
Abstract
Purpose:
To evaluate the volume of bone cyst using the planimetry method of the Cavalieri principle.
Methods:
A retrospective analysis was carried out on data from 25 computed tomography (CT) images of patients with bone cyst. The volume of the cysts was calculated by two independent observers using the planimetry method. The procedures were repeated 1 month later by each observer.
Results:
The overall mean volume of the bone cyst was 29.25 ± 25.86 cm3. The mean bone cyst volumes calculated by the first observer for the first and second sessions were 29.18 ± 26.14 and 29.27 ± 26.19 cm3, respectively. The mean bone cyst volumes calculated by the second observer for the first and second sessions were 29.32 ± 26.36 and 29.23 ± 26.36 cm3, respectively. Statistical analysis showed no difference and high agreement between the first and second measurements of both observers. The Bland–Altman plots showed strong intraobserver and interobserver concordance in the measurement of the bone cyst volume. The mean total time necessary to obtain the cyst volume by the two observers was 5.27 ± 2.30 min.
Conclusion:
The bone cyst of the patients can be objectively evaluated using the planimetry method of the Cavalieri principle on CT. This method showed high interobserver and intraobserver agreement. This volume measurement can be used to evaluate cyst remodeling, including complete healing and cyst recurrence.
Introduction
Bone cysts are clear fluid-filled cystic lesions which tend to expand and weaken the bone. This benign lesion represents one of the most frequent osseous lesions. 1 The cysts have a predilection to occur in males more frequently than in females. 1,2 It usually occurs in childhood and adolescence (highest incidence between 5 years and 15 years of age). 1 Common locations include the proximal humerus and femur, although any section of any long bone may be involved. 3
Although the clinical features and diagnosis of cysts have been well described, the management of these lesions is controversial. Occasionally, the cyst is discovered incidentally during investigation for another complaint. If the cyst is not threatening the mechanical strength of the bone, close observation is the recommended management option. Usually, however, the cyst is symptomatic or is associated with a pathological fracture. 2 Management methods for these symptomatic patients or active cysts or cysts which enlarge during the observation period include injection, decompression, and combined surgical techniques. 2,4 Various success rates have been reported with these treatment options, although a complete cure is not guaranteed by any. 5 The aim of all these management options is to obtain clinical and radiological healing in the cyst. However, there is no standard method to understand healing. In literature, some radiographic classification systems have been defined for radiographic healing and although there are minor differences, all classify radiographic healing by the amount of opacification of the cyst and cortical thickening. 6,7
The volume of the cysts is important for various reasons. One is to determine healing of the cyst for objective measurements. In addition, the volume of the cyst is proportional to the risk of pathological fracture. The risk is determined by the percentage of the bone occupied by the cyst in the transverse plane. 8 Another risk for pathological fracture is explained by the radiographic cyst index. 9 Conversely, another study concluded that the radiographic cyst index was not validated as an accurate predictor of fracture. 10 In literature, the volume of similar pathological lesions has been calculated by different methods. In a study by Göbel et al., the tumor volume of Ewing sarcoma patients was calculated from plain X-rays and computed tomography (CT) scans according to whether the tumor shape was ellipsoid or cylindrical. 11 Glowacki et al. used the same method to calculate the volume of the bone cyst from X-rays. 12 Docquier et al. designed a semiautomatic segmentation method to measure the volume of a bone cyst from magnetic resonance imaging (MRI). 13 However, none of these methods for calculating volume has been widely accepted.
The stereological method of the Cavalieri principle is an effective method in volumetric measurements of biological structures. Planimetry and point-counting are two different stereological methods for estimating volume based on the Cavalieri principle. 14 Both methods have shown similar results and are correlated to each other. 14,15
In this study, it was aimed to estimate the bone cyst volume from CT scans of patients using the planimetry method of the Cavalieri principle.
Materials and methods
Approval for the study was granted by the local ethics committee of our institution. Twenty-five CT scans showing simple bone cyst, irrespective of gender, were obtained from the archives of the Department of Orthopaedics and Traumatology, Faculty of Medicine, Ondokuz Mayis University, Samsun, Turkey. The CT scans of bone cysts in the axial plane were acquired using a helical CT scanner (Toshiba Aquilion, Canon Medical Systems Corporation Toshiba, Dalian) by applying the following parameters, thickness: 1 mm, 120 kVp, 150–220 mAs. The axial scans in the Digital Imaging and Communications in Medicine (DICOM) file format were transferred to software (Horos v. 1.1.7) and reconstructed in the coronal plane to determine the upper and lower boundaries of the cysts. After the reconstruction process, the CT scans were divided into 1 mm sections in the coronal plane and saved as DICOM files. Each CT image showed one cyst in the bone. The cyst localizations were seven tibiae, six femurs, four radii, three humeri, three fibulae, one metacarpal, and one calcaneus. The total number of cyst samples was 25. Bone cysts with pathological fracture were excluded from the study as it was not possible to distinguish the boundaries of the cyst on the cross-sectional images. The volume of the bone cyst was estimated using the planimetry approach of the Cavalieri principle on CT images.
