
Abstract
Background:
The purpose of this prospective study is to compare and correlate the clinical results of arthroscopic repair of a combined anteroinferior and superior labral lesion with those of an isolated anteroinferior labral lesion or type II superior labral tear from anterior to posterior (SLAP) lesion.
Methods:
A comparative study involving patients who underwent arthroscopic labral repairs in a tertiary hospital between 2010 and 2014 was conducted. A total of 96 patients were divided into three groups: Group A consisted of 61 patients with the anteroinferior labral lesion, group B consisted of 16 patients with the type II SLAP lesion, and group C consisted of 19 patients with the combined anteroinferior and superior labral lesion. Patient demographics, preoperative and postoperative pain scores, shoulder functional scores (Constant Shoulder Score, UCLA (University of California at Los Angeles) Shoulder Score, and Oxford Instability Score), and shoulder ranges of motion were measured and compared.
Results:
Except that patients from group B were generally older (28.8 vs. 22.2 for group A and 22.0 for group C, p = 0.04) at the time of surgery, no significant differences exist among the three groups in patient demographics and relevant clinical data. Preoperative and 2-year postoperative clinical outcomes, as well as the improvements, were comparable among the three groups. Low failure rates were observed for all three groups (6% vs. 10% vs. 11%, p = 0.999).
Conclusions:
Patients with the type II SLAP lesion underwent surgery at an older age. With appropriate surgical procedures, equivalent postoperative results can be expected for combined anteroinferior and superior labral lesion repair compared to isolated labral lesion repair.
Keywords
Introduction
The glenoid labrum provides attachments for the shoulder capsule and various tendons and ligaments, increases the glenoid surface by deepening the socket, and contributes to shoulder stability. Anteroinferior and superior labra are common anatomical locations prone to injuries. A Bankart lesion has been described many years ago as detachment of the anteroinferior labrum in patients with anterior shoulder instability. 1 Superior labral tear from anterior to posterior (SLAP) lesions, first described by Andrews et al., 2 are labral tears extending anteriorly from the posterior superior labrum, initially categorized by Snyder et al. 3 into four types. A type II SLAP lesion is the most common type, in which both superior labrum and biceps tendon are detached from the superior glenoid rim leading to instability of the labrobicipital complex. Although identified as a distinct clinical entity by prior studies, isolated SLAP lesions with no associated pathological findings are uncommon. 4 Maffet et al. 5 later added three more types (V–VII) to the original classification, with type V SLAP lesion representing an anteroinferior labral tear that continues superiorly and includes a separation of the biceps complex (a combination of Bankart and type II SLAP lesions).
Like the anteroinferior labral lesion, the type II SLAP lesion also contributes to glenohumeral instability. Studies have found that the superior aspect of the labrum and the biceps anchor restrict anterior glenohumeral translation. 6 –8 However, SLAP lesions can occur without significant instability. 2,3,5 A few studies have compared patients with a combined anteroinferior and superior labral lesion with those with an isolated anteroinferior labral lesion to evaluate the effect of concomitant SLAP repair on clinical outcomes. 9 –11 The association and difference between the type II SLAP lesion and the combined labral lesion, in terms of arthroscopic repair outcomes, have not been clearly defined. Therefore, the purpose of this study is to compare and correlate the clinical results of arthroscopic repair of the combined anteroinferior and superior labral lesion with those of the isolated anteroinferior labral lesion or type II SLAP lesion.
Materials and methods
A comparative study involving patients who underwent arthroscopic labral repairs in a tertiary hospital between 2010 and 2014 was conducted. Patients who met the following criteria (1) below 40-year old, (2) had traumatic shoulder injuries, and (3) had been prospectively followed up for at least 2 years—were included in the study. Patients with an associated rotator cuff injury, posterior labral injury, significant bony defect (exceeding 20% of the glenoid), humeral avulsion of the glenohumeral ligament, or previous stabilization procedures to the shoulder were excluded. All procedures were performed by two fellowship-trained sports surgeons.
