images. 17 After measuring the three types of anteversion, final cup inclination and anteversion angles were calculated using these mathematical formulas suggested by Murray 18 :


Calculated inclination and anteversion angles were compared with the “safe zone” described by Lewinnek et al. (inclination of 40 ± 10° and anteversion 15 ± 10°). 11 In addition, we computed the accuracy as the mean deviation from the target angle (anteversion = 15°, inclination = 40°), and the precision was defined as the 95% limit on the deviation between the calculated angles and the target angles in each group.
To assess the clinical outcome, we calculated the Harris Hip score preoperatively and at 1 year postoperatively. All measurements were performed twice by one orthopedic surgeon (S.T.Y) who did not know the study group of the patients, and the means of measured values were analyzed.
Statistical analysis was performed using SPSS version 17.0 software (SPSS Inc., Chicago, Illinois, USA). Independent t-tests were used to compare the two study groups for demographic data, mean cup anteversion and inclination, and mean deviation from target values. Pearson’s χ 2 test was used to compare both groups, regarding the number of hips in the safe zone. Fisher’s exact test was used to compare both groups regarding the number of patients in stratified anteversion and inclination.
Results
Demographic data
No significant differences were observed in demographic characteristics between the two groups except follow-up duration (Table 1). There were 21 (70%) male and 9 female (30%) patients in each group. The mean age of the navigation group was 62.2 years (range 34–86 years) and 62.1 years (range 36–83 years) in the conventional group. The mean BMI was 23.1 ± 2.8 kg/m2 in the navigation group and 24.2 ± 2.3 kg/m2 in the conventional group.
Demographic characteristics of both study groups.

BMI: body mass index.
a Values are represented as mean ± standard deviation.
Operation time
The mean operative time for navigation-assisted THA was 168.0 ± 38.1 min (range 94–225 min) and 165.3 ± 31.1 min (range 119–250 min) in the conventional THA (Table 2). There was no significant difference in operative time.
Comparison of cup angles, placement, and operative times between the two groups.

a Values are represented as mean ± standard deviation.
Radiologic results
Table 2 compares the overall radiologic results by study group. In the navigation group, the mean anteversion angle was 20.6 ± 7.45°, and the mean inclination angle was 43.1 ± 7.26°. In the conventional group, the mean anteversion angle was 21.3 ± 5.95°, and the mean inclination angle was 45.2 ± 11.67° (Figure 2). The navigation and conventional groups did not differ significantly in mean anteversion and inclination angles (anteversion: p = 0.697; inclination: p = 0.420). In the navigation group, 20 (66.7%) patients were placed within the safe zone for anteversion, 11 and 23 (76.7%) patients in the conventional group (p = 0.390) were placed within the safe anteversion zone. However, the inclination criteria of Lewinnek et al. for the safe zone were met by 26 (86.7%) patients in the navigation group and 18 (60%) patients in the conventional group (p = 0.020). The frequency of placement within the safe zone for both anteversion and inclination did not differ significantly between the two groups (Figure 3).

The mean cup anteversion and inclination angles for each study group are displayed.
