
Abstract
Introduction:
The purpose of this study was to compare the movement of the flexor pollicis longus (FPL) tendon on the distal radius during wrist and finger motions before and after removal of a volar plate in patients with distal radius fractures using transverse ultrasound and to evaluate the kinematic effects on the FPL by the removal.
Methods:
Twenty-five patients with distal radius fracture were evaluated quantitatively by transverse ultrasound using coordinates for the movement of the FPL on the distal radius during wrist and finger motions before and after the plate removal.
Results:
At all wrist positions, during finger motion, the FPL moved significantly more palmarly away from the radius after plate removal compared to before. However, the FPL was still situated more dorsoulnarly compared with unaffected side. Moreover, the FPL moved significantly most dorsally both before and after removal at the wrist dorsal flexion position with finger flexion.
Conclusions:
These findings suggested that any adhesion between the FPL and the pronator quadratus (PQ) muscle was released by removing the plate and that the FPL would approach original tendon movement. Additionally, it is speculated that any remaining atrophy and fibrosis of the PQ may be the reason for more dorsoulnar location of the FPL in the affected side compared with the unaffected one. This ultrasound evaluation may be useful in further understanding the FPL kinematics on the distal radius, and in appropriate treatment of the distal radius fracture with plate fixation for preventing FPL rupture.
Introduction
Many studies described that flexor pollicis longus (FPL) rupture was one of the severe complications after volar plating for the distal radius fracture and that it induced poor clinical results. 1 –7 The prevalence of FPL rupture has been reported in 1.8–12% of cases. 3,8,9 Moreover, several authors recommended that the plate should be removed early after the bone union of the distal radius fracture for preventing potential FPL rupture related to the plate fixation. 10 –12 By reducing the risk of FPL rupture may be of significance to better understand the movement of the FPL on the distal radius before and after the plate fixation.
Recently, the movement of the FPL on the distal radius has been described during wrist or finger motion after plate fixation using longitudinal or transverse ultrasound in healthy subjects and in patients with distal radius fractures after volar locking plate fixation. 13 –16 Ultrasound examination can be helpful to evaluate and elucidate various dynamic FPL movements quantitatively and noninvasively at the wrist in vivo. 16,17 However, using the longitudinal ultrasound method, it is difficult to maintain the transducer on the wrist except at the wrist neutral or slightly dorsal flexion position and to examine the transverse movement of the FPL. 13 –15 Conversely, the evaluation with transverse ultrasound can provide further detailed information about the FPL kinematics on the distal radius in the dorsal–palmar and the radial–ulnar directions at various wrist positions. 16,17
Currently, there have been a few studies examining the movement of the FPL on the distal radius during wrist and finger motion by transverse ultrasound in healthy subjects and in patients who underwent plate fixation for distal radius fractures. 16,17 Especially, our previous studies were the first to describe that the FPL moved most dorsally on the distal radius and that the distance between the FPL and the plate or the radius was the smallest at the wrist dorsal flexion position with fingers in flexion among all wrist positions during finger motion with transverse ultrasound. 16,17
However, there has been little research comparing the transverse ultrasound movement of the FPL during wrist and finger motions between before and after the plate removal in patients with distal radius fractures.
In the present study, using a technique introduced in our previous studies, we quantitatively evaluate the FPL movement as coordinates on the distal radius during wrist and finger motions with transverse ultrasound before and after plate removal in the affected and the unaffected sides of patients with distal radius fractures.
We consider that this ultrasound information can offer further knowledge and understanding of the kinematics of the FPL on the distal radius and suggest more appropriate treatments for the distal radius fracture with plate fixation, especially for preventing the FPL rupture.