Planimetry method
The cross-sectional surface area of the cysts was measured by the planimetry method using ImageJ which is a free software distributed by the National Institutes of Health, USA (ImageJ, 1.37v: http://rsb.info.nih.gov/ij/). The digital images were transferred to ImageJ software and opened. If there were more than 30 sections containing tumor, the sections were resampled in ½ fraction to decrease the number of slices for efficient processing. The polygon selection tool was used to delineate the outermost boundaries of the cyst on every image of the coronal section plane (Figure 1). The program automatically measured the delineated area for each slice.
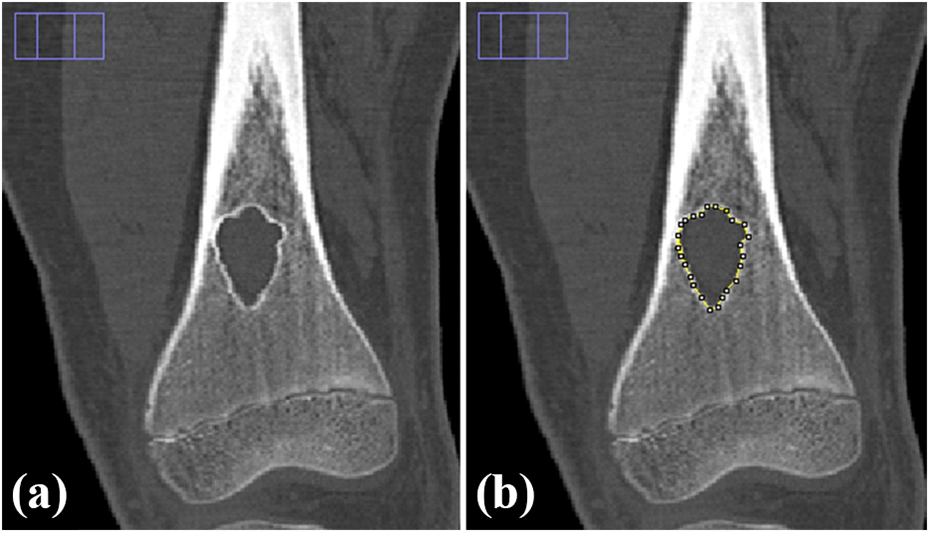
(a) A coronal slice of a femoral bone cyst and (b) delineation of the femoral bone cyst contours for the planimetric process.
The volume estimations were carried out by two independent observers (F. S./M. G.) to assess the interobserver reproducibility of the method. These procedures were repeated on CT images 1 month later by each observer using the same estimation parameters to check intraobserver repeatability. The observers were blinded to the estimation results of their first measurement and the results of the other observer. The volume of bone cysts was estimated by multiplication of the obtained sectional surface areas with the section thickness as described in previous reports by Acer et al. 15 and Kayipmaz et al. 16

where t (including interval) is the section thickness of consecutive sections and Σ A is the total sectional area of the cyst in consecutive sections. The coefficient error (CE) of planimetric volume estimations was calculated using the formula described in previous studies by Mazonakis et al. 17 The mean CE was 1.10 ± 0.61% (min–max, 0.36–2.83) for all the estimations. The simple calculation of bone cyst volume, CE of estimates, and other related data were performed using Excel (Microsoft, Washington, USA) as a spreadsheet. After the initial setup, and the preparation formula in a small macro program, the cut sectional surface area of the cyst, section thickness, and other data were input for each scan, and the volume of the cyst was calculated automatically. The mean time for the volume estimations was also recorded.
Statistical analysis
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) for Windows software (v. 22, IBM Corporation, USA) and MedCalc Statistical Software (v. 13.0, MedCalc Software, Belgium). The Bland–Altman method was used to evaluate concordance of the repeated measures for each observer and agreement between the measures of both observers in both sessions to determine the intraobserver repeatability and interobserver reproducibility of the Cavalieri method. A value of p < 0.05 was accepted as statistically significant. Intraobserver and interobserver agreement (variability) was also analyzed using the intraclass correlation coefficient.
