
Abstract
Purpose:
The purpose of this study was to present a new radiograph of peritrapezial view and examine whether this view could supply clear and reliable radiographs of the joints around trapezium.
Methods:
The radiographs of peritrapezial and Robert views were taken on both hands of the 30 healthy volunteers (15 men and 15 women). The four peritrapezial joints were evaluated by two trained hand surgeons to find out whether these views could clearly show the joint spaces around the trapezium. Intra- and interobserver agreement for evaluation of each joint space and the ratio of joints which both of the two observers rated as clear joint space were compared between peritrapezial and Robert views.
Results:
The κ values of inter- and intra-observer reliability were, respectively, 0.559 and 0.715 in peritrapezial view and 0.462 and 0.355 in Robert view. The ratios of joints, which both of the two observers rated as clear joint space in each of the two time evaluations, were slightly higher in peritrapezial view than Robert view for the thumb carpometacarpal (100% vs. 96.7%) and scaphoid-trapezium joints (100% vs. 93.3%). In addition, these ratios were significantly higher in peritrapezial view than Robert view for the trapezium-index metacarpal (90.0% vs. 46.7%, p < 0.001) and trapezium-trapezoid joints (93.3% vs. 50.0%, p < 0.001).
Conclusion:
The peritrapezial view clearly shows the joint spaces around the trapezium. This view showed better inter- and intra-observer reliability for peritrapezial joints than Robert view especially in trapezium-index metacarpal and trapezium-trapezoid joint. This radiograph could provide a preliminary step for evaluating and managing pathologies of the peritrapezial joints.
Introduction
Complex shape of the thumb carpometacarpal (CMC) joint allows for multidirectional movement, including opposition. However, its unique shape makes it a difficult structure for evaluation using a simple radiograph 1 and makes it vulnerable to arthritic change. 2 Many studies have attempted to develop a reliable and reproducible method to obtain a high-quality radiograph that reflects the real morphology of the thumb CMC joint.
The Robert view (true anteroposterior view) and the lateral view are the most commonly used in clinical practice. Robert suggested the forced pronation position of wrist and forearm to overcome the relative obliquity of longitudinal axis of thumb CMC joint compared to anatomical axis of hand in 1936. 1 Since then, several modifications of image acquisition have been reported, but the basic concept have not been changed. 3 –5 Billing and Gedda emphasized the use of specific apparatus for fixing the hand to get the true lateral view of thumb in 1952. 6 The anatomical landmarks, such as the shape of trapezium and the superimposition of first metacarpal sesamoids, have been used to evaluate the accuracy of the lateral view. 6,7 However, these radiographs have been limited in terms of reliability and accuracy. 1,3,7,8
Thumb CMC osteoarthritis (OA) is a common and painful problem, especially for women. 9 Its prevalence was reported to be 25% among postmenopausal women 10 and the rate increased in proportion to older age in both sexes. 11 In cases of thumb CMC OA, several studies have reported the radiological incidence rates of concomitant arthritis in the joints around the trapezium, known as pantrapezial or peritrapezial arthritis: 43–86% in trapezium-index metacarpal joint, 0–35% in trapezium-trapezoid joint, and 7–48% in scaphoid-trapezium joint. 8,12 –14 Although the study designs differed, the reported incidence rates vary too greatly. Furthermore, North et al. 8 pointed out that the typical radiographs of the CMC joint could not correctly reflect anatomic changes of the peritrapezial joints. Thus, there has been a need for reproducible radiograph and specific radiological references of the joints around the trapezium for optimal evaluation and treatment.
We developed a new true posteroanterior view of the trapezium, the peritrapezial view, as well as a framework that enables easy reproduction of this radiograph by using 3-D printing technology. The purpose of this study was to present this new peritrapezial view and to examine whether this view could supply clear and reliable radiographs of peritrapezial joints (thumb CMC, trapezium-index metacarpal, trapezium-trapezoid, and scaphoid-trapezium joints).
