
Abstract
Purpose:
Rockwood classified acromioclavicular (AC) joint injuries by displacement of the joint on radiographs. This classification has driven the management dogma of acute AC dislocation. The correlation between Rockwood grade and symptoms has not been described in acute injury. This study assesses that relationship.
Methods:
This series included 77 patients with acute AC joint injury (<6 weeks), treated between 2006 and 2015. Objective and patient-reported measures enabled correlation between clinical measures and Rockwood grade.
Results:
The mean age was 32 years (±11.86; range 17–59 years); 88% were male. Forty-four per cent were professional athletes and 43% suffered injury during rugby. The mean time from injury to presentation was 2 weeks (±1.64; range 0–5 weeks). There was poor correlation between Rockwood classification and pain (visual analogue scale) (r s = 0.05; p = 0.752). Poor correlation was noted between Rockwood grade and functional deficit (elevation (r s = 0.18; p = 0.275), abduction (r s = 0.19; p = 0.246) and strength (r s = 0.09; p = 0.579) vs. contralateral side). Oxford and Constant scores did not correlate with Rockwood grade (r s = 0.13; p = 0.972 and 0.01; p = 0.448, respectively).
Conclusion:
The Rockwood grade does not correlate with clinical symptoms in acute AC joint injury. Previous evidence demonstrates the Rockwood classification’s limitations in predicting the structures injured. Therefore, the reliability of using the Rockwood grade as a decision-making tool in the management of acute AC joint dislocation is unclear.
Introduction
Acromioclavicular (AC) joint dislocations account for nearly 10% of all shoulder injuries that seek medical attention. 1 The AC joint is particularly at risk in athletes, and it accounts for 40–50% of shoulder injuries in this population. 2 The mechanism of injury is usually a result of either a fall or a collision, 3 and as a result, AC injuries occur more frequently in younger male athletes, especially in collision sports such as rugby. 4
AC joint injury describes a spectrum of severity, from a mild sprain to rupture of all stabilizing structures. Low-grade injuries are estimated to be twice as common as high-grade injuries. 5
Plain radiographs are the standard imaging investigation after injury to the AC joint, as based on the original descriptions by Tossy et al., 6 Allman 7 and Rockwood et al. 8 The Zanca view removes superimposition of scapula spine to unmask the AC joint pathology. An axillary lateral may provide some indication of posterior displacement. The degree of vertical displacement on radiographs is proposed to correlate with the sequence of structural injuries. The normal coracoclavicular distance is 1.1–1.3 cm. 8 AC joint injuries were classified into three types by Tossy and Allman 6,7 : Rockwood expanded this in 1989 to include types IV, V and VI (Table 1). 8
Rockwood classification with reference to injury of structures and AC joint displacement ratio. 7

AC: acromioclavicular.
The Rockwood classification is the standard instrument used to categorize these injuries and guides many surgeons in their surgical decision-making. 9
Low-grade sprains (grades I and II) are usually managed nonoperatively. 10 They are not, however, entirely benign, 11 and a minority will suffer ongoing pain. High-grade injuries (Rockwood IV and V) are usually managed operatively. The management of grade III injuries remains controversial. Some studies report improved outcomes with surgery, but nonoperative treatment has been supported by many studies, including a recent meta-analysis. 12
An obvious limitation of Rockwood’s classification is that it takes into account neither patient symptoms nor functional demands. The degree of pain and functional impairment experienced by patients varies and may not be closely related to the degree of displacement.
The aim of this study is to determine whether a relationship exists between the Rockwood grade and patients’ acute symptoms and functional deficit. While it is plausible to believe that the degree of symptoms and functional incapacitation are greater in higher grades of AC joint dislocation, we hypothesized that there is no such association.
Materials and methods
A retrospective evaluation of a single centre’s series of patients with acute AC joint injuries was performed. Patient data were entered into an electronic database at presentation. All patients signed a consent form authorizing collection of such data at their initial consultation. This database was searched to identify all acute injuries to the AC joint from February 2006 to February 2015. We defined ‘acute’ as presenting at less than 6 weeks after injury. Electronic medical records and imaging were reviewed. No patient was contacted as part of this study.
