
Abstract
Objective:
This study aimed to investigate whether (1) the primary repair of rotator cuff tears can prevent the progression of osteoarthritis (OA) and (2) the quality of postoperative cuff integrity affects the incidence of osteoarthritic changes.
Methods:
A total of 86 patients treated with mini-open repair for rotator cuff tears over a minimum of 10 years of follow-up (mean ± standard deviation 11.1 ± 1.0 years) were retrospectively analyzed. Preoperative and postoperative radiographs of the affected and unaffected sides were compared, and the degree of OA was evaluated using the Samilson and Prieto classification. Magnetic resonance imaging was used to evaluate cuff integrity, classify patients into good and poor cuff integrity groups, and compare the degree of OA between the two groups.
Results:
OA deteriorated either significantly or to a similar degree on both sides postoperatively. However, OA progressed in significantly more cases on the affected side. A comparison between the aforementioned cuff integrity groups showed that the postoperative OA of the poor cuff integrity group was significantly worse than that of the good cuff integrity group on the affected side.
Conclusion:
Our study showed that even if rotator cuff tears are repaired, the progression of osteoarthritic changes cannot be halted. The progression of OA was affected by cuff integrity. Rotator cuff dysfunction due to poor cuff integrity was a risk factor for shoulder arthritis.
Introduction
There is no clear consensus on the characteristics of osteoarthritis (OA) of the shoulder joint after rotator cuff repair. Contributing factors for OA include systemic factors, such as age, gender, ethnicity, and genes, as well as local factors, such as the load on weight-bearing joints, history of trauma, obesity, and changes in the joint structure due to fractures. 1 Rotator cuff tears that are accompanied by OA progression and pain are diagnosed as rotator cuff tear arthropathy (RCTA). 2 OA of the shoulder joint is categorized into either primary or secondary OA. Secondary OA cases are commonly found in Asian populations, 3 and RCTA is one of the representative diseases of secondary OA.
Chalmers et al. followed up 67 shoulders for a median duration of 8 years with small- to medium-sized asymptomatic rotator cuff tears and found that 22% of patients exhibited OA progression. 4 Gerber et al. followed up 46 shoulders for a minimum of 10 years after latissimus dorsi transfer for massive rotator cuff tears and found that 48% of patients showed OA progression. 5 From these reports, we inferred that rotator cuff tears could be a local factor (especially in patients with trauma history) for OA, and that the progression of OA and RCTA may be prevented for cases with tear sizes that allow for primary rotator cuff repair. However, to the best of our knowledge, there were no reports that directly addressed this subject matter.
Moreover, whether or not the quality of the primary rotator cuff repair (quality of postoperative cuff integrity) affects the incidence of osteoarthritic changes, some researchers have reported varying results regarding the association between the degree of OA progression and rotator cuff integrity. 6 –9 One report demonstrated minimal progression of OA despite poor cuff integrity. 6 In contrast, others have reported that the maintenance of cuff integrity is correlated with the degree of OA progression after rotator cuff repair. 7 –9 Thus, the association between the degree of postoperative OA progression and cuff integrity remains unclear.
The purposes of this study are to clarify whether (1) the progression of osteoarthritic changes can be halted with rotator cuff repair and (2) the quality of postoperative cuff integrity affects the incidence of osteoarthritic changes.
Materials and methods
Study population
A total of 86 shoulders of 86 patients underwent primary repair for rotator cuff tears at our hospital between March 1998 and June 2004. For all cases, the follow-up periods were over a minimum of 10 years (mean ± standard deviation (SD) 11.1 ± 1.0 years). The following patients were excluded from this study: bilaterally operated patients, deceased patients, patients who underwent reoperation within the previous 10 years, patients who developed a shoulder disorder due to cerebral infarction, and patients who developed a shoulder disorder due to trauma. Ultrasound examination was performed at the final evaluation, and cases with cuff tears on the unaffected side were excluded.
The mean age at the time of operation was 60.4 years (SD ±7.3 years). The study included 46 male shoulders and 40 female shoulders (right 63 and left 23).
The preoperative tear size was assessed during open surgery and was categorized according to the classification of DeOrio and Cofield. 10 In all, 16 tears were small (<1 cm in length), 52 were medium (1–3 cm), 11 were large (3–5 cm), and 7 were massive (>5 cm).
This is a retrospective study. The study protocol was approved by the Ethics Committee of Azumi General Hospital ethics committee (reference number: 774), and written informed consent was obtained from all patients prior to surgery. The methods were carried out in accordance with the approved guidelines.