A total of 96 patients satisfied the inclusion and exclusion criteria. They were divided into three groups based on the arthroscopic findings and operative procedures performed: Group A consisted of 61 patients with the anteroinferior labral lesion, group B consisted of 16 patients with the type II SLAP lesion, and group C consisted of 19 patients with the combined anteroinferior and superior labral lesion. Age of first dislocation, involvement in contact sports, and number of dislocations were evaluated in addition to population demographics.
All patients underwent general anesthesia with surgery performed in the beach chair position. For group A, the torn anteroinferior labrum was mobilized off the face of the glenoid before repair. For group B, any frayed or degenerative tissue was gently debrided before repair. For group C, the anteroinferior labral lesion was repaired before superior labral lesion repair. Repair of labral lesions was done using bioabsorbable suture anchors Gryphon™ and Lupine® (Mitek Sports Medicine, Raynham, Massachusetts, USA).
Postoperatively, the patients were admitted to the ward for overnight observation. The operated arm was placed in an arm sling. Pendulum motion exercises were allowed from postoperative day 1, before starting on passive range of motion (ROM) and strengthening exercises at 6-week post-operation during outpatient physiotherapy.
The outcomes measured in the study were visual analog scale for pain, shoulder functional scores using Constant Shoulder Score, UCLA Shoulder Score, and Oxford Instability Score, as well as the examiner determined ROM in both forward flexion and abduction. Both preoperative and postoperative data at 3, 6, 12 months, and 2 years were collected and analyzed. Failure was defined as a re-dislocation or a subluxation episode during the 2-year period. Kruskal–Wallis test and Fisher’s exact test were applied for continuous and categorical variables, respectively. A p value of <0.05 was considered significant.
The hospital ethics committee audited and approved the study protocol. The study was carried out in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Results
Table 1 summarizes the patient demographics and relevant clinical data. Except that patients from group B were older (28.8 vs. 22.2 for group A and 22.0 for group C) at the time of surgery, no significant differences exist among the three groups.
Preoperative patient data.a
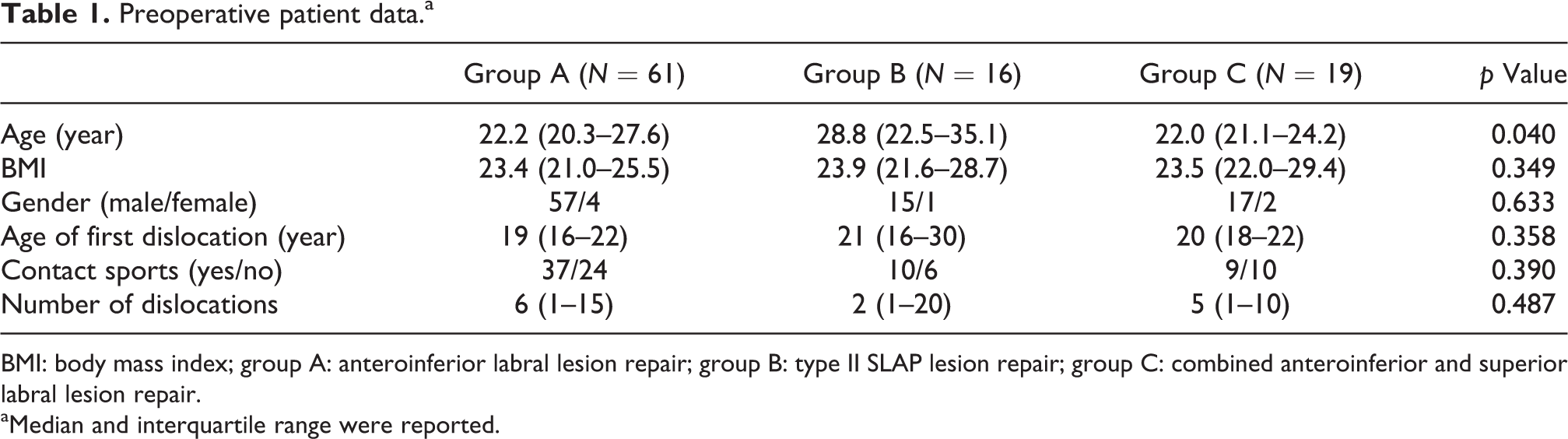
BMI: body mass index; group A: anteroinferior labral lesion repair; group B: type II SLAP lesion repair; group C: combined anteroinferior and superior labral lesion repair.
aMedian and interquartile range were reported.