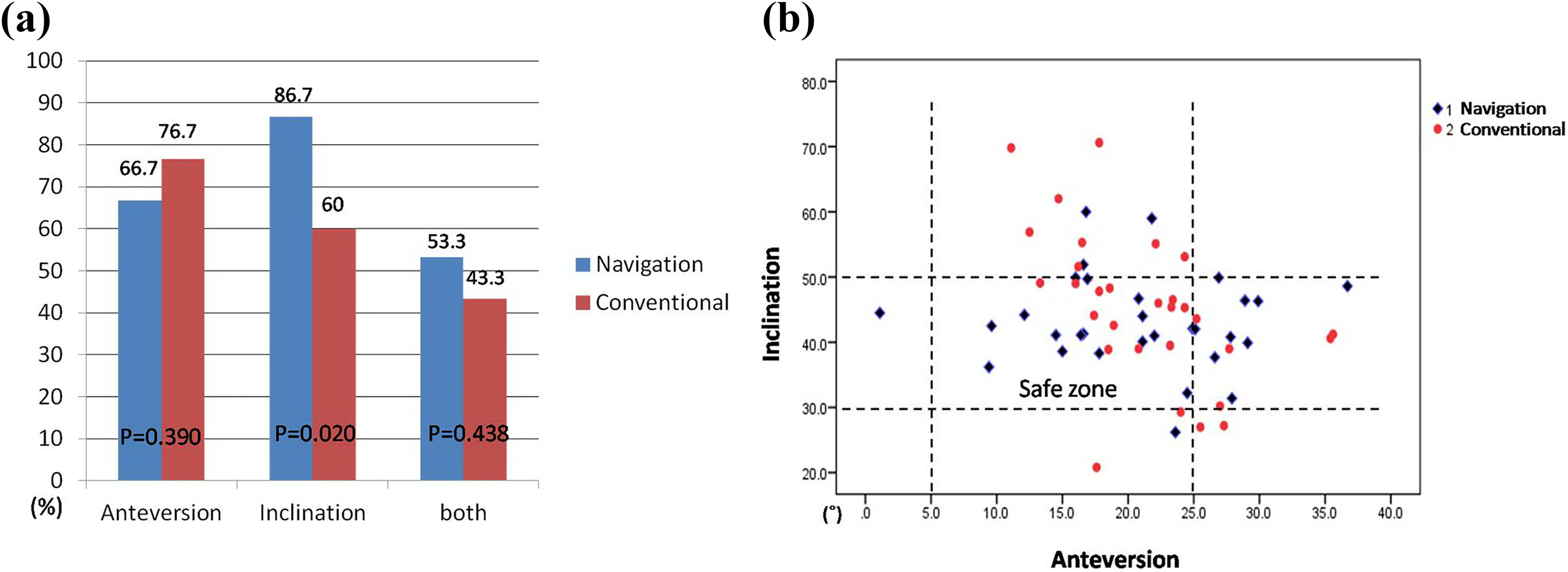
The frequency of placement within the safe zone. (a) Bar graph shows the percentages of the navigation and conventional groups in the safe zone. (b) Scatterplot of postoperative anteversion and inclination angles of the navigation and conventional groups are displayed relative to the safe zone.
The mean deviations from the anteversion target angle (15°) were similar: 7.47 ± 5.47° in the navigation group and 6.84 ± 5.26° in the conventional group (p = 0.649). However, the mean deviation from the inclination target angle (40°) differed significantly between the navigation and conventional groups: 5.76 ± 5.33° and 9.77 ± 8.06°, respectively (p = 0.027) (Figure 4).

The mean deviation from the target angles (anteversion = 15° and inclination = 40°) for anteversion and inclination for both study groups is displayed.
The precision of the anteversion angle was 4.09° in the navigation group and 3.93° in the conventional group; the precision of the inclination angle was 3.98° and 6.02°, respectively, in the navigation group and in the conventional group.
A separate analysis was performed using data from patients with values within the safe zone, based on both anteversion and inclination criteria. This separate analysis found that the mean deviations from the target anteversion angle were 4.21 ± 3.13° in the navigation group and 5.09 ± 2.90° in the conventional group (p = 0.443). The mean deviation from the target inclination angle also did not differ significantly between the two groups (navigation group: 3.65 ± 3.20° and conventional group: 5.13 ± 3.07°, p = 0.216). The precision values for the anteversion angle were 3.31° in the navigation group and 3.50° in the conventional group; for the inclination angle, they were 3.41° and 3.71°, respectively, in the navigation group and in the conventional group.
The distribution of the inclination angles among categories of the inclination angle (each category had a range of 5°) was examined. The placement of the acetabular cup of the conventional group appeared more diverse than that of the navigation group; however, this difference was not significant (p = 0.5786) (Figure 5(a) and (b)).
