
Abstract
Background:
Arthroscopic surgery is becoming popular in the management of hip pathologies. There are numerous studies describing the outcomes of the treatment of athletes with this method. These outcomes are generally found to be excellent. Yet there are little data in the literature with respect to the arthroscopic treatment of nonathletes. The objective of our study is to compare the outcomes of the femoroacetabular impingement (FAI) treatment between athletes and nonathletes using arthroscopy, using two popular scales.
Methods:
The study involved a total of 129 male patients operated at our departments between 2009 and 2013. The subjects were divided into two groups: athletes and nonathletes. The results were assessed using the Nonarthritic Hip Score (NAHS) and Modified Harris Hip Score (MHHS). In addition, the length of postoperative hospitalization was evaluated.
Results:
Analyses revealed that athletes performed better in NAHS over each period under analysis (prior to the operation, 12 and 24 months after the operation). As regards MHHS in these periods, the results in both groups were comparable. In addition, it was found that the length of postoperative hospitalization was similar in athletes and nonathletes.
Conclusions:
Arthroscopic treatment of FAI is an effective method producing visible effects in athletes as well as nonathletes but quicker recovery in male athletic population. In the examined population, NAHS was a better measurement tool than MMHS, showing differences between the athlete and nonathlete population.
Introduction
The femoroacetabular impingement (FAI) concept was identified and described by Ganz. 1,2 According to his findings, FAI was a mechanical cause of the chronic hip pain. The theory of impingement was a breakthrough regarding explanation of etiology of the early idiopathic degenerative hip disease and labral or chondral abnormalities.
Initially, FAI was managed by the open method through the lateral approach, with excision of the greater trochanter, and surgical dislocation of the hip to gain full access to the femoral head and acetabulum. In 2007, Sussmann et al. compared FAI operation using the open technique and arthroscopy on a human corpse. Using computed tomography (CT), they proved that accuracy and precision of arthroscopy is higher than in the open technique. On the other hand, resection time was shorter when the open method was applied. 3 The mini-open technique (with a limited approach) is an optional method of the FAI treatment. It allows for osteoplasty without hip dislocation. As regards a new approach offered by Pierannunzii and d’Imporzano, firstly hip arthroscopy is conducted, where intra-articular injuries are evaluated and managed. Then, if necessary, hip osteotomy is performed through the anterior mini-open approach, which allows for exposure of the anterolateral portion of the head–neck junction. Their 2007 study revealed satisfactory results in eight out of eight patients treated with the mini-open technique. 4
The development of hip arthroscopy contributed to its wide-range application in the treatment of FAI. Initially, arthroscopy was only a limited open technique but its evolution and usage of the traction table resulted in its application in the treatment of central compartment pathologies and allowed for good joint evaluation.
In the recent decade, the indications for arthroscopy increased considerably. Nowadays, it is no longer limited to only athletes but seems to bring positive effects in the management of less physically active people.
There are numerous publications concerning the results of arthroscopic treatment among young and adult athletes, professionals and amateurs unvolved in a large number of sports, including baseball, polo, and soccer. 5 –15 Thus, arthroscopy has been widely used in the sports medicine. Yet a number of publications comparing FAI treatment effects in athletes and nonathletes are insufficient—only a small number of studies have been conducted on that issue. 16,17 Therefore, our work is aimed at demonstrating the effects of arthroscopic treatment of FAI in athletes and nonathletes in a larger comparable population. The purpose of this study was to compare the clinical results of athletes to those of nonathletes who underwent arthroscopic surgery for FAI. Our hypothesis was that better outcomes and quicker recovery were observed in the athletic population.
Material and methods
Of all the patients referred to our department for hip arthroscopy, patients with a history of systemic disorders, pediatric hip disorders, or significant hip trauma were excluded. We included patients with an FAI diagnosis confirmed by clinical and X-ray examination. In all the patients, FAI diagnosis was based on the interview, physical examination, and X-ray diagnostics. Interviewed patients reported limited hip mobility and mild pain at the end of the range of motion. Patients with clear symptoms of labral tears were also excluded from the study.
A total number of 129 patients (138 hips) were included in the study. The patients were divided into two groups: athletes (89 patients and 95 hips) and nonathletes (40 patients and 43 hips; Table 1). A minimum sport’s activity of 2 h three times a week was required to be included in the athlete group.
Sports activity by patients.