Preoperative and 2-year postoperative clinical outcomes, together with the improvements, are presented in Table 2. Pain scores were comparable. There were no differences among the three groups in Constant Shoulder Score, UCLA Shoulder Score, and Oxford Instability Score. Slightly lower improvements in functional scores were observed in group C compared to the other two groups, without statistical significance. Both forward flexion and abduction ROM have improved significantly from preoperative values, for all three groups; however, they were not significantly different among each other at the 2-year follow-up. Improvements in ROM were highest in group C, but these did not achieve statistical significance. Failure rate was also similar in all groups, regardless of the type of repairs performed.
Clinical results at pre-op, 2-year follow-up, and respective improvements.a

VAS: visual analog scale; OIS: Oxford Instability Score; UCLA: University of California at Los Angeles; group A: anteroinferior labral lesion repair; group B: type II SLAP lesion repair; group C: combined anteroinferior and superior labral lesion repair.
aMedian and interquartile range were reported.
Chronological changes of shoulder functional scores during the 2-year follow-up period are shown in Figure 1. There existed a general trend of improvement across all scorings over time in all three groups. Nevertheless, slight reductions were observed for Constant Shoulder Score at 3 months postoperatively for all groups, which were compensated thereafter. Group C demonstrated minor decrements in shoulder functional scores at 2 years postoperatively, while the other two groups either maintained or improved on the scores.

Chronological changes of shoulder functional scores after repair. Group A: anteroinferior labral lesion repair; group B: type II SLAP lesion repair; group C: combined anteroinferior and superior labral lesion repair.
Discussion
This study is first of its kind, which compared clinical results of arthroscopic labral repairs using bioabsorbable suture anchors among patients with an anteroinferior, superior, or combined anteroinferior and superior labral lesion. The most significant finding of the study is that 2-year clinical outcomes of the three distinct yet related lesions are comparable, in terms of pain, shoulder functional scores, ROM, and failure rate. However, patients with the type II SLAP lesion underwent surgery at an older age.
In this study, 19 of 80 patients who had an anteroinferior labral lesion (groups A and C) developed the combined anteroinferior and superior labral lesion. This is comparable to studies by Hantes et al. (25 of 63) and Durban et al. (44 of 120), 10,11 substantiating that the combined labral lesion is not uncommon among glenoid labral lesions. Whereas the pathological etiology of the combined anteroinferior and superior labral lesion is unclear, this study tries to establish the relationship of the combined labral lesion with either the anteroinferior or superior labral lesion, in terms of clinical results of arthroscopic repair.
The anteroinferior labral lesion is the main cause of anterior instability, while the superior labrum and biceps tendon also play important roles in shoulder joint stability. A cadaveric study by Mihata et al. 12 demonstrated that arthroscopic repair of the SLAP lesion alone cannot fully restore anterior glenohumeral translation. Therefore, fixation of both the anteroinferior labral lesion and SLAP lesion to restore primary shoulder stability and prevent residual laxity has been advocated by many authors. 9,11,13,14 However, there was no consensus regarding whether anteroinferior labral lesion repair or SLAP lesion repair should be performed first. Warner et al. 13 and Hantes et al. 10 repaired the anteroinferior labral lesion prior to the SLAP lesion to avoid potential visual limitation. Cho et al. 9 reversed the procedures by repairing the SLAP lesion prior to the anteroinferior labral lesion to shorten the operative time to minimize soft tissue swelling and ease anteroinferior labral repair by creating a bowstring effect on the labrum after stabilization of the SLAP lesion.
Patients with the type II SLAP lesion underwent surgery at an older age, but the median age of first dislocation was comparable to the other two groups. Two commonly accepted biomechanical etiologies of SLAP lesions, acute traumatic injuries and chronic repetitive injuries, may possibly contribute to this. Impaction of the humeral head against the superior labrum and the biceps anchor, usually as a result of a fall onto an outstretched arm with the shoulder positioned in abduction and flexion, represents the acute traumatic etiology; whereas, a “peel-back” mechanism in overhead athletes, as proposed by Burkhart and Morgan, 15 requires repetitive minor trauma to the superior labrum, which was also supported by cadaveric biomechanical studies. 16,17 A group of patients with chronic injuries further delayed the time of surgery for group B, who started with a marginally older age of first dislocation.