Demographic variables included age, gender, sport and level of competition. Injury data included mechanism of injury, time from injury to presentation and side of injury. Clinical examination findings included range of motion, strength and posterior displacement. New patients completed a shoulder assessment questionnaire on presentation to record patient-reported outcome scores including Constant Shoulder Score (CS), 13 Oxford Shoulder Score (OSS) 14 and visual analogue scale (VAS) (0–15) for pain. The 0–15 scale was used so that, for the Constant score’s pain component, a categorical scale could be applied (no pain = 15, mild = 10, moderate = 5 and severe = 0).
Radiographic data
Plain anteroposterior (AP) Zanca and axial radiographs of the AC joint were analysed. Clavicle translation was measured as the ratio of the AC joint height. These methods have been described for measuring the AC joint displacement. 15,16 Therefore, the AC joint ratio (R; equation (1)) was calculated to enable Rockwood grading.
Statistical analysis
Descriptive statistics was calculated for all variables of interest. Spearman’s correlation analysis was used to determine the association between the clinical measures (CS, OSS and VAS) and the Rockwood grade. The recommendations of Burnand et al. 17 were used to classify correlations, using Spearman’s rho (r s) <0.30 as a negligible correlation; 0.30 ≤ r s < 0.45 as moderate correlation; 0.45 ≤ r s < 0.60 as substantial correlation; and r s ≥ 0.60 as high correlation. All analyses were performed using SPSS (version 20.0; IBM, Manchester, UK).
Results
Seventy-seven patients presented within 6 weeks from injury to their AC joint. The mean cohort age was 32 years (±11.86; range 17–59 years), of whom 88% were male. Seventeen patients had low-grade sprains (grades 1 and 2); 35 patients had grade 3 dislocation; 13 had grade IV instability; and 12 had grade 5 dislocation.
Professional athletes accounted for 44% of the patient cohort. Forty-three per cent of the patient cohort suffered injury while playing rugby. The mean time from injury to presentation was 2 weeks (±1.64; range 0–5 weeks).
Pain
There was poor correlation between Rockwood grade and pre-intervention VAS pain score (r s = 0.05; p = 0.752) (Figure 1).

Pre-intervention pain (VAS) by Rockwood grade. VAS: visual analogue scale.
Functional deficit
The pre-intervention movement deficit observed in patients’ injured shoulders showed poor correlation with injury grade: deficit in forward elevation (r s = 0.18; p = 0.275) and abduction (r s = 0.19; p = 0.246). Similarly, the deficit in strength compared to the contralateral side showed negligible correlation with the Rockwood grade (r s = 0.09; p = 0.579).
PROM scores
Pre-intervention Oxford and Constant scores showed negligible correlation with Rockwood’s classification (r s = 0.13; p = 0.972 and 0.01; p = 0.448, respectively) (Figure 2).
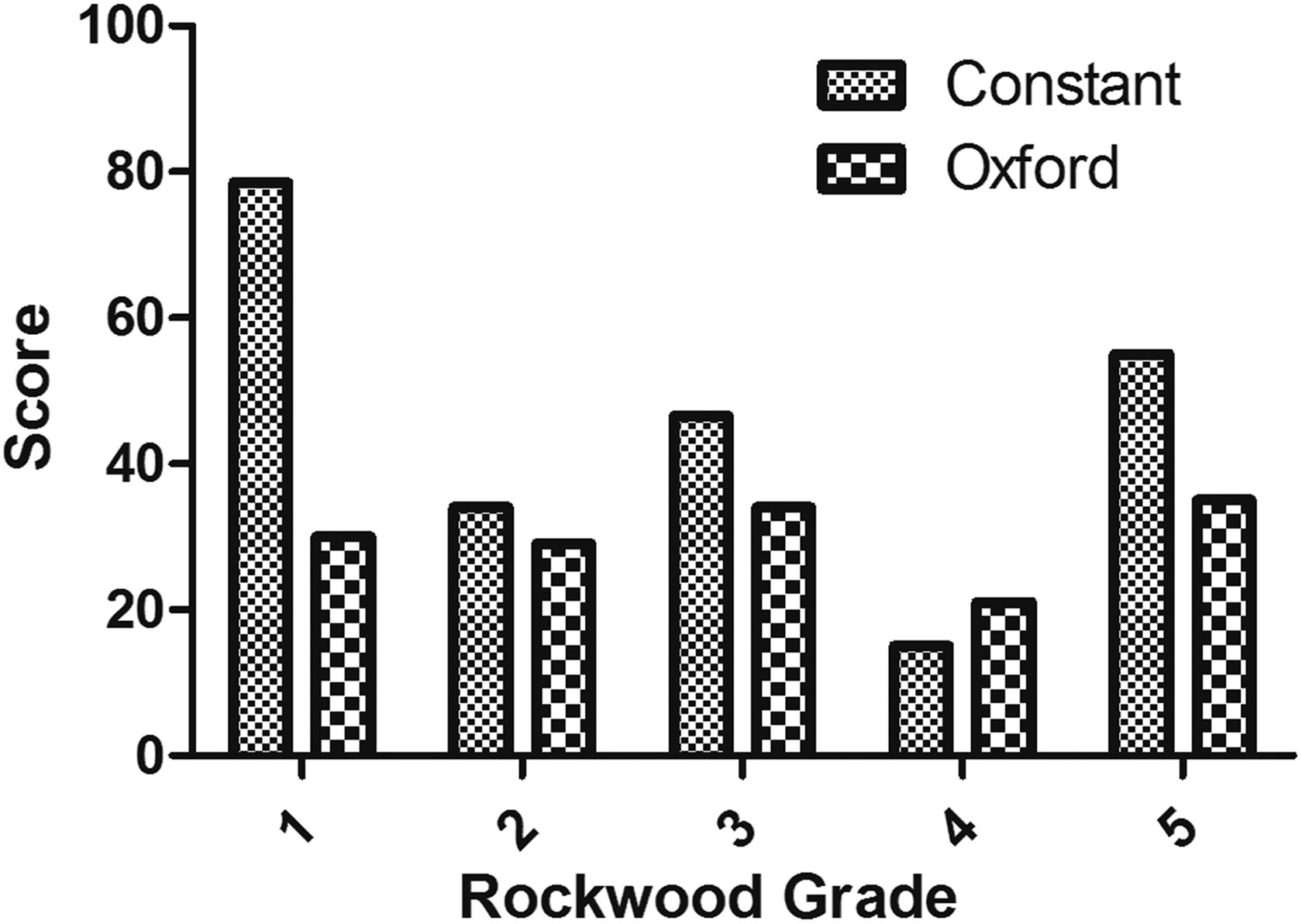
Pre-intervention Constant and Oxford Shoulder Scores by Rockwood grade.