Methods
Development of the peritrapezial view and framework
The peritrapezial view and its framework were developed by one of the authors (G.H.B). He found a position for the coronal surface of trapezium to be parallel to the horizontal plane (Figures 1 and 2). One healthy man was recruited as a volunteer, and his hand was manipulated into the designated position. The volunteer was directed to sequentially maneuver the wrist and hand as follows: 60° of wrist volar flexion, 30° of wrist ulnar deviation, 20° of wrist supination, 30° of thumb abduction, and 10° of thumb pronation with the hand in a palm-down position. After confirming the accurate posture with fluoroscopic examination, a rubber clay mold was made on which the hand was placed to create the desired posture. The grooves for the palm, wrist, and each finger were widened and flattened to reflect the hand size differences among individuals. At this point, a 3-D scan of the modified clay mold was performed (StereoScan, 3D systems, Germany), and the rough surfaces and sharp edges of the 3-D scanned image were then reprocessed using a 3-D designing tool (Geomagic Sculpt, Creo, San Hose, CA, USA). The final framework was produced by a 3-D printer (Fortus 450mc, Stratasys, Eden Prairie, MN, USA) based on the scanned images of the modified mold.

The peritrapezial view of the hand of a 21-year-old man (a) and its magnified version (b). The six joints around trapezium and trapezoid (thumb CMC, trapezium-second metacarpal, trapezium-trapezoid, scaphoid-trapezium, trapezoid-second metacarpal, and scaphoid-trapezoid joints) are clearly visible with parallel sclerotic bone margins. CMC: carpometacarpal.

The Robert view (a), the true lateral view (b), and the peritrapezial view (c) of the hand of a 23-year-old man. In Robert view, the peritrapezial joints are shadowed by soft tissue. Thumb CMC and scaphoid-trapezium joints are evident, but trapezium-second metacarpal and trapezium-trapezoid joints are overlapped by adjacent bones. In true lateral view, first metacarpal bone base is shadowed by second metacarpal bone base. In peritrapezial view, all the joints around trapezium and trapezoid, including thumb CMC, scaphoid-trapezium, trapezium-second metacarpal, trapezium-trapezoid, scaphoid-trapezoid and trapezoid-second metacarpal joints, are clearly visible without overlapping. CMC: carpometacarpal.
The framework was made of acrylonitrile-butadiene-styrene resin. It has radiolucency and is one of the ideal materials for conceptual modeling, functional prototyping, and manufacturing tools. Velcro was attached to the location of the distal radioulnar joint and the middle of fingers in order to fix the position of the wrist and hand during examination (Figure 3). We made three versions of framework according to the size (large/medium/small) by magnifying and minifying 30% of the 3-D scanned images. We registered patent for this framework in our country (Korean Patent System, patent number: 10-1654585).

The photographs of framework for peritrapezial view and placing the subject’s hand on the framework.
Subjects
In March 2015, 30 healthy volunteers (15 men and 15 women) were enrolled in this study. The inclusion criteria were (1) no history of disease affecting the bones and joints (rheumatoid arthritis, metabolic bone disease, etc.) or trauma on the wrist and hand and (2) healthy adults (over 19 years old) with completed bone growth. The radiographs of peritrapezial and Robert views were taken on both hands of the subjects by radiologic technicians who had no prior knowledge of the subjects. All of the peritrapezial views were taken using the medium size framework without specific difficulties. The radiologic technicians instructed the volunteers to put their hand on and fit their radial border of palm and wrist to the framework. In addition, the following information was collected: age, sex, and body mass index (BMI) which is derived from body weight and height. The Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire was obtained to analyze the functional normality of these subjects. The average DASH scores were 4.3 (SD 3.3) in men and 4.7 (SD 3.3) in women, which are compatible with the average DASH scores in the general population of the third decade (Table 1). 15 This study was approved by the institutional review board of our institution (ASMC-15-IRB-002).
The basic information of the enrolled subjects.

BMI: body mass index; DASH: The Disabilities of the Arm, Shoulder, and Hand.