Surgical procedure and postoperative rehabilitation
In all patients, surgery was performed by the same shoulder surgeon using the mini-open deltoid split approach. 11,12 A 3-cm skin incision was made starting from the midpoint of the anterior edge of the acromion toward the axilla. The anterior deltoid muscle was divided longitudinally along the myofibers. The degenerative coracoacromial ligament was resected, and acromioplasty was carried out visually according to the Neer method. 13 The rotator cuff tear was repaired with a transosseous suture while keeping the position at 0° shoulder abduction after the degenerated edge of the cuff tear was resected.
All patients received postoperative therapy based on the same rehabilitation program. The postoperative arm was fixed with a shoulder abduction pillow for 2–4 weeks at 70° abduction and 30° horizontal flexion. Elbow joint active flexion/extension exercises, shoulder girdle (trapezius, rhomboids major and minor, levator scapulae, and serratus anterior) relaxation, and passive shoulder joint range of motion (ROM) training were started on the day after surgery. Two to four weeks after surgery, the pillow was replaced with a smaller shoulder abduction pillow. Three to five weeks after surgery, active ROM training was initiated in the neutral (zero) position. Three months after surgery, muscular strength reinforcement training was started on the extrinsic muscles, and light work was permitted. Heavy labor and sports were permitted without restriction 6 months after surgery.
Evaluation using radiographs
Radiographs of the affected and unaffected sides were obtained preoperatively and 10 years postoperatively using the same settings. The radiograph consisted of an anteroposterior exposure with the shoulder in internal rotation, external rotation, and elevation positions.
The radiographs were analyzed by an experienced and blinded shoulder joint surgeon with no knowledge about the disease history and clinical findings of each patient. The degree of OA on the radiograph was compared between the affected and the unaffected sides and between the preoperative and the 10-year postoperative time points.
We evaluated the degree of OA using the Samilson and Prieto classification. 14 OA was divided into four grades: 0 = normal, 1 = mild (osteophytes <3 mm on the humeral head), 2 = moderate (osteophytes between 3 mm and 7 mm on the humeral head or the glenoid rim), and 3 = severe (osteophytes >7 mm with or without articular incongruity).
We classified patients into either OA progression or no change group on the affected side. The medical histories, preoperative degree of OA, and shoulder function were compared between the two groups. Shoulder function was preoperatively evaluated according to the University of California Los Angeles (UCLA) shoulder score by the same physician and followed up for more than 10 years postoperatively. 15
Evaluation using magnetic resonance imaging
More than 10 years postoperatively, patients underwent magnetic resonance imaging (MRI), a GP Flex Coil with a 1.0-T unit (Signa Horizon Lx 1.0T, GE Healthcare, Chicago, Illinois, USA).
MR images were analyzed by an experienced and blinded shoulder joint surgeon with no knowledge about the disease history and clinical findings of each patient. Using spin-echo proton-weighted sequences (repetition time: 3000 ms, echo time: 7.4 ms, matrix: 256 × 192), spin-echo T2-weighted sequences (repetition time: 3000 ms, echo time: 90 ms, matrix: 256 × 192) and gradient-echo T2*-weighted sequences (repetition time: 440 ms, echo time: 20 ms, flip angle: 30°) were obtained. Sections were 4-mm thick with a 1-mm gap between sections.
Cuff integrity was evaluated with the classification reported by Sugaya et al. 16 The classification types were as follows: type I, repaired cuff appeared to have sufficient thickness compared with normal cuff with homogenously low intensity on each image; type II, sufficient thickness compared with normal cuff associated with partial high intensity area; type III, insufficient thickness with less than half the thickness when compared with normal cuff, but without discontinuity; type IV, presence of a minor discontinuity in only one or two slices on both oblique coronal and sagittal images; and type V, presence of a major discontinuity observed in more than two slices on both oblique coronal and sagittal images.
We classified patients into either good cuff integrity group (type I, II, and III) or bad cuff integrity group (type IV and V). The medical histories and the degree of OA were compared between the two groups.
Statistical analysis
Mann–Whitney’s U test was used to compare the degree of OA on radiographs between the affected and the unaffected sides and between the preoperative and the 10-year postoperative observation. Mann–Whitney’s U test was also used to compare the age, degree of OA, and UCLA score between the good cuff integrity group and the poor cuff integrity group in addition to the OA progression and no change group. The χ 2 of independence test was used to compare the gender, affected side, history of trauma, and tear size between the good cuff integrity group and the poor cuff integrity group in addition to the OA progression and no change group. Statistical analysis was performed using the Statcel software (version 3; OMS Institute, Tokyo, Japan), with the significance level set at 5%.
