
Abstract
Purpose:
This study compared the functional outcome and repair integrity of arthroscopic rotator cuff repair according to articular-side repair state in full-thickness tears.
Methods:
We prospectively enrolled 80 consecutive patients with full-thickness rotator cuff tears of 1.5–3.5 cm at the anterior to posterior dimension. These patients were divided into two groups according to intraoperative articular-side repair state during operation: complete and incomplete repair groups. Repair integrity was evaluated at 6 months after the operation by magnetic resonance image or ultrasonography. Clinical outcomes were evaluated at 1 year and 2 years postoperatively. Four outcome measures were used in this study: visual analog scale pain score, American Shoulder and Elbow Surgeons (ASES) score, the Shoulder Rating Scale of the University of California at Los Angeles (UCLA) score, and range of motion.
Results:
At 2-year follow-up, the average UCLA, ASES, and constant score improved significantly to 32.46, 87.94, and 79.69, respectively, in the complete group and to 32.50, 87.65, and 78.92, respectively, in the incomplete group. The UCLA, ASES, and constant score improved in both groups postoperatively (all ps < 0.000); however, there was no significant difference between the two groups (p = 0.960, 0.921, and 0.796, respectively). The re-tear rate was 13.7% in the shoulders that underwent complete repair and 33.3% in the shoulders that underwent incomplete repair; this difference was statistically significant (p = 0.041).
Conclusion:
Regardless of the repair state of articular-side rotator cuff, the arthroscopic rotator cuff repair resulted in comparable functional outcomes between two groups at short-term follow-up. However, patients who repaired articular-side rotator cuff incompletely revealed higher re-tear rate after operation than those who repaired completely.
Introduction
Rotator cuff tears comprise the majority of shoulder lesions in adult patients. In general population, the prevalence of rotator cuff tear was 22.1%, which increased with age. 1 In spite of these high incidence rates, rotator cuff repair is not always associated with clinically satisfactory outcomes. Because multiple factors have been shown to be associated with a less favorable outcome following rotator cuff repair, such as age, sex, smoking status, larger tear size, poor tendon quality, fatty degeneration of cuff muscle, poor repair integrity, and repair technique. 2 –11
We hypothesized that repair state of articular-side rotator cuff would have an effect on clinical outcomes and repair integrity after operation. We considered that patients with complete repair of articular-side rotator cuff during operation would result in higher clinical outcomes than for patients with incomplete repair of articular-side rotator cuff. However, to our knowledge, no reported study compared clinical and radiological outcomes of arthroscopic rotator cuff repair procedure according to the repair state of articular-side rotator cuff.
We compared the functional outcome and repair integrity of the arthroscopic suture-bridge repair methods in full-thickness rotator cuff tears according to the repair state of articular-side rotator cuff.
Materials and methods
Patient selection
Between October 2013 and October 2014, we prospectively enrolled 80 consecutive shoulders (80 patients) with full-thickness rotator cuff tears of 1.5–3.5 cm at the anterior to posterior dimension, which were treated using an arthroscopic suture-bridge technique. All operations were performed by a single surgeon (K.C.K.) in one hospital setting. The indication for surgery was failure of nonoperative treatment, which included a physical therapy program and, in some cases, a corticosteroid injection.
Enrolled 80 consecutive patients were divided into two groups according to the intraoperative articular-side repair state during operation: complete and incomplete repair groups. The complete repair was defined as complete coverage of the footprint of rotator cuff after rotator cuff repair. We used the following inclusion criteria: (1) full-thickness supra- and/or infraspinatus tear with an anteroposterior (AP) length of 1.5–3.5 cm and (2) repair of the rotator cuff tear using an arthroscopic suture-bridge technique. We used the following exclusion criteria: (1) full-thickness rotator cuff tear with an AP length of <1.5 cm or >3.5 cm, (2) partial rotator cuff repair, (3) repair of the rotator cuff tear using a mini-open or open repair method, (4) combined full-thickness subscapularis tear requiring concomitant repair, (5) combined acromioclavicular joint arthritis requiring concomitant distal clavicle resection, (6) neurological involvement, (7) revision operation, (8) operation using the suture-bridge technique after the conversion of a partial-thickness rotator cuff tear to a full-thickness lesion, and (9) arthritic changes in the glenohumeral joint. Important demographic differences between the two groups are listed in Table 1.