Analysis of the joint spaces around the trapezium
The peritrapezial and Robert views were analyzed to find out whether these views could supply clear and reliable radiographs of the four peritrapezial joints. Two fellowship trained hand surgeons, who had no prior knowledge of the peritrapezial view independently, reviewed the 30 sets of radiographs consisted of peritrapezial and Robert views. Each observer was asked to rate yes or no, whether the four peritrapezial joint spaces around trapezium (thumb CMC, trapezium-index metacarpal, trapezium-trapezoid, and scaphoid-trapezium joints) have a clear radiolucent area between the parallel radio-opaque sclerotic margins in each radiograph. The same review was carried out 1 week later to evaluate intra-observer reliability. Observers were asked not to confer with each other regarding the scoring of the radiographs to reduce bias.
Statistical analysis
All statistical analyses were performed using IBM-SPSS ver. 22.0 software (IBM Corp., Armonk, North Castle, NY, USA) and a p value < 0.05 was considered significant. The κ multi-rater measure (Κ) was used to estimate intra- and interobserver agreement for evaluating the peritrapezial and Robert views. The Κ value was calculated for the ratings of observers whether the four joint spaces around trapezium are clearly visible in each radiograph. Interpretation of the Κ values was done using the scale proposed by Altman 16 : 0–0.20, poor strength of agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, good agreement; 0.81–1.0, very good agreement. In addition, ratio of joints, which both of the two observers rated as clear joint space in each of the two time evaluations, were compared between peritrapezial and Robert views using the χ 2 test in each of the four peritrapezial joints.
Results
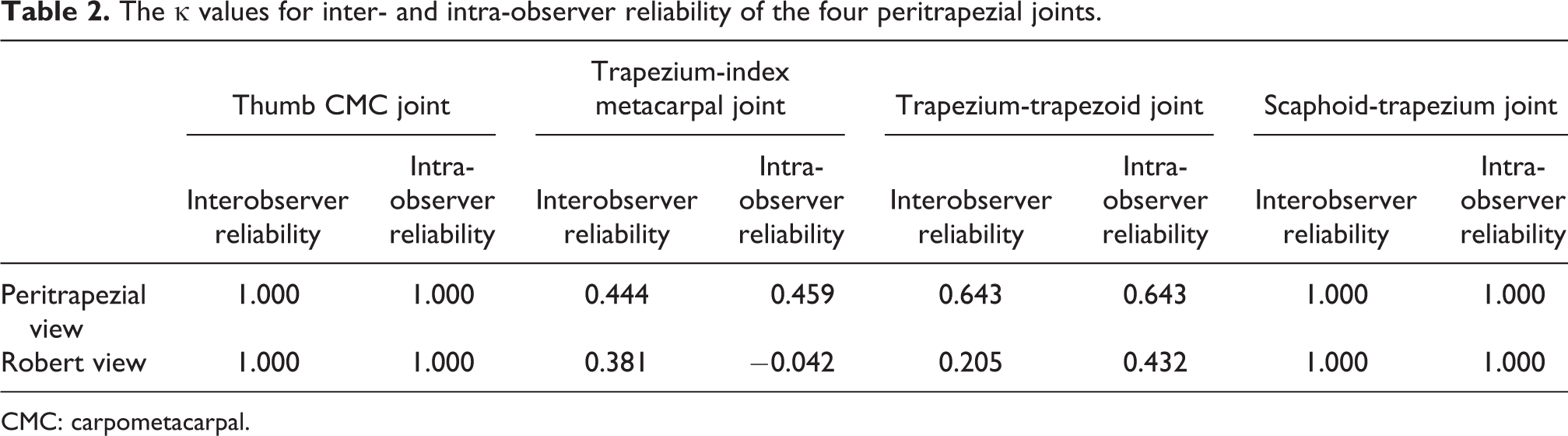
The κ values for inter- and intra-observer reliability of the four peritrapezial joints are described in Table 2. The κ value of inter- and intra-observer reliability was 1.000 (very good agreement) for the thumb CMC and scaphoid-trapezium joints in both of peritrapezial and Robert views. However, peritrapezial view showed higher κ value of inter- and intra-observer reliability than Robert view for the trapezium-index metacarpal and trapezium-trapezoid joints. In the analysis of 240 joints of 60 hands in 30 subjects, the κ values of inter- and intra-observer reliability for peritrapezial view were 0.559 (moderate agreement) and 0.715 (good agreement), and those for Robert view were 0.462 (moderate agreement) and 0.355 (fair agreement). The ratios of joints, which both of the two observers rated as clear joint space in each of the two time evaluations, were slightly higher in peritrapezial view than Robert view for the thumb CMC (100% vs. 96.7%) and scaphoid-trapezium joints (100% vs. 93.3%). In addition, these ratios were significantly higher in peritrapezial view than Robert view for the trapezium-index metacarpal (90.0% vs. 46.7%, p < 0.001) and trapezium-trapezoid joints (93.3% vs. 50.0%, p < 0.001).