There was a marked relationship between time to presentation and Constant score. This was due to the improved range of motion components noted in those presenting longer after their injury (Table 2). However, this change in function over time was not significantly different between injury grade subgroups: strength, p = 0.0955; pain, p = 0.9922; abduction, p = 0.125; and forward elevation, p = 0.198.
Correlation between time from injury to presentation and Constant score, Oxford Shoulder Score and VAS pain score.

VAS: visual analogue scale.
Gender and athletic level
The Rockwood grade neither showed relationship with patient gender (r s = 0.06; p = 0.630) nor did being a professional athlete influence the findings (r s = 0.11; p = 0.342).
Discussion
This cohort comprised 77 active patients, of whom 44% were professional athletes and 43% were injured during rugby. The young, predominantly male cohort reflects a typical patient demographic of AC joint injury: the young, male, contact athlete. 4
The most important finding is that there was negligible association between the pre-intervention clinical and functional scores and the degree of AC joint displacement in acute injury. The literature is lacking in exploring the link between displacement and acute symptoms, but studies have demonstrated no correlation between post-surgical displacement and clinical outcomes. 18
Others have identified the limitations of the Rockwood classification in terms of reliability. Ng et al. demonstrated only moderate-to-poor inter- and intra-rater reliability of the classification on the AP Zanca radiograph. 19 The axillary radiograph, which is used to identify patients with posterior displacement, is also subject to limitations. Although sensitive, the specificity of the axillary view is so poor that a ‘positive test’ is more likely to be ‘false positive’ than the true pathology. 20 Cross-sectional imaging may improve the application of a radiological diagnosis. Cho et al. explored the reliability of plain films and the impact of additional 3D CT scanning. 5 There was only moderate-to-fair reliability on radiographs, and the addition of 3D CT did not improve agreement. Magnetic resonance imaging (MRI) has the advantage of identifying rupture of the coracoclavicular ligaments following AC joint injury. 21 Nemec et al. compared radiographs with MRI in patients with acute AC joint injury. MRI examination changed the injury ‘grade’ in nearly half of cases, with over a third being downgraded. 22
The cohort comprises a high proportion (44%) of professional athletes. Muccioli et al. reported poorer outcomes in professional sportspeople versus non-professional athletes after surgical reconstruction for chronic symptomatic instability. 15 The reason for their reported difference remains unclear. Although our cohort included only patients with acute injury, this study has not shown such a difference. It is therefore unlikely that our professional athletes have skewed the findings of our study.