Results
Two observers estimated the volumes of 25 bone cysts twice at an interval of 1 month. The overall mean volume (mean ± SD) of the bone cyst estimated by the Cavalieri principle was 29.25 ± 25.86 cm3.
The mean bone cyst volumes obtained by the first observer for the first and second sessions were 29.18 ± 26.14 and 29.27 ± 26.19 cm3, respectively. The Bland–Altman analysis showed that the mean cyst volumes estimated by the first observer for the first and second sessions differed between −0.82 cm3 and 0.64 cm3. There was no significant difference between the first and second measurements of the first observer (p > 0.233; Figure 2). There was also high agreement between the first observer’s estimation results in the first and second sessions (r = 0.999, p < 0.001).

The Bland–Altman plot showing the differences between the mean cyst volumes estimated by the first observer in the first and second sessions. The dashed line represents 95% limits of agreement.
The mean bone cyst volumes obtained by the second observer for the first and second sessions were 29.32 ± 26.36 and 29.23 ± 26.36 cm3, respectively. The Bland–Altman analysis showed that the mean cyst volumes estimated by the second observer for the first and second sessions differed between −0.56 cm3 and 0.75 cm3. There was no significant difference between the first and second measurements of the second observer (p > 0.180; Figure 3). There was also high agreement between the second observer’s estimation results in the first and second sessions (r = 0.999, p < 0.001).

The Bland–Altman plot showing the differences between the mean cyst volumes estimated by the second observer in the first and second sessions.
The Bland–Altman analysis showed that 95% of the mean of cyst volumes estimated by the first and second observers for the first and second sessions were −0.14 and 0.04 cm3, respectively. The Bland–Altman analysis indicated that the mean cyst volumes obtained by the first and second observers differed between −1.20 cm3 and 0.91 cm3 for the first session (p > 0.192) and between −0.84 cm3 and 0.92 cm3 for the second session (p > 0.664; Figures 4 and 5). There was no significant difference between the volume estimates of the two observers for both sessions. The interobserver agreement was found to be almost perfect in both sessions (r = 0.999, p < 0.001).