Materials and methods
We recruited 25 patients with distal radius fractures treated with volar locking plate and subsequent removal of the plate (9 men, 16 women; mean age 54.1 years with a range of 27–75 years). Fractures were classified according to the Arbeitsgemeinschaft für Osteosynthesefragen (AO)/The Association for Study of the problems of Internal Fixation (ASIF) classification system as types A3 (n = 2), B3 (n = 1), C1 (n = 3), C2 (n = 12), and C3 (n = 7). All fractures were fixed using a volar locking plate system, variable angle locking compression plate (LCP) two-column Volar Distal Plate 2.4 (Depuy Synthes, Paoli, PA). All plates were placed proximal to the watershed line on the distal radius appropriately for each case and covered by the pronator quadratus (PQ) and the intermediate fibrous zone, as described by Orbay and Touhami. 5 According to Soong criteria, 6 review of radiographs after plating demonstrated grade 0 prominence in 21 cases (84.0%), grade 1 prominence in 4 (16.0%), and grade 2 prominence in none. Patients with distal radius fractures whose wrists were affected bilaterally were excluded. After signed consent was obtained from all patients in this study, we performed ultrasound examinations at 1 month before and 1 month after the plate removal.
The ultrasound image acquisition procedure has been reported previously. 16,17 Briefly, each patient was seated with the elbow flexed, the forearm supinated, and the shoulder in neutral position. The forearm of the patient was positioned on a custom-made table. An ultrasound scanner (Mylab Five; Hitachi Medical Corporation, Tokyo, Japan) equipped with an LA332 3.5/12MHz Hi-Definition linear array transducer (LA332) was used. All ultrasound examinations were performed by a single orthopedic surgeon (M.N.). The transducer was placed on the distal radius of the wrist (Figure 1). A custom-made device fastened to the transducer was attached at the patient’s wrist to maintain the transducer stable during wrist and finger motion. Additionally, the transducer was kept perpendicular to the skin of the wrist proximal to the wrist crease to identify the ulnar edge of the most distal portion of the distal radius without applying extra pressure to the soft tissue above the distal radius. It was easy to confirm this bony landmark in all wrists by transverse ultrasound . The FPL, the flexor digitorum superficialis (FDS) and flexor digiti profundus tendons, and the median nerve were identified by transverse ultrasound during full flexion and extension of all fingers. The transverse ultrasound image was obtained for each of the five wrist positions (neutral, 60° dorsal flexion, 60° palmar flexion, 40° ulnar deviation, and 10° radial deviation) during finger motion. Each wrist angle was measured with a goniometer (SD1-01; Suzukiiryo Inc., Tokyo) placed on the wrist. Both hands of each subject were imaged. The patients were asked to move from full extension to flexion of all fingers at each wrist position.

Setup of transverse ultrasound examination equipment.
All recorded images were examined, and the initial and final frames of each wrist and finger motion were selected. Additionally, the coordinates of the FPL were determined as follows (Figure 2). The reference point (P) was defined as the vertex of the palmar bony prominence of the radiolunate fossa of the distal radius on the watershed line that was mentioned as a transverse ridge bordering the pronator fossa distally by Orbay and Touhami. 5 The distances between P and the centroid of the FPL on the X-axis (x) and on the Y-axis (y) were measured. The position of the FPL was shown as a coordinate point (x mm, y mm). With increase in the distance of x or y, the FPL location deviated to the radial side or the palmar side, respectively.

Illustration of measuring the location of the FPL on the distal radius as a coordinate. FPL: flexor pollicis longus; FCR: flexor carpi radialis; FDS: flexor digitorum superficialis; FDP: flexor digiti profundus; MN: median nerve; RA: radial artery. P: the reference point defined as the vertex of the palmar bony prominence of the radiolunate fossa of the distal radius on the watershed line; x and y: the distances between P and the centroid of the FPL on the X-axis and Y-axis, respectively.
The results were calculated as the average of 3 measurements. All data were analyzed by SPSS 21.0J. The FPL displacements from the neutral wrist position to the other four wrist positions for all finger extension and flexion were statistically analyzed with the paired Student’s t test. Moreover, the displacement between all finger extension and flexion in each wrist position was statistically analyzed with the paired t test. Furthermore, the displacement before and after removal of the plate in each wrist position was statistically analyzed with the paired t test. A p value of less than 0.05 was considered statistically significant.
Results
Movement of the FPL at various wrist positions during finger motion
In the radial–ulnar direction, the FPL moved statistically significantly (p < 0.05) more ulnarly at the wrist dorsal flexion, palmar flexion, and ulnar deviation positions and more radially at the radial deviation position than at the wrist neutral position in full extension and flexion of finger before and after plate removal in the affected and unaffected sides (Figure 3).