The present study had several limitations. In line with most studies examining the AC joint injury, this study is a retrospective case series. Another potential limitation is the varying times from injury to presentation. When assessing acute symptoms after any injury, time to presentation is likely to have an effect. In our study, the Constant scores did change with time to presentation. This is due to the improved range of motion, but pain scores and Oxford scores did not alter. Furthermore, there was no significant difference in this improvement in function (strength, flexion and abduction) between injury grade subgroups. Therefore, the main study finding– that Rockwood grade and acute pain and symptoms do not correlate–can remain valid. We have already noted the published limitations of using plain radiographs to assess AC joint displacement. Zanca views may vary in their projection angle, and this might influence the perceived displacement. This is important and, as mentioned above, represents a limitation of the Rockwood classification when using real-world radiographs. We present pre-intervention data and not the final outcome or eventual treatment. Despite this, we believe that the poor correlation between acute functional deficit and symptoms is important, as this is the time when a surgeon would need to decide upon either early surgery or a conservative-first approach.
In terms of the strengths of this study, we have employed validated patient-reported shoulder questionnaire assessments soon after injury and before intervention to establish symptom burden, strength and range of motion deficit compared to the uninjured shoulder. This combination provides a robust assessment of the impact of AC joint injury in the acute period. No AC joint-specific PROM is observed. It is of course possible that a PROM that specifically focuses on AC joint injuries and their impact on sport, occupation and activities of daily living might demonstrate a difference between Rockwood grades in acute injury where the OSS, CS and VAS cannot.
Conclusions
Our primary objective was to examine the association between the radiographic Rockwood grade and patients’ acute symptoms. We have demonstrated that no such association exists.
If an injury classification system is to be helpful, alongside providing a common language, it should also provide reliable injury severity grading, prognostication, and decision-making support. Nemec et al. have shown that the Rockwood classification, applied to radiographs, is unable to identify reliably the structures injured. 22 The present study has shown that symptoms do not correlate with injury grade in the acute phase. Unlike other retrospective series where outcomes post-intervention are presented, this study focused on pre-intervention symptoms, as this is the point at which a surgeon would need to choose between early surgery and a conservative-first treatment plan.
While it may be appropriate, the consensus for early surgery in Rockwood grades IV–VI is based on scant comparative clinical data. The controversy regarding the best management of grade III injuries continues to confound surgeons. Given these limitations and this study’s findings that acute symptoms do not correlate with injury grade, it seems unreasonable to advocate reliance upon the radiographic Rockwood grade as a decision-making instrument for surgical selection in patients with acute AC joint injury. A small pilot comparative study that prospectively explores conservatively treated versus operatively treated high-grade injuries might validate the practice of early surgery in such patients. If, however, the surgery-first approach were shown not to be of benefit, or remained in doubt, then a larger study would be justified both ethically and in the interests of future patients.
Despite the limitations of Rockwood’s classification, the potential usefulness of radiological evaluation should not be forgotten. Further study to formulate an improved classification system is warranted: one that considers symptoms, functional impairment and the patient’s functional demands as well as exploiting modern imaging modalities such as MRI.
Until such data or classification systems become available, we are reassured that our selection algorithm for patients with acute AC joint injury remains appropriate: We offer early surgery to those patients with unstable AC joint injuries whose pain and dysfunction 2–3 weeks after injury lead to an inability to perform work, sport and daily activities. If patients are coping well, regardless of their injury grade, then we would allow them to continue rehabilitation without early surgery.
Footnotes
Author contributions
All authors have contributed to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.