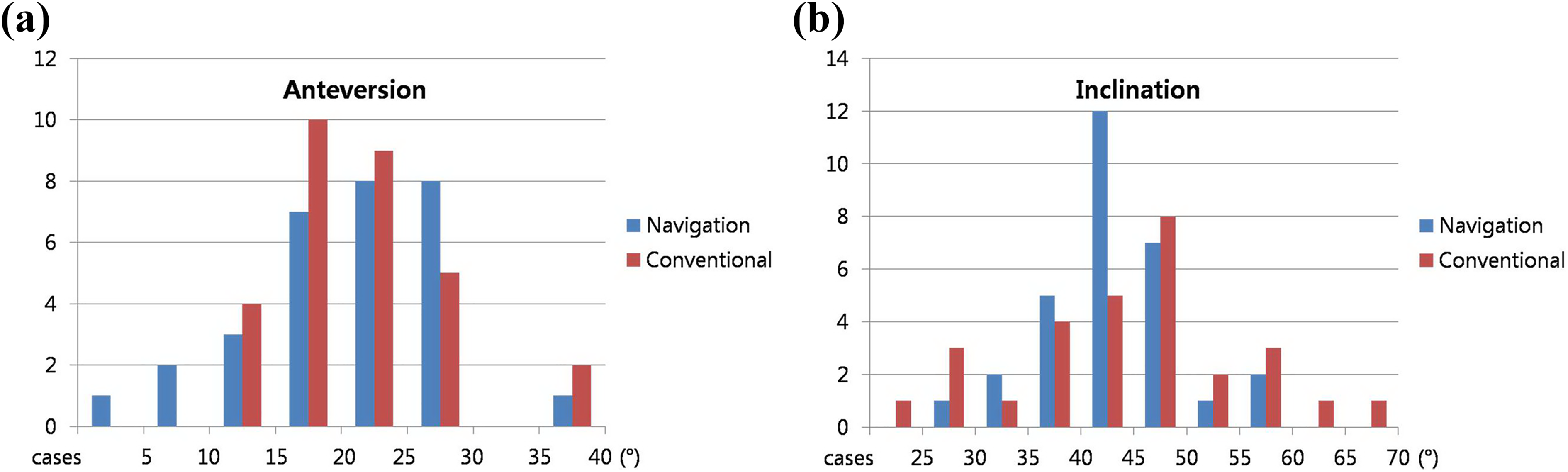
Comparison of the study groups according to the distribution of patients among categories of the anteversion (a) and inclination (b) angles; each category includes a range of 5°.
Clinical results
In both groups, the postoperative Harris Hip score improved significantly compared with the preoperative score, and no significant differences were found between the study groups at 3 years postoperatively. Regarding complications, we encountered one dislocation in the navigation group and two dislocations in the conventional group, which were treated with conservative treatment using manual reduction and brace.
Discussion
The positioning of the acetabular cup during THA, especially using conventional techniques, is dependent on the position of the patient’s pelvis on the operative table during cup insertion. 19 The patient’s position is not always maintained correctly during surgery. This may lead to pelvic malalignment and misjudgment in estimating pelvic orientation. 4,9 In addition, anatomical landmarks can be difficult to distinguish in patients with a deformed or dysplastic hip. Another possible cause of cup malpositioning is pelvic motion during impaction of the cup into the acetabulum. 4
Navigation systems have been introduced as a tool to achieve ideal implant position in THA. The THA navigation system registers the bony landmarks to calculate the APP, which is used as the reference plane. The approach of using the APP was introduced to computer-assisted cup placement in 1988 by Jaramaz et al. 20 Today, almost all navigation-assisted THAs rely on the definition of the APP. Wolf et al. 21 reported a substantial error in the estimation of anteversion and inclination if bony landmarks that define the APP were not correctly located. Therefore, registration of bony landmarks (the ASIS and symphysis pubis) is a critical step to achieving correct cup position and must be as accurate as possible. However, when registration is performed superficially, the overlying soft tissue can interfere with locating bony landmarks correctly and potentially introduce tilting of the reference plane. Parratte and Argenson 22 reported that the thickness of the soft tissue over the bony landmarks can affect the anteversion and inclination of the acetabular cup in navigation-assisted THA, and they observed an increase in acetabular cup position measurement error in patients with a BMI ≥ 27 kg/m2. In addition, in navigation-assisted THA, pelvic geometry characteristics, such as tilting, rotation, and obliquity, affect the calculation of the APP and can lead to inaccuracies of acetabular cup placement. 23,24
Many studies reported the radiologic results of cup placement with the use of navigation-assisted THA (Table 3). 14,16,17,25 –27 Lin et al. 17 reported a significant decrease in the mean deviation from the desired position in anteversion and inclination using navigation-assisted THA. Pagkalos et al. 26 demonstrated no significant improvement in accuracy using navigation-assisted THA compared to conventional positioning.