Radial displacement of the FPL from P in the radial–ulnar direction during wrist and finger motion. FPL: flexor pollicis longus.
Moreover, the FPL moved statistically significantly (p < 0.05) more ulnarly in full flexion of fingers than in full extension of fingers at all wrist positions both before and after the plate removal in the affected and unaffected sides (Figure 3).
In the dorsal–palmar direction, the FPL moved statistically significantly (p < 0.05) more dorsally at the wrist dorsal flexion and ulnar deviation positions and more palmarly at the palmar flexion and radial deviation positions than at the wrist neutral position in full extension and flexion of fingers before and after the plate removal in the affected and unaffected sides (Figure 4). Especially, the FPL moved statistically significantly (p < 0.05) most dorsally at the wrist dorsal flexion position among all wrist positions before and after the plate removal in the affected and unaffected sides.

Palmar displacement of the FPL from P in the palmar–dorsal direction during wrist and finger motion. FPL: flexor pollicis longus.
Furthermore, the FPL moved statistically significantly (p < 0.05) more dorsally at the wrist dorsal flexion, palmar flexion, and ulnar deviation positions and more palmarly at the wrist neutral and radial deviation positions in full flexion of fingers than in full extension of fingers before and after the plate removal in the affected and unaffected sides (Figure 4).
Comparison of the movements of the FPL before and after the plate removal in the affected and unaffected sides
In the radial–ulnar direction, the FPL moved statistically significantly (p < 0.05) more radially after the plate removal than before at all wrist positions in full extension and flexion of fingers (Figure 3). Before and after the plate removal in the affected and unaffected sides, the FPL moved within the area from 5 mm to 10 mm at the radial side of P on the distal radius during wrist and finger motion.