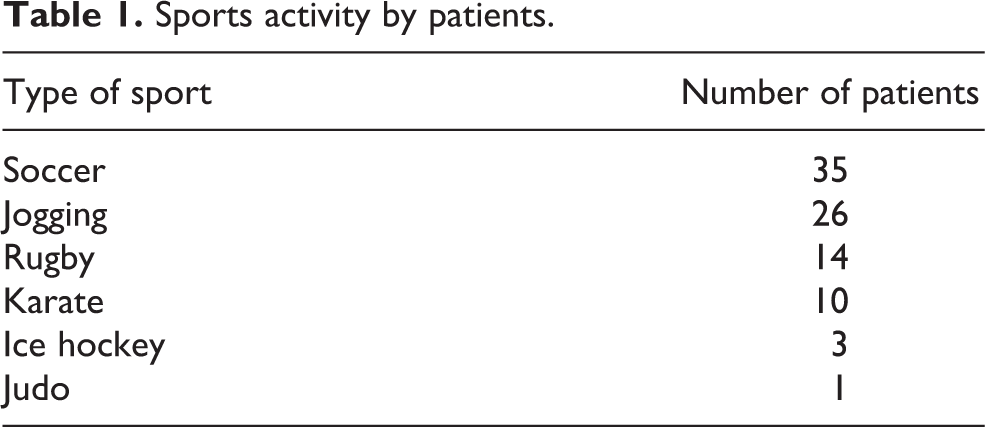
All patients were males. The mean age of athletes was 36.7 years (range: 18–52 years); standard deviation (SD) = 13.3 years. The mean age of nonathletes was 38.5 years (range: 26–78 years); SD = 14.4 years. Groups were demographically comparable without statistical differences. All the patients underwent arthroscopic surgery due to FAI, between August 2009 and August 2013.
After preoperative management, patients were positioned supine. Arthroscopy was performed through the anterolateral and then anterior portals in a standard fashion starting from the peripheral compartment. All surgeries were performed by the same surgeon (senior author). Osteoplasty of the cam and pincer impingement was performed using the spherical bone cutter.
Apart from FAI, five cases of labral degeneration and one case of osteoarthritis were diagnosed intraoperatively in athletes. In the nonathletes group, four cases of labral degeneration and three cases of osteoarthritis were diagnosed.
Labral degenerations were debrided with a shaver, taking care to retain the margin of the healthy labrum intact. No labral sutures were used. Exposed regions of the damaged cartilage were evaluated using the Outerbridge classification system, intraoperatively making on them a number of drill holes under arthroscopic and X-ray visualization.
Patients in both groups received low-molecular-weight heparin as an anticoagulant therapy for 10 days. They were recommended to use the operated limb during walking, with partial weight bearing as tolerated, which depended on the extent of surgery, damages of additional structures, general fitness, and muscular fitness of the operated limb. Patients were recommended to make use of continuous passive motion machines.
The study included evaluation of the hip arthroscopy using Modified Harris Hip Score (MHHS) and Nonarthritic Hip Score (NAHS) as well as postoperative hospitalization time. Patients were given MHHS and NAHS before the operation and 12 and 24 months after the surgery.
Statistically significant value was at p < 0.05, while statistically insignificant at p > 0.05. Analysis of variance (ANOVA) with repeated measures test was used for further analysis.
Results
A total of 129 patients aged between 18 and 58 years and mean age of 37.8 (SD = 15.3) were included in the study. The percentage of nonathletes included in the study was larger than that of athletes—69% and 31%, respectively.
Then the NAHS outcomes of athletes and nonathletes were compared as follows: prior to the treatment, 12 months after treatment, and 24 months after treatment. To do this, ANOVA tests were conducted. Table 2 shows the descriptive statistics obtained in those analyses. It was revealed that the athletes performed better in the NAHS test in each period under analysis (prior to the treatment, 12 months, and 24 months after treatment). Scores were statistically significant in each period (p < 0.05).
Descriptive statistics of NAHS for three measurement periods broken down by sports played by patients.

NAHS: Nonarthritic Hip Score; ANOVA: analysis of variance.