Demographic and surgical data.
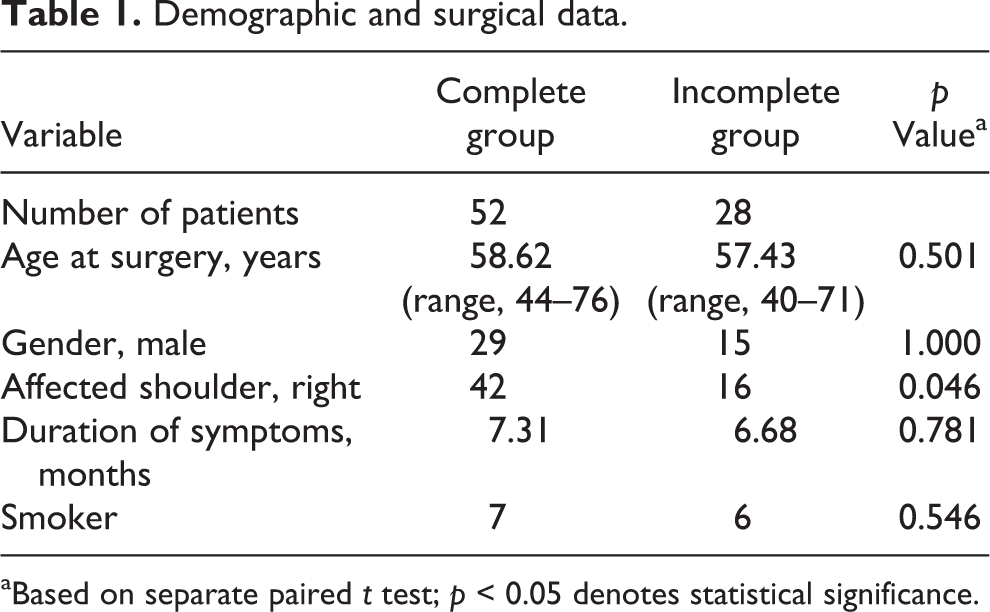
aBased on separate paired t test; p < 0.05 denotes statistical significance.
The study was approved by our institutional review board (IRB) and the need for informed consent from all patients was waived (IRB No. CNUH 2016-11-021).
Clinical and radiological evaluation
Enrolled patients returned for a follow-up functional evaluation at 1 year and 2 years after the operation. Clinical data were collected preoperatively and postoperatively at the 1 year and 2 years follow-up by two orthopedic surgeons. Four outcome measures were used in this study: visual analog scale (VAS) pain scores, American Shoulder and Elbow Surgeons (ASES) score, the Shoulder Rating Scale of the University of California at Los Angeles (UCLA), and range of motion (ROM). Active ROM was measured goniometrically, and passive ROM was not measured. Active ROM included forward flexion (FF) and abduction (Abd) measured with the patient in a standing position, and external rotation assessed while the patient was standing with the arm in an adducted position.
Enrolled patients returned for follow-up magnetic resonance image (MRI) or ultrasonography (US) evaluation to confirm the integrity of the repaired cuff at 6 months after operation. One specialized musculoskeletal radiologist performed all follow-up US examinations using an IU-22 system (Philips Healthcare, Bothell, Washington, USA). The MRI and US images were evaluated by an experienced radiologist. A recurrent tendon defect was diagnosed by US when a distinct hypoechoic or mixed hyper- and hypoechoic defect was visualized in both the transverse and longitudinal planes. A full-thickness re-tear was diagnosed when a focal defect was present in the rotator cuff into which the deltoid muscle could be compressed with a probe to separate the torn tendon ends or when the cuff retracted to such an extent that the torn ends could be distinctly visualized. MRI was used to classify the integrity of the tendon into one of two categories: (1) intact (sufficient thickness, Sugaya types I and II) or (2) insufficient/not healed/retorn (ranging from insufficient thickness (<50% normal cuff thickness) to discontinuity, Sugaya types III–V). 12 Important clinical differences between the two groups are listed in Table 2.
Clinical and surgical data.