The similarities between patients from groups A and C in terms of demographics associate the combined labral lesion more closely with isolated anteroinferior labral lesions rather than with SLAP lesions. Hantes et al. 10 found that the longer interval between injury and surgery and the increased number of dislocations played significant roles in the development of an extensive labral tear in the combined labral lesion. However, Durban et al. 11 advocated that the extent of the labral lesion may not be related to the number of dislocations but rather to the amount of energy exerted during the initial dislocation. Both hypotheses were neither reaffirmed nor rejected in this study. Patients from group C had a similar, if not shorter, interval between injury and surgery and a comparable number of dislocations compared to patients from either group A or group B. Their involvement in contact sports, which was used as a surrogate for high-energy trauma, was also comparable. Kim et al. also revealed that the extent of the labral lesion is not always related to the number of dislocations. 18 Acute high-energy trauma may cause extensive labral lesions, such as the combined anteroinferior and superior labral lesion, during the initial dislocation; whereas extensive labral lesions could also develop from repetitive dislocations chronically, which was the scope of the study by Hantes et al.
No significant differences in failure rate and functional outcomes were noted among the three groups. Similar findings were reported in other studies, where the combined labral lesion was compared with the isolated anteroinferior labral lesion. 10,11 This study further confirmed the equivalent functional outcomes between combined labral lesion repair and type II SLAP lesion repair. Correction of any soft tissue injury contributes more importantly to the results of arthroscopic repair of labral lesions than the extent and location of labral lesions. The overall failure rate of 9.4% in this series is in accordance with the low recurrence rates reported elsewhere. 10,19 While most other studies reported various functional scores only at pre-operation and final follow-up, chronological changes were documented and evaluated in this study. Patients from group C experienced an unexpected decline in functional scores at the last follow-up. It is unknown whether this is due to the larger size of the lesion therefore more suture anchors used or statistical error from the small sample size. The authors would follow up with the patients to observe the future trend.
Reduced shoulder ROM can be potential complications from repair of relatively extensive labral tears such as the combined anteroinferior and superior labral lesion. No difference in forward flexion and abduction ROM was observed at 2-year follow-up, similar to the findings from other studies. 9 –11,13,19 Surprisingly, patients with more extensive labral lesion repair showed better improvements in shoulder ROM than those with isolated lesion repair, although no statistical significance was observed. Cho et al. 9 also reported a slower ROM recovery in the combined labral lesion patients compared to the isolated anteroinferior labral lesion patients, attributing to the closure of the anterosuperior labrum during SLAP lesion repair. However, the slower ROM recovery was not observed in this study. Durban et al. 11 repaired the posterosuperior labrum and avoided anterosuperior labral and capsular plication to provide firm and stable fixation with some slack to the biceps anchor to maintain some external rotation. In addition, the superior and posterosuperior capsule was released, so they did not observe a significant decrease in external rotation in patients with the combined labral lesion. Restriction on shoulder ROM is also a common complication in patients with SLAP lesion repair, secondary to overtightening of the capsulolabral complex. 20 In the current series, a trend toward more limited ROM in group B was also observed. However, this did not translate into significant differences in both final ROM or improvements in ROM between groups B and C. Nevertheless, ROM in external rotation was not measured to confirm the deficit, which was one of the limitations of the study.
The other limitation of the study is the small sample size and uneven distribution of the three groups. A larger and similar group sample sizes would be ideal; however, there is sparse literature with at least 2-year follow-up.
Conclusion
In conclusion, patients with the type II SLAP lesion underwent surgery at an older age. The combined anteroinferior and superior labral lesion is a potential concomitant lesion in the anteroinferior labral lesion or SLAP lesion, and comparable postoperative results can be expected in terms of shoulder functional scores, ROM, and failure rate, despite the more extensive lesion size.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.