Then the MHHS outcomes were compared in athletes and nonathletes as follows: prior to the treatment, 12 months after treatment, and 24 months after treatment. To do this, ANOVA tests were conducted. Table 3 shows the descriptive statistics obtained in those analyses. It was revealed that the performance of athletes was similar to nonathletes in the MHHS test in each period under analysis (prior to the treatment, 6 months, and 12 months after treatment). Yet the scores were statistically insignificant in each period (p > 0.05). Athletes returned to their previous activities within 6 months after surgery (avg.: 3.3 months, range: 2.8–5.9 months).
Descriptive statistics of MHHS for three measurement periods broken down by sports played by patients.
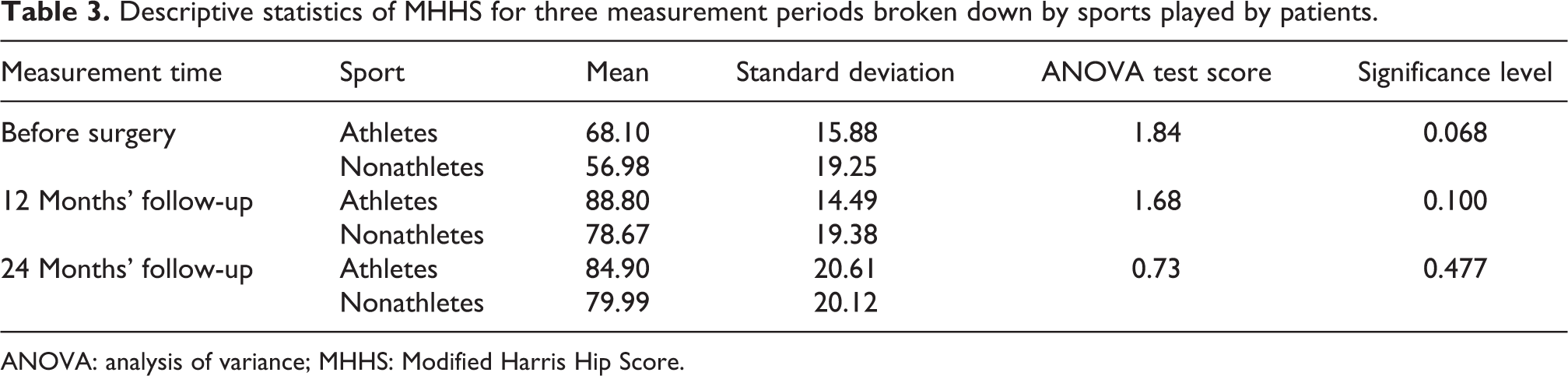
ANOVA: analysis of variance; MHHS: Modified Harris Hip Score.
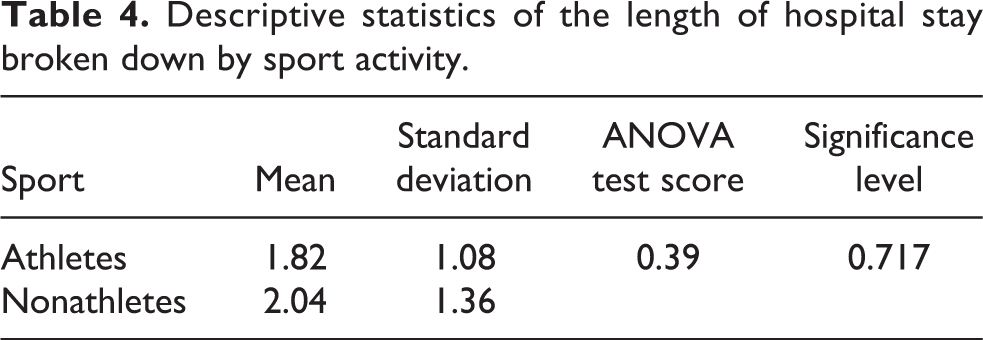
Then it was examined whether athletes and nonathletes were different in terms of the length of hospital stay. To do this, ANOVA tests were conducted. Table 4 shows the descriptive statistics obtained in those analyses. It was revealed that the length of hospital stay was similar in both athletes and nonathletes. Scores were also statistically insignificant (p > 0.05).
Descriptive statistics of the length of hospital stay broken down by sport activity.