Moreover, in the dorsal–palmar direction, the FPL moved statistically significantly (p < 0.05) more palmarly after the plate removal than before at all wrist positions in full fingers extension and flexion (Figure 4). Furthermore, the distance between the FPL and the plate or the distal radius in the palmar–dorsal direction at wrist dorsal flexion position in full fingers flexion was statistically significantly the smallest among all wrist positions (p < 0.05) both before and after the removal. The distance of the wrist dorsal flexion position in full flexion of fingers after the plate removal was greater than that before the removal. The average distances were 0.3 mm ± 0.14 mm before the removal and 1.0 mm ± 0.15 mm after the removal. On the other hand, the distance was 1.5 mm ± 0.18 mm in the unaffected side. Additionally, the distance after the removal was statistically significantly smaller than that in the unaffected side.
In Figure 5, we summarized the FPL movement on the distal radius in the flexion fingers at varied wrist positions before and after the plate removal in the unaffected side (Figure 5).
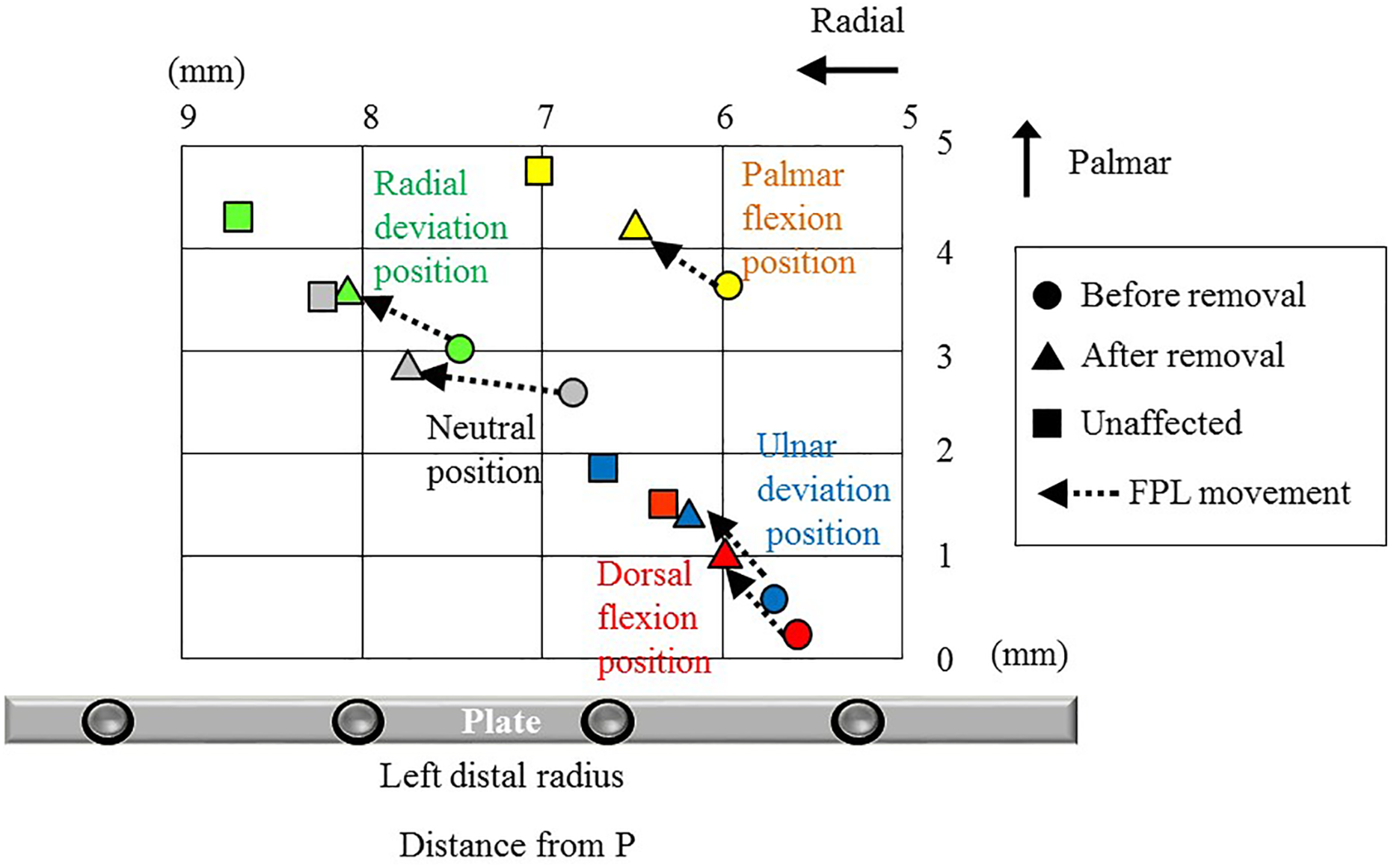
The distance from P to the FPL during the wrist motion with flexion of all fingers on the distal radius (average value). FPL: flexor pollicis longus. •: before plate removal in the affected side; ▴: after plate removal in the affected side; ▪: in the unaffected side; ⇠: the movement of the FPL.
Discussion
Recently, several studies focused on the movement of the FPL on the distal radius during wrist and finger motions using longitudinal or transverse ultrasound in healthy subjects or patients with distal radius fracture with volar locking plate fixation, studying the risk of the FPL rupture. 13 –17 Despite the importance of researching the kinematics of the FPL for preventing the tendon rupture related to plate fixation, there has been little information detailing the movement of the FPL on the distal radius during wrist and finger motions after the plate removal by ultrasound or by other means. Examining quantitatively the dynamic transverse ultrasound movement of the FPL during wrist and finger motion before and after the plate removal may be useful in obtaining further knowledge of kinematic and biomechanical changes of the FPL in patients with distal radius fractures.