Results
Evaluation using radiographs
None of the patients had severe OA (Samilson and Prieto stage 3) in any category. In the preoperative classification of OA, there was no significant difference between the unaffected and the affected sides (p = 0.46). In the classification of OA 10 years postoperatively, OA of the affected sides was significantly worse than that of the unaffected sides (p < 0.001). On the affected side, OA was significantly worse 10 years postoperatively than preoperatively (p < 0.001). On the unaffected side, OA was also significantly worse 10 years postoperatively than preoperatively (p = 0.039; Table 1).
Comparison of the degree of OA on radiograph between the affected and the unaffected sides and between the preoperative and the 10-year postoperative time points.

OA: osteoarthritis.
With regard to the degree of OA progression, 55% of patients had OA progression on the affected side (no change: 39 cases, one stage worse: 41 cases, two stages worse: 6 cases), while 19% had OA progression on the unaffected side (no change: 70 cases, one stage worse: 16 cases, two stages worse: 0 cases).
The OA progression group comprised of 47 cases and the no change group comprised of 39 cases on the affected side. The preoperative UCLA score of the OA progression group was significantly worse than that of the no change group (p = 0.0090). The postoperative UCLA scores showed no significant differences between the OA progression and no change groups (p = 0.70). Patients with fair or poor UCLA scores (<27) were considered symptomatic, which resulted in six cases with OA progression (12.8%) and one case with no progression (2.6%). Other items showed no significant differences between the two groups (Table 2).
A comparison of the medical history, the preoperative degree of OA, and the UCLA score between the OA progression and the no change groups.
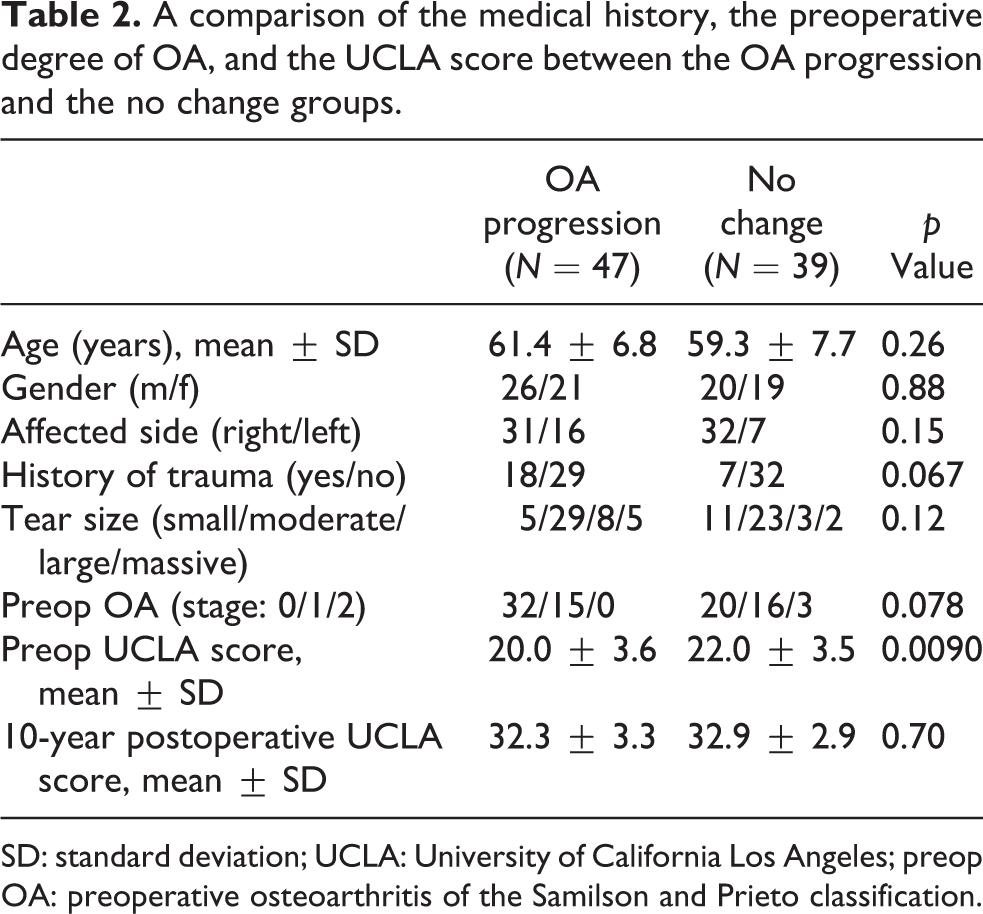
SD: standard deviation; UCLA: University of California Los Angeles; preop OA: preoperative osteoarthritis of the Samilson and Prieto classification.