The Bland–Altman plots showed strong intraobserver (Figures 2 and 3) and interobserver (Figures 4 and 5) similarities in the measurement of the bone cyst volume using the Cavalieri principle. The mean total time required by the two observers to obtain cyst volume using the Cavalieri principle was 5.27 ± 2.30 min (range, 1.51–9.53 min). The mean bone cyst volume estimation results of the 25 bone cysts obtained by the first and second observers are shown in Figure 6.
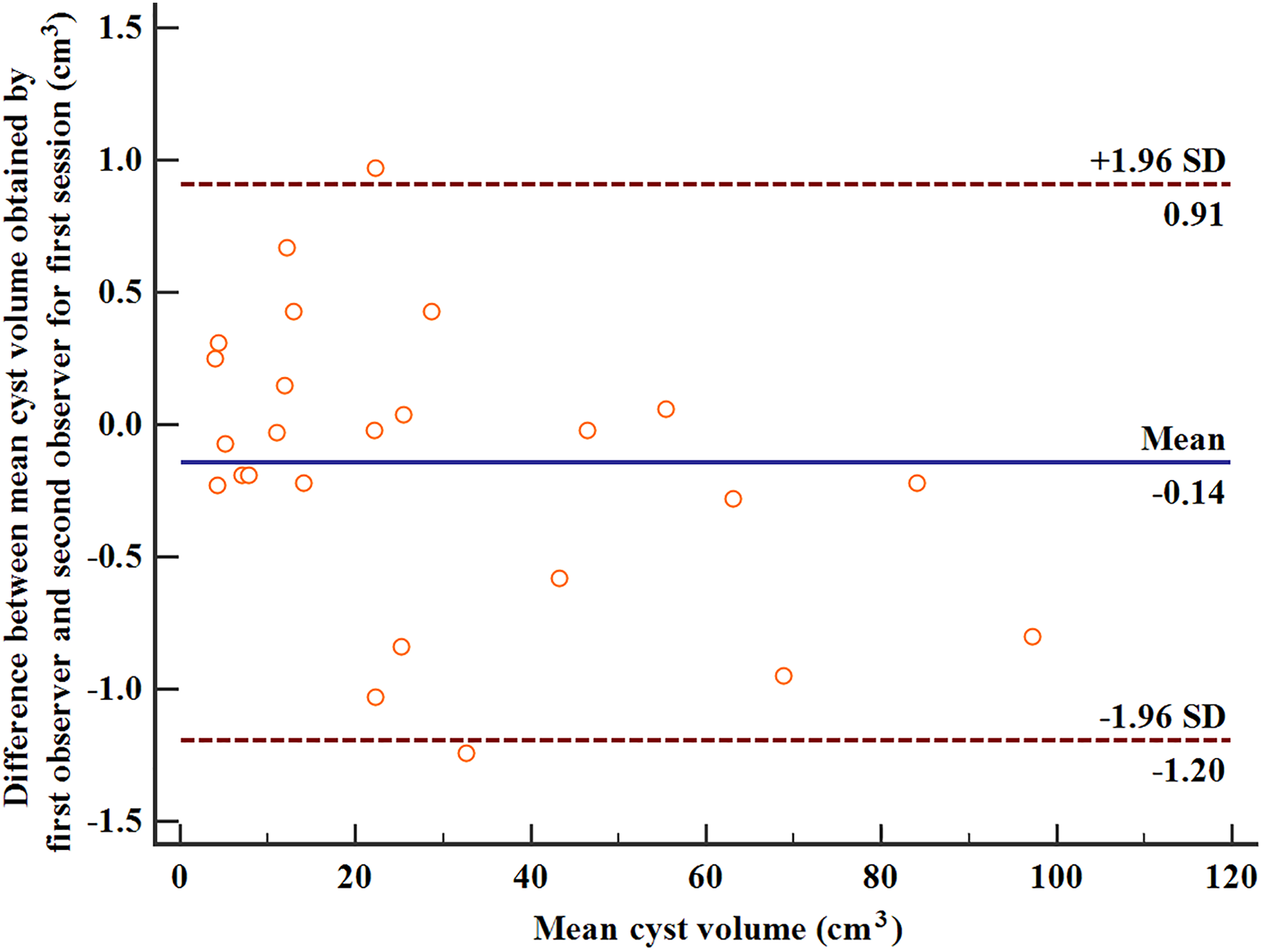
The Bland–Altman plot showing the differences between the mean cyst volumes estimated by the first and second observers in the first session.

The Bland–Altman plot showing the differences between the mean cyst volumes estimated by the first and second observers in the second session.
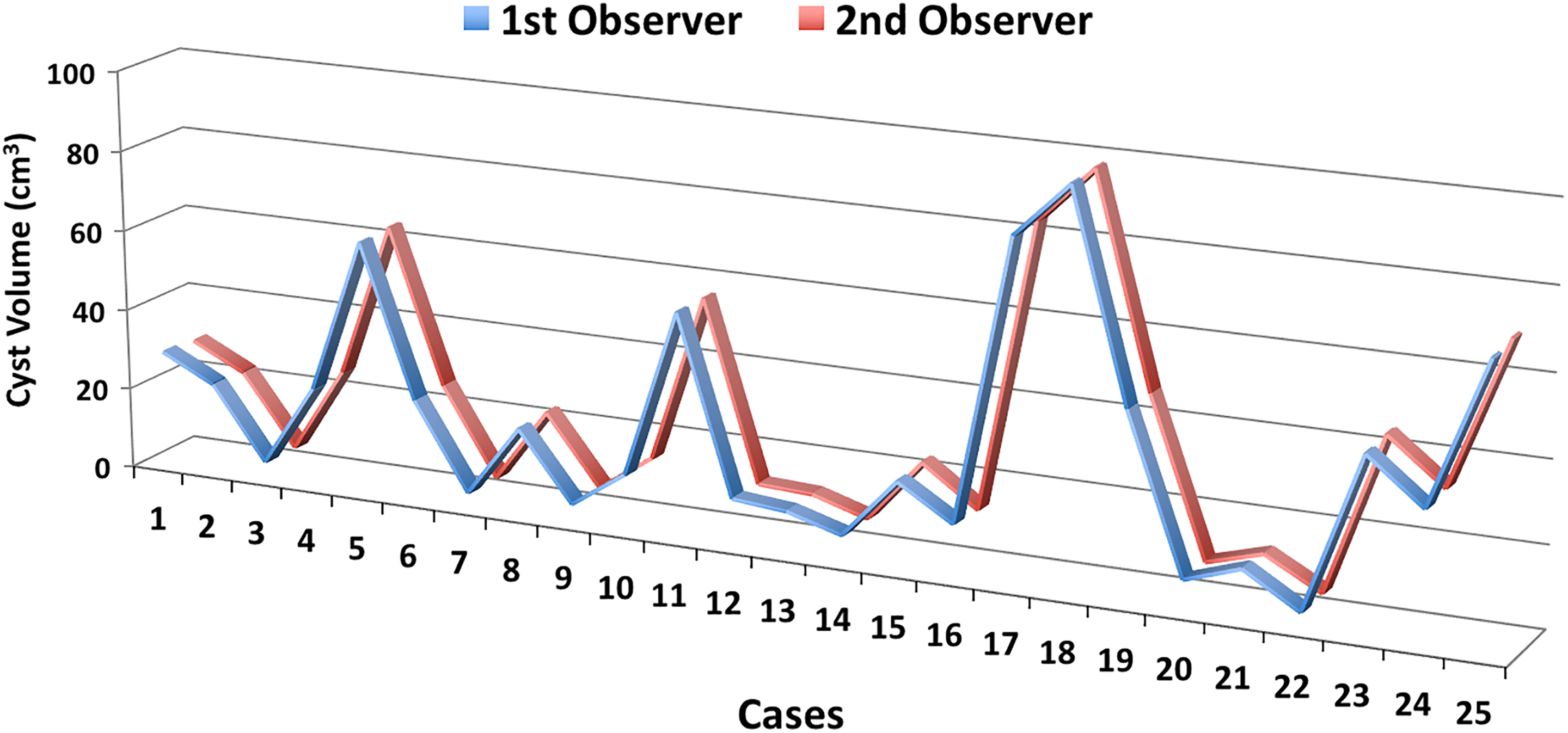
The mean bone cyst volume estimation results of the 25 bone cysts obtained by the first and second observers using the Cavalieri principle.
Discussion
In this study, bone cyst volume was calculated using the stereological planimetry method of the Cavalieri principle. The two blinded observers calculated similar volumes in the first and second sessions, which demonstrated the intraobserver repeatability of this method. The statistical analysis of the results of both observers showed a high level of agreement, which demonstrated the interobserver reproducibility of this method.
The natural history of the bone cysts is unclear. When cysts are immediately adjacent to a growth plate, they are named active cysts. When they have achieved some distance from the growth plate, they are named latent cysts. During the observation of a child with an active cyst, the volume of the cyst can be enlarged especially in the growth period. The volume of the cyst is also important to evaluate radiographic healing after an intervention. Another advantage of calculating the preoperative volume of the cyst is that an adequate volume of the therapeutic agent to fill the cyst can be prepared. The estimation of the exact volume of the cyst with an objective method is important in clinical practice.