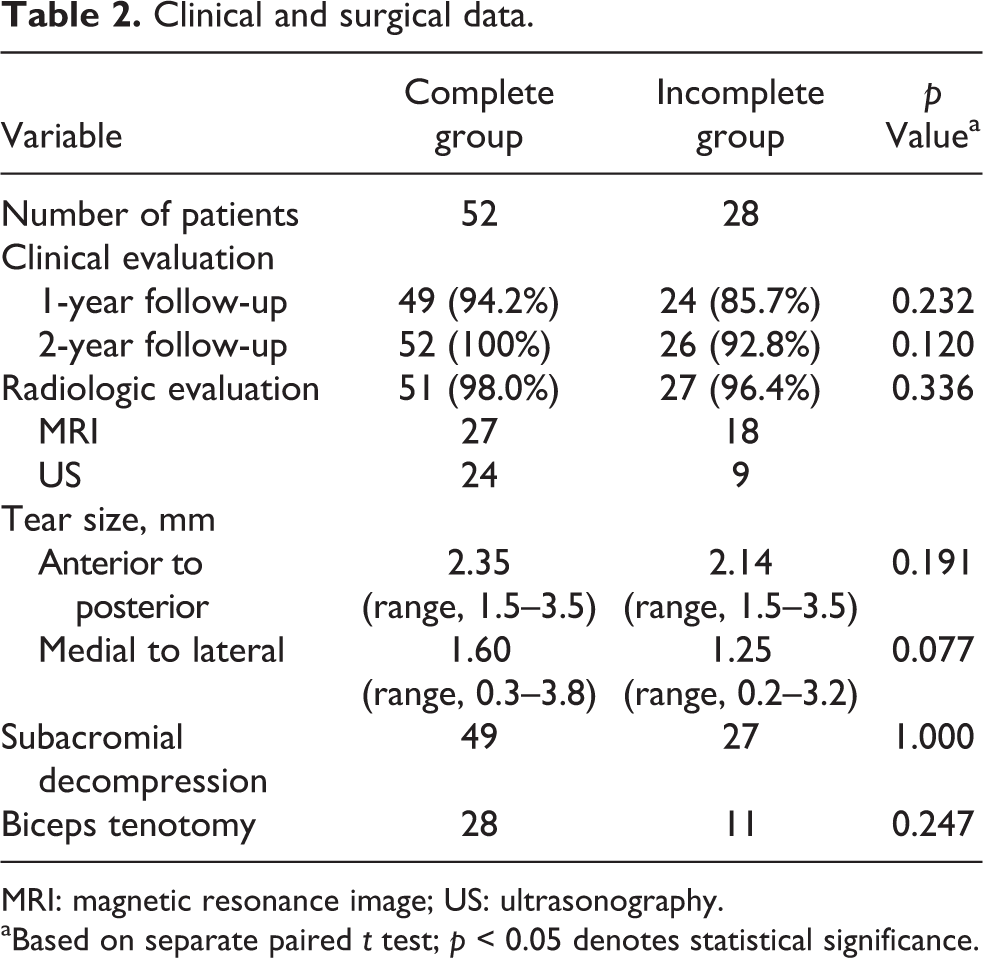
MRI: magnetic resonance image; US: ultrasonography.
aBased on separate paired t test; p < 0.05 denotes statistical significance.
Statistical analyses
The level of significance was set at p < 0.05. Comparisons between two groups were performed using the chi-square test and the independent samples t test for patient characteristics and the independent t test for preoperative tear size and pre- and postoperative ROM and ASES, UCLA, and VAS scores. The paired t test was used to compare ROM and ASES, UCLA, and VAS scores between the two groups at 1 year and 2 years after the operation. Power analysis was performed with α = 0.05 to evaluate powers of comparison tests (independent samples/paired t tests) for pre- and postoperative ROM, ASES, UCLA, and VAS scores. The sample sizes used for power calculations are different depending on the statistical methods or missing values. The smallest sample size is 24 for paired t tests at 1 year follow-up. The power of our study was estimated to be at least 0.95 for all the tests, which was statistically significant. These analyses were performed using SAS software (version 9.3; SAS Inc., Cary, North Carolina, USA).