Evaluation using MRI
The good cuff integrity group comprised 65 cases and the poor cuff integrity group comprised 21 cases. The tear size of the poor cuff integrity group was significantly larger than that of the good cuff integrity group (p = 0.0044). Other items showed no significant differences between the two groups (Table 3).
A comparison of the medical history between the good and the poor cuff integrity groups 10 years postoperatively.

SD: standard deviation.
On the unaffected side, there were no significant differences between the good and the poor cuff integrity groups 10 years postoperatively (p = 0.23). On the affected side, OA in the poor cuff integrity group was significantly worse than that of the good cuff integrity group 10 years postoperatively (p = 0.0024; Table 4).
A comparison of the degree of OA between the good and the poor cuff integrity groups 10 years postoperatively.
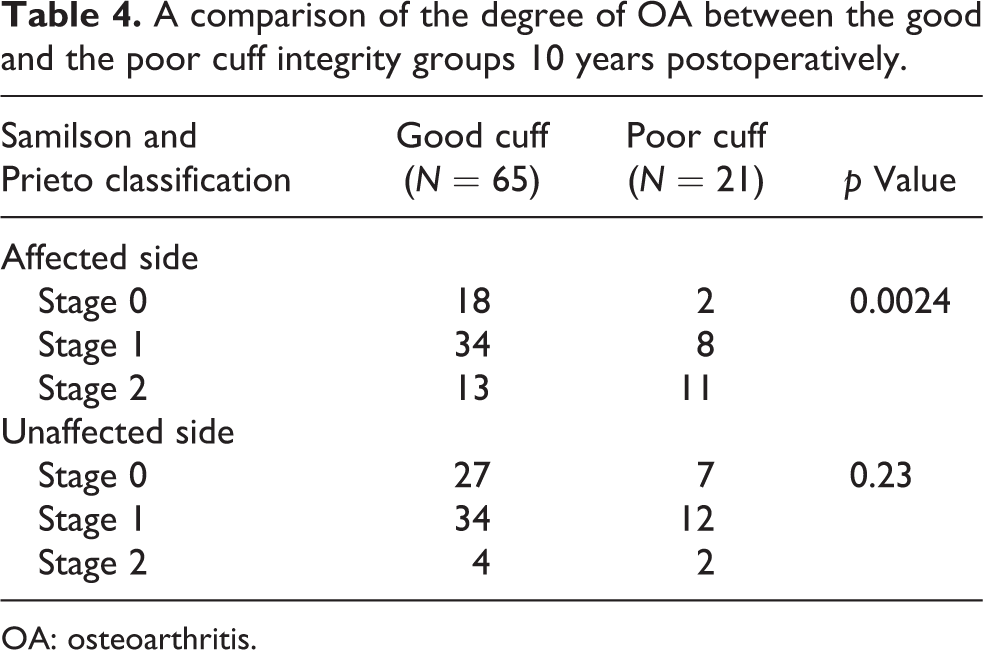
OA: osteoarthritis.
Complications
No intraoperative or perioperative complications were reported. None of the patients had neural injuries or wound infection problems.
Discussion
Contributing factors for OA include systemic factors, such as age, gender, ethnicity, and genes, as well as local factors, such as the load on weight-bearing joints, history of trauma, obesity, and the joint structure. 1 Moor et al. reported that a short acromion with an inferiorly inclined glenoid would be associated with glenohumeral OA. 17 We initially focused our study on the progression of OA after rotator cuff repairs over time. In general, the development of OA is believed to be associated with age. Kobayashi et al. reported that the prevalence of shoulder OA in the respondents younger than 65 years of age was 11.1%, whereas it was 20.3% in respondents aged 65 years and older. 3 This study showed that OA of the shoulder progressed on both the affected and the unaffected sides but occurred in significantly more cases on the affected side over a mean follow-up duration of 11.1 years postoperatively. Because the unaffected shoulder also showed OA, we confirmed that osteoarthritic changes occurred with age. Because the OA in the affected side had progressed to a more advanced stage compared with the unaffected side, we found that the progression of osteoarthritic changes cannot be halted even if the cuff tear had been once repaired.