The κ values for inter- and intra-observer reliability of the four peritrapezial joints.
CMC: carpometacarpal.
Discussion
With advances of the technology in medical field, computed tomography (CT) and magnetic resonance imaging (MRI) were developed and have been widely used to understand the 3-D structures of complicated anatomic sites. However, because of the radiologic hazard of CT and the cost of MRI, these imaging modalities could not be used for routine check-up. Therefore, an accurate and reproducible radiograph is essential to the diagnosis, classification, and management of musculoskeletal diseases. 2 In this study, we showed that peritrapezial view is more suitable for visualizing peritrapezial joints especially for trapezium-index metacarpal and trapezium-trapezoid joints than Robert view.
The Robert view and true lateral view have several limitations to be used as standard radiographs of the thumb CMC joint. First, a unique posture of the evaluated upper extremity is required to obtain an accurate image: the maximal pronation of the wrist and forearm in Robert view 1 and thumb adduction and forearm pronation of 15–35° in true lateral view. 7 These maneuvers are difficult for elderly patients with advanced arthritic changes. In addition, the radiological technicians need to be sufficiently skilled to adequately reproduce the unique posture for consistency. Second, the joint spaces could be overlapped by adjacent bones in these radiographs, which hinders an accurate evaluation. 8 The trapezium could be overlapped by adjacent structures in the Robert view depending on the extent of wrist pronation and the angle of the X-ray beam. 3 Moreover, the scaphoid-trapezium joint and the base of the first metacarpal bone are shadowed by the base of the second metacarpal bone in the true lateral view. Third, the other joints around the trapezium are not easily assessed using these images, except for thumb CMC and scaphoid-trapezium joints. 8,17 The Bett’s or Gedda’s view, used previously to minimize overlap and observe the peritrapezial joints, neither have good reliability nor they could be used widely owing to the complicated and inconsistently described hand positions, including thumb abduction and wrist volar flexion. 18 –20
The accuracy and reliability of the peritrapezial view are simultaneously achieved using the framework. Radiologic technicians do not have to direct the patients to shift their hand into certain positions, as the framework makes the coronal plane of the trapezium parallel to the horizontal plane. A high-quality radiograph is obtained by simply placing the patient’s hand on the framework and directing the radiograph beam perpendicularly to the base of the thumb. This simple procedure could reduce examination time and minimize the radiological hazard by reducing the imaging repetition caused by poor image quality.
3-D printing technology has been widely used in the medical field. To our knowledge, this is the first study to develop a real-size framework to assist radiologic evaluation using 3-D printing technology. This framework could be used in operation field after sterilization and used permanently, since it is constructed of materials with high heat tolerance and durability. We expect further studies to introduce new frameworks specific to enhance the radiologic evaluation of other body sites.
Several limitations of the present study require consideration. First, to introduce the peritrapezial view, we only analyzed the radiographs of young healthy adults. Further analyses of the peritrapezial view are needed with radiographs of patients with pathologies around the trapezium such as thumb CMC OA. Second, we did not compare the peritrapezial view with other radiological views or tools except Robert view. Additional studies are needed to evaluate the difference between peritrapezial view and other radiographic views or other image modalities, such as CT and MRI.
In conclusion, the peritrapezial view is a true posteroanterior view of the trapezium and clearly shows the joint spaces around the trapezium. This view showed better inter- and intra-observer reliability for peritrapezial joints than Robert view especially in trapezium-index metacarpal and trapezium-trapezoid joints. This radiograph could provide a preliminary step for evaluating and managing pathologies of the peritrapezial joints.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.