Surgical technique and evaluation
All operations were performed by a single surgeon (K.C.K.) with the patient under general anesthesia and in the beach-chair position. The conventional suture-bridge repair method was developed by Park et al. 13 Under arthroscopy, the rotator cuff footprint was debrided. Depending on tear size, one- or two-suture anchors (4.5 or 5.5 mm, Bio-Corkscrew; Arthrex, Naples, Florida, USA) were placed in the medial row. Both limbs of each of the two sutures perforated the tendon medially to establish parallel horizontal mattress stitches for each medial anchor. Knot tying was performed for each mattress stitch. To establish the lateral row, a suture-bridge lateral-row repair technique was used to fully insert two knotless anchors (3.5 or 4.5 mm, Bio-PushLock; Arthrex) at an angle perpendicular to the cortical surface of the humerus (Figure 1). After completion of rotator cuff repair in the subacromial space, the repair state of articular-side rotator cuff was determined by glenohumeral joint examination through posterior portal using probe palpation through anterior portal. And then, patients were divided into two groups according to the repair state of articular-side rotator cuff after completion of bursal-side rotator cuff repair: complete and incomplete repair groups (Figure 2).

(a) Arthroscopic view shows a rotator cuff tear involving the supraspinatus. Two suture anchors were placed in the medial row. Sutures were passed through the reduced tendon in a mattress configuration. (b) The arthroscopic view from the lateral portal shows the completed repair of a rotator cuff tear with two PushLock (Arthrex, Naples, Florida, USA) anchors.

After completion of rotator cuff repair, the repair state of articular-side rotator cuff was determined by glenohumeral joint examination through posterior portal and using probe palpation through anterior portal. (a) Arthroscopic view of the complete repair group shows the footprint was completely covered by repaired rotator cuff. (b) Arthroscopic view of the incomplete repair group shows the footprint was incompletely covered by repaired rotator cuff (asterisk).
The maximum AP length of each rotator cuff tear was measured using a calibrated probe introduced through the anterior or posterior portal under arthroscopic observation from the posterolateral or lateral portal. The maximum mediolateral (ML) length of each tear was estimated on preoperative oblique coronal, T2-weighted MR images. We used MRI instead of arthroscopy to measure the ML length of each tear due to considerable changes in this dimension according to shoulder position, especially Abd (Table 1). All measurements were performed by the first author.
Postoperative management
All patients received standardized pre- and perioperative care at one hospital. The same regimen was prescribed to all patients, regardless of the repair state of articular-side rotator cuff. Postoperatively, we prescribed the use of a shoulder-immobilizing sling with an Abd pillow and provided instructions to maintain the shoulder at 30°–40° internal rotation and 20° Abd. The patients began gentle passive FF of the affected arm using the unaffected arm in the second postoperative week. The sling with the Abd pillow was removed weeks postoperatively and active ROM mobilization was started. Active-resistance muscle-strengthening exercises were started after 12 weeks using Thera-Band (HCM-Hygienic Corporation, Batu Gajah, Malaysia). At 3–4 months after surgery, the patients were permitted to perform light activities. Sports and heavy labor were allowed after 6 months.
Results
Of the 80 shoulders, 78 (97.5%) underwent MRI or US after 6 months postoperatively. Each follow-up rate at 1 year and 2 years after the operation was 91.3% (73 of 80 shoulders) and 97.5% (78 of 90 shoulders).
At 1 year follow-up, the average UCLA, ASES, and constant scores improved significantly to 31.86, 43.82, and 76.90, respectively, in the complete group and to 31.29, 45.25, and 75.71 in the incomplete group (Table 3). The UCLA, ASES, and Constant score improved in both groups after surgery (all ps < 0.001); however, there was no significant difference between the two groups at 1 year follow-up (p = 0.501, 0.783, and 0.748, respectively; Table 4). Additionally, both groups showed significant improvement in ROM after surgery (Table 3).
Comparison between the preoperative findings and postoperative clinical outcome at 1-year follow-up.

UCLA: Shoulder rating scale of the University of California at Los Angeles; ASES: American Shoulder and Elbow Surgeons score; VAS: Visual analog scale pain score.
aBased on separate paired t test; p < 0.05 denotes statistical significance.
Comparison of the clinical outcomes in the two groups at 1-year follow-up.