In literature, various methods have been described by different authors to calculate similar pathological lesions. 11 –13 However, the repeatability and reproducibility of these methods are limited.
The Cavalieri principle is an effective and accurate method to estimate different biological structures. The planimetry method is the most commonly used technique for estimation of the volume. 15 The requirement for the application of the planimetry method is an entire set of two-dimensional slices through the object, provided they are parallel, separated by a known distance, and begins randomly within the object. These criteria are met by standard MRI and CT scanning techniques. 18,19 In addition to various organs and structures calculated by the planimetry method, bone pathologies were also calculated. Bulut et al. compared planimetry and point-counting methods to estimate the size of mandibular cysts on orthopantomogram and reported sufficient agreement of both methods. 14 The estimation of the volume by the planimetry method of sheep mandibular defects resulted in similar measurements to the actual volumes of the defects. 16
In the current study, 1 mm CT sections were used to calculate the volume of the cyst. Sezgin et al. compared various section thicknesses to estimate the volumes of the cavities on dry sheep mandibles and reported that slice thickness up to 1 mm can be chosen. 20
A limitation of this study is that this technique needs CT which exposes the patient to relatively large doses of radiation. However, when a bone cyst is first diagnosed, CT evaluation is recommended especially for lesions in areas such as the spine or pelvis which cannot be easily viewed on plain radiography. Another indication for CT is when there is concern regarding the structural integrity of a weight-bearing area. 4,5 However, repeated CT evaluations are less desirable in children.
In conclusion, this study showed that the bone cysts of patients can be objectively evaluated using the planimetry method on CT. This method showed high interobserver and intraobserver agreement. This volume measurement can be used to evaluate cyst remodeling, including complete healing and cyst recurrence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.