Comparative studies between imageless navigation-assisted and conventional THA in recent 5 years.

SD: standard deviation; Navi.: navigation THA; Con.: conventional THA; RCT: randomized controlled trial; NS: nonsignificant; BMI: body mass index.
a Mean deviation from the desired position.
In this study, we hypothesized that navigation-assisted THA could provide a more accurate and precise cup placement compared to the conventional method. However, in our study, the use of computer navigation enhanced the accuracy and precision of inclination but not anteversion. Postoperative CT of the navigation group revealed less deviation from the target inclination angle and more frequent inclination angles in the safe zone. However, the mean anteversion and inclination angles were not significantly different between the two groups. These findings differed from the studies intended for Western population as described in Table 3.
Ybinger et al. 24 reported that inclination inaccuracy correlated with the thickness of the soft tissue overlying the ASIS, whereas imprecision in anteversion correlated with the thickness of the soft tissue overlying the pubic tubercle. In our study, most of the patients in the navigation group were not obese (mean BMI = 23.1 ± 2.8 kg/m2). Therefore, it was relatively easier to locate the ASIS than the pubic tubercle. These procedures for bony landmark registration could explain our results; in our study, the use of the navigation system enhanced the accuracy and precision of only cup inclination. However, the soft tissue overlying the pubic tubercle interfered with the registration of the bony landmark and thereby induced inaccuracy of anteversion angles in the navigation group.
We registered the anatomical landmarks using a blunt metal probe superficially; perhaps this method is another explanation for our lower rate of placement within the safe zone for anteversion. One of the previous reports demonstrated that it was possible to achieve a high accuracy by penetrating the skin and the subcutaneous tissue to register bony landmarks. 27
This study was conducted in an Asian population. Because differences may exist in pelvic parameters among different populations, pelvic geometry differences may influence the acetabular cup placement. However, we did not consider these potential differences between the races, and we focused only on BMI. In spite of this limitation, the current study was conducted using CT and mathematical equations for measuring the postoperative anteversion and inclination. In this way, we could obtain accurate and reliable outcome data.
Bajek et al. reported that a navigation system does not substitute for surgical skill and experience, because it merely transmits information to the surgeon. 28 The decisions are in the hands of the surgeon during the entire procedure. However, navigation provides real-time information of the acetabular cup position to the surgeon and serves as an additional tool to achieve correct cup position.
Increasing surgical volumes for replacement surgery in both community setting and a single-surgeon setting has shown to reduce the complication rates and revision rates significantly, which have been correlated as better functional outcome. 29 However, all our surgeons had limited exposure to navigation prior to study, thus providing a reliable evaluation of educational effect of navigation. We had a low-to-intermediate case load of approximately 50–70 cases per year in our center, and this also makes our study relevant to the majority of arthroplasty surgeons across the world who work mostly in a low-to-intermediate volume center.
Conclusion
Based on the results of this study, there were no significant differences in the mean anteversion and inclination angles between the groups. However, navigation-assisted THA increases the probability of placement within the safe zone for inclination and enhances the accuracy and the precision of inclination of the acetabular cup relative to conventional THA, while that of anteversion was not affected by navigation. This finding may be due to the effect of the patient’s physique on the APP-based reference system of imageless navigation. To achieve a better cup position, more reliable methods of acquiring the APP or using other anatomical registration techniques, which are not less affected by patients’ physique, are needed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.