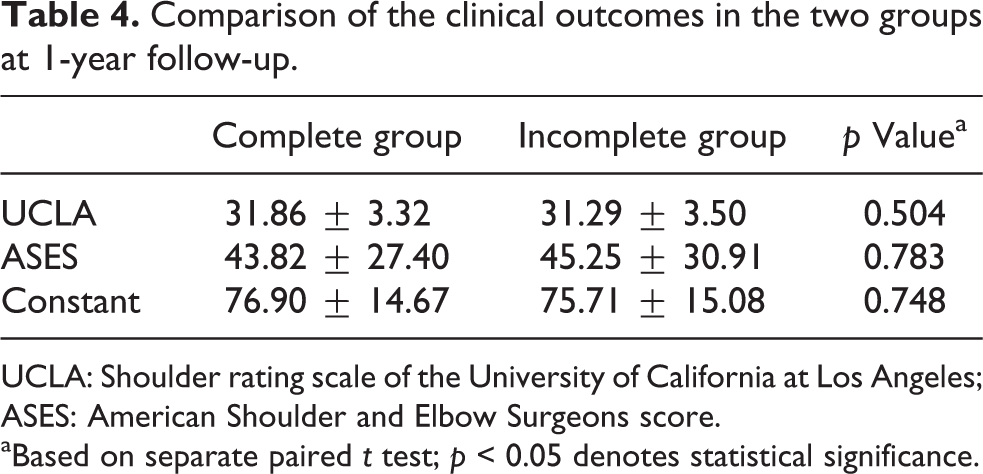
UCLA: Shoulder rating scale of the University of California at Los Angeles; ASES: American Shoulder and Elbow Surgeons score.
aBased on separate paired t test; p < 0.05 denotes statistical significance.
At 2 year follow-up, the average UCLA, ASES, and constant score improved significantly to 32.46, 87.94, and 79.69, respectively, in the complete group and to 32.50, 87.65, and 78.92 in the incomplete group (Table 5). The UCLA, ASES, and constant score improved in both groups after surgery (all ps < 0.001); however, there was no significant difference between the two groups at 2-year follow-up (p = 0.960, 0.921, and 0.796, respectively; Table 6). Additionally, both groups showed significant improvement in ROM after surgery (Table 5).
Comparison between the preoperative findings and postoperative clinical outcome at 2-year follow-up.

UCLA: Shoulder rating scale of the University of California at Los Angeles; ASES: American Shoulder and Elbow Surgeons score; VAS: Visual analog scale pain score.
aBased on separate paired t test; p < 0.05 denotes statistical significance.
Comparison of the clinical outcomes in the two groups at 2-year follow-up.

UCLA: Shoulder rating scale of the University of California at Los Angeles; ASES: American Shoulder and Elbow Surgeons score.
aBased on separate paired t test; p < 0.05 denotes statistical significance.
Overall re-tear rate of a repaired rotator cuff was 20.5% (16/78 shoulders). The re-tear rate was 13.7% (7/51 shoulders) for complete group and 33.3% (9/27 shoulders) for incomplete group; this difference was statistically significant (p = 0.041). No intra- or perioperative complication occurred, and no patient experienced neural injury, wound infection, or suture anchor problems.
Discussion
This study evaluates clinical and radiographic outcomes according to articular-side repair state after suture-bridge rotator cuff repair. We hypothesized that repair state of articular-side rotator cuff would have an effect on clinical outcomes and repair integrity after operation. Although there was no significant difference in functional outcomes at short-term follow-up, incomplete articular-side rotator cuff repair increased re-tear rate in full-thickness rotator cuff tears.
Arthroscopic rotator cuff repair is a common surgical procedure. Multiple factors have been shown to be associated with a less favorable outcome following rotator cuff repair, including age, sex, smoking status, larger tear size, poor tendon quality, fatty degeneration of cuff muscle, poor repair integrity, and repair technique. 2 –11 For age, sex, and smoking status, there were no statistical differences in this study. For tear size, tendon quality, and fatty degeneration of cuff muscle, we prospectively enrolled 80 consecutive shoulders with full-thickness rotator cuff tears (supraspinatus and/or infraspinatus) with narrow limitation for tear size (1.5–3.5 cm at anterior to posterior dimension). Although we were unable to assess preoperative muscle atrophy grades, we strictly limited tear size to reduce variability in postoperative outcomes due to differences in tendon quality and fatty degeneration of cuff muscle. Tear size both anterior to posterior and medial to lateral of two groups had no statistical differences in this study.