Some investigators reported the rate of OA progression after primary rotator cuff repairs to be 18–20% at 9–10.5 years postoperatively. 18,19 In our study, 55% of patients had OA progression on the affected side. The rate of OA progression in our cases was greater than past reports. We believe that the increased rate is likely due to the older age of our patients (mean age 60.4 years) compared to past reports (mean age 51–58.1 years), the fact that retear cases and many manual laborers were included in our study, and how we evaluated our radiographic data. Although classification systems tend to rely on radiography taken from a single direction, we evaluated our data from three directions, which consisted of an anteroposterior exposure with the shoulder in internal rotation, external rotation, and elevation positions. We believe that this multidirectional evaluation enabled us to detect more subtle changes in the progression of OA compared to previous studies.
On comparing the OA progression with the no change group, the preoperative UCLA score of the OA progression group was significantly worse than that of the no change group. The medical histories and preoperative degree of OA showed no significant differences between the two groups. Flurin et al. showed no associations linking the risk of glenohumeral OA to the patient activity profile, history of trauma, or preoperative symptom duration. In contrast, statistically significant associations were identified between glenohumeral OA and age, male gender, initial tear severity, and the pain/mobility components of the preoperative Constant score. 20 In this study, low preoperative shoulder function scores were similar, but our results were different with regard to age, gender, and the initial tear size compared to past reports. We suspected that the low preoperative shoulder function score with poor ROM and muscle strength developed abnormal shoulder movement, which may have been a risk factor for the progression of OA.
The postoperative UCLA scores showed no significant differences between the OA progression and no change groups. Elia et al. reported good clinical results after open rotator cuff repair at an average follow-up of 11.4 years, despite 69% of patients exhibiting OA progression. 21 Small changes in OA may not induce changes in shoulder function if the degree of OA is not severe.
Retear rates after rotator cuff repairs have been previously demonstrated to be proportional to the initial tear size. 22 This study also shows that the tear size of the poor cuff integrity group was significantly larger than that of the good cuff integrity group.
Various theories have been reported concerning an association between the degree of OA progression and the cuff integrity. One report shows a favorably low OA progression rate (32%), despite poor cuff integrity. 6 On the other hand, there are also reports that OA is more common after poor cuff integrity cases than good cuff integrity cases (good: 21%, bad: 100% 8 ; good: 8.3%, bad: 36% 9 ; and good: 25%, bad: 46% 20 ). We compared the degree of OA between the good cuff integrity group and the poor cuff integrity group. On the affected side, the OA of the poor cuff integrity group was significantly worse than that of the good cuff integrity group 11.1 years postoperatively. Neer et al. reported that the causes of shoulder arthritis were shoulder instability due to rotator cuff dysfunction, decrease of the joint pressure, and decrease of the synovial fluid. 2 Konno et al. reported that the loss of rotator cuff function might lead to superior translation of the humeral head during arm elevation. 23 This abnormal superior migration may cause undue traction on the capsule and labrum, which may be a cause of shoulder arthritis. In our study, rotator cuff dysfunction due to poor cuff integrity was a risk factor for shoulder arthritis.
This study has several limitations. First, the sample size of patients was small due to the study being performed at a single center; future research would benefit from multicenter studies with a larger sample size. However, since the clinical and imaging evaluations were conducted by different physicians who did not perform the surgery in a blinded manner, we believe that objective data were obtained. Second, our cases were evaluated using radiographic images that may lead to poor reproducibility. However, since patients underwent radiographic evaluation using identical settings and positions at the same institution, we believe that objective data were obtained. Third, we used the Samilson and Prieto classification that was originally described for use in patients with dislocation arthropathy and did not use the Hamada classification and acromiohumeral interval that is specific to RCTA. Because none of the patients had severe OA in any category, Samilson and Prieto classification enabled us to detect more subtle changes in the progression of OA compared to others. Fourth, the study did not include MR images of the unaffected side. Although the unaffected side can include cases of asymptomatic rotator cuff tear, surgery was not performed on the unaffected side for the 11.1-year duration of the study. Ultrasonic examination was performed at the final evaluation, and there were no rotator cuff tears; thus, we believe that the unaffected side indicates normal shoulders.
Conclusion
Because the OA in the affected side had progressed to a more advanced stage compared with the unaffected side over a mean follow-up duration of 11.1 years postoperatively, we found that the progression of osteoarthritic changes cannot be halted even if the cuff tear had been once repaired. The progression of OA was affected by cuff integrity. Rotator cuff dysfunction due to poor cuff integrity was a risk factor for shoulder arthritis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.