Our previous studies quantitatively reported the transverse ultrasound movement of the FPL on the distal radius as coordinates during wrist and finger motions in healthy subjects and patients with distal radius fracture. 16,17 Moreover, our reports described that the FPL moved more dorsally on the affected side than on the unaffected side in the patients with the distal radius fractures with plate fixation at all wrist positions during finger motion. 16 In addition, we demonstrated that the FPL moved most dorsally at the wrist dorsal flexion position with finger flexion among all wrist positions during finger motion. 16,17
In the current study, using the same previous technique, we have for the first time to our knowledge investigated the FPL movement patterns on the distal radius during wrist and finger motions before and after the plate removal in the affected and the unaffected sides of patients with distal radius fracture, to evaluate the biomechanical effect of the plate removal. Subsequently, at all wrist positions during finger motion, the FPL moved significantly more palmarly after removal than before and moved away from the distal radius (Figure 5). Especially, at the wrist dorsal flexion position with finger flexion both before and after removal, the FPL moved significantly most dorsally, and the distances between the FPL and the plate or the distal radius was the smallest among all wrist positions during finger motion. Moreover, the distance after the plate removal was statistically significantly larger than those before removal.
These findings suggested that any adhesion between the FPL and the PQ was released by removing the plate, and the FPL moved greatly palmarly at all wrist positions and approached original tendon movement. In addition, they showed that the FPL would not be irritated by the watershed line of the distal radius. However, at all wrist positions during finger motion, the FPL after removal in the affected side was still situated more dorsally compared with the unaffected side (Figure 5). The distance between the FPL and the plate or the radius after removal in the affected side was also statistically significantly smaller than that in the unaffected side. Furthermore, the average distance was 0.3 mm before the removal, 1.0 mm after the removal, and 1.5 mm in the unaffected side at the wrist dorsal flexion position with finger flexion, which is when the FPL moved closest to the plate or the distal radius. Kadoma et al. found that the average distance between the FPL and the distal volar margin of the volar locking plate by longitudinal ultrasound was 0.7 mm at the wrist neutral position and 0.5 mm at the wrist maximal dorsal flexion in patients with distal radius fracture with plate fixation, which is in line with our study findings. 14 Moreover, a statistically significant relation was found between the ultrasonographic distance and intraoperative findings, that is, the thickness of intermediate tissue between the FPL and the distal volar margin of the plate. 14
Additionally, the longitudinal ultrasound views of both the FPL and the PQ on the distal radius are also shown in Figure 6 at wrist neutral position before and after the plate removal in both the affected and the unaffected sides. From these findings, it is speculated that any remaining atrophy and fibrosis of the PQ may be the reason for more dorsal location of the FPL at all wrist positions after the plate removal in the affected side compared with the unaffected side. Thus, in the future it may be considered necessary to examine the movement of the FPL by transverse ultrasound regularly after the plate removal.

Longitudinal ultrasonographic image of the distal radius. FPL: flexor pollicis longus; PQ: pronator quadratus. A: before plate removal in the affected side; B: after plate removal in the affected side; C: in the unaffected side.
There are some limitations to this study. First, we examined a relatively small group. A larger group with distal radius fractures may provide more detailed information with regard to FPL movement. Second, all measurements were performed by a single examiner. Therefore, interobserver reliability could not be evaluated although, in the current study, a custom-made transducer fixing device was placed to reduce examiner dependency on the patient’s wrist during wrist or finger motion. Third, we could not evaluate the relationship between the FPL-plate distance and the degree of tendon damage because clinically, even if the FPL are in contact with the plate, all cases are not necessarily tendon injured. Finally, the difference in the plate position for the distal radius fracture, according to Soong criteria, 6 was not evaluated. Increasing the group size may enable further examination regarding both the extent of the FPL movement on the radius in detail and the relationship between the distance between the FPL-plate distance and the degree of tendon damage.
In conclusion, this study quantitatively showed the detailed movement of the FPL on the distal radius during wrist and finger motions compared with before and after the plate removal using transverse ultrasound by a coordinate system in patients with distal radius fracture. Consequently, the current study described that there were significant differences in the FPL movements on the distal radius before and after the plate removal in the affected and unaffected sides. This study suggested that these FPL movement patterns would help to depict the release of any adhesion between the FPL and the PQ on the distal radius and to confirm the efficacy of removing the plate. This transverse ultrasound evaluation may be useful in the obtaining further knowledge and understanding the kinematics of the FPL on the distal radius and in suggesting more appropriate treatment of the distal radius fracture with plate fixation, especially for preventing the FPL rupture.
Further studies comparing the FPL movement between early and long term after the plate removal should be conducted in patients with distal radius fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.