Biomechanical studies have shown that the double-row technique increased in initial fixation strength, minimal gap formation, and sufficient mechanical strength compared with single-row technique. Therefore, double-row technique may be beneficial in both clinical outcomes and repair integrity. Several studies reported comparisons of single-row and double-row techniques. Although postoperative radiographic evaluation showed significantly better tendon healing in the double-row group and more re-tears in the single-row group, clinical results did not show significant difference between the two groups. 14 In addition, biomechanical studies have shown that suture-bridge technique improved the biomechanics of rotator cuff repair constructs. 8 The mean pressurized contact area between the tendon and tuberosity insertion footprint with the suture-bridge technique was superior to that of the conventional double-row technique. 9,10 The suture-bridge technique has greater ultimate-to-load failure and less gap formation than the double-row technique. 9,10 This biomechanical superiority of the suture-bridge technique may contribute, at least in part, to the low structural failure of the repaired cuff. Although the biomechanical data and clinical advantages showed promise, postoperative MRI and US showed re-tear rates with no significant difference, and clinical results also did not show significant difference between two groups. 15
Although clinical results may not show significant difference among techniques, postoperative radiographic evaluation may show significantly difference in tendon healing based on the repair methods. Therefore, only the arthroscopic suture-bridge technique was used in this study, thereby reducing variability in postoperative outcomes due to differences in the surgical technique. There were no differences in frequency of biceps tenotomy or subacromial decompression. In addition, all operations were performed by a single shoulder surgeon in one hospital setting, thereby reducing variability in postoperative outcomes due to differences in the technical expertise of different surgeons.
It is important that medial anchor in suture-bridge technique should be placed at articular side margin. 13 The incomplete repair could be generated by incorrected location of medial anchor or gap formation because of loose tying of medial row. 10 In our study, the re-tear rate was 13.7% for complete group and 33.3% for incomplete group with statistically significant difference. However, no significant difference was observed in the short-term clinical results between two groups. Many studies have shown that pain and overall scores are comparable between re-tear and non-re-tear cohorts, but that if sufficiently powered and if subscales of strength and function are broken out, intact repairs have better outcomes. In addition, Mall et al. 16 found tear extension in 23% of patients in a longitudinal study using US for nonhealing rotator cuff tendons. This is especially important, given the evidence that full-thickness rotator cuff tears do not heal spontaneously. It has long been noted that rotator cuff tears retract and form adhesions, complicating surgical repair. Tendons deteriorate over time, often leaving only tissue-paper-quality tendons for repair. Fatty degeneration and muscle atrophy occur, with permanent changes likely in longstanding cuff tears. Therefore, mid- and long-term results will be necessary to compare the results between two groups.
The present study has some limitations. First, although all US evaluations were performed by an experienced musculoskeletal radiologist, this technique is examiner dependent. 17 However, we did not perform the US examination ourselves to avoid surgeon bias. 18 Second, although repair integrity was confirmed postoperatively, we did not analyze the effects of anatomical factors such as fatty degeneration of muscle or tendon quality on the outcome of rotator cuff repair. We were unable to assess preoperative muscle atrophy grades due to incomplete MRI scans, which lacked an appropriate Y-shaped view. Third, we could not compare the postoperative cuff integrity evaluation by the two radiologists to compare the reliability of US and MRI. Despite these limitations, the present study has several strengths. First, all operations were performed by a single shoulder surgeon in one hospital setting. Second, we restricted the size of full-thickness rotator cuff tears included in the study to an AP length of 1.5–3.5 cm. Third, although controversy has surrounded the long-term clinical outcomes following different rotator cuff repair methods or techniques, only the arthroscopic suture-bridge technique was used in this study. We believe that most small tears (<1 cm AP length) do not require suture-bridge or double-row repair. A recent systemic review found no significant difference in re-tear rates between single- and double-row repairs of tears <1 cm in length. 19
Conclusion
Regardless of the repair state of articular-side rotator cuff, the arthroscopic rotator cuff repair resulted in comparable functional outcomes between two groups at short-term follow-up. However, patients who repaired articular-side rotator cuff incompletely revealed higher re-tear rate after operation than those who repaired completely. Although no significant difference was observed in the short-term clinical results between two groups, mid- and long-term results will be necessary to compare the results between the two groups.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.