Discussion
There are numerous scientific reports about the efficacy of the arthroscopic treatment of FAI. Briggs proved that conservative treatment is effective in only a small number of patients and the basic mode of FAI treatment is arthroscopy. 18 A large number of researchers discussed the outcomes of the treating athletes using other methods. All the available data suggest a huge success rate of arthroscopy. It is widely known that this method enables patients to recover physical fitness in a really short time. 5,6,8 –11,13,14 There are cases where concomitant osteoarthritis may either lengthen this time or even prevent athletes from returning to professional sport. 19 Philippon et al. proved that after arthroscopic treatment, 93% of athletes included in the study recovered the fitness level they demonstrated prior to the disease. 9
Thus, arthroscopic treatment may certainly be said to be a huge breakthrough in the FAI treatment. The objective of our study was to compare the outcomes of the FAI treatment between athletes and nonathletes (i.e. in both groups of patients) using arthroscopy.
There is no just one most reliable scale to evaluate FAI treatment because of nonavailability of direct comparisons of all applied scales. Researchers use a wide range of scales to evaluate patients with hip and groin pain or young and elderly patients. The rating scales for hip function that authors mention most frequently include NHHS, MHHS, Hip Outcome Score (HOS), Copenhagen Hip and Groin Outcome Score (HAGOS), International Hip Outcome Tool (iHOT-12), and Hip Sports Activity Scale (HSAS). Occasionally, a new rating scale for hip function is developed and applied in the case for which it is designed for.
To evaluate patients who received hip arthroscopy, we applied the rating scales that were also used in a large number of other studies—MHHS and NAHS. 10,16,17 In our opinion, they proved to be useful in the testing of a large number of hip pathologies, which was crucial for us. Moreover, both rating scales are recommended by the International Society for Hip Arthroscopy to evaluate the treatment outcomes of patients who received hip arthroscopy. The scales are frequently applied and their usefulness has been proved in a large number of studies. 7,10,16,17,20,21 Given the fact that our study included young, middle-aged, and elderly people (age range: 18–78 years), MHHS and NAHS were most useful. In our opinion, the possibility of applying these rating scales to population of various age groups is another advantage.
In 2011, Tijssen et al. conducted extensive studies on the usefulness of different rating scales after the arthroscopic treatment of the hip. NAHS was recommended to evaluate patients after hip arthroscopy and was found to provide the best quality evaluation. 22
According to other researchers, NAHS, compared with HAGOS and iHOT scales, is also reliable and precise in the identification of lesions in the hip. In addition, authors claim that NAHS has the smallest probability of error. 23
Thorborg et al. compared MHHS with iHOT and HOS using the COSMIN checklist. Their study revealed that iHOT scale meets only a few COSMIN parameters so its application in young patients with hip pain is questionable. According to Thorborg et al., the MHHS scale demonstrates better responsiveness parameter compared with their counterparts.
A study by Aprato et al. included 691 patients and was aimed to analyze the MHHS quality in the evaluation of patients after hip arthroscopy. 24 The authors proved that MHHS demonstrates correlation with patients’ satisfaction and provides reliability at the level of R = 0.451 for p < 0.001, sensitivity at the level of 73%, specificity at the level of 64%, and accuracy at the level of 71% over the first year after treatment. Moreover, they proved that despite certain limitations of the MHHS, there is a correlation between the level of patients’ satisfaction and the rating scale outcome. Thus, the authors confirmed the usefulness of MHHS in the evaluation of patients after hip arthroscopy. 24
As regards HAGOS and HSAS, they were not used here due to the specific parameters of the groups of patients involved in the study.
Thorborg et al. assessed the usefulness of HAGOS in terms of the COSMIN checklist. They recommended this scale for young and middle-aged patients with chronic hip and groin pain. 21 According to Naal et al., HSAS is designed for athletes with FAI, but further studies to assess its usefulness in young patients should be conducted. 25
There are limited data in the literature with respect to the evaluation of different groups of patients after the arthroscopic treatment of hip pathologies. Malviya et al. were among those few authors who compared groups of athletes and nonathletes after arthroscopic management of the hip. 7 They found that athletes recover faster over the first 6 weeks following the surgery. Similar outcomes are also observed 6 and 12 months later. Thus, over those periods there was no prevalence in any group. Noteworthy, however, the outcomes of MHHS and NAHS surveys conducted prior to the surgery were similar to the groups under study. There was no prevalence in the group of athletes.
In our study, the scores of nonathletes were considerably lower in both surveys conducted prior to the treatment. To sum up, their hip-associated ailments were larger and hip functionality was worse prior to the surgery, compared to athletes. The outcomes suggest that hip functionality improved in both groups after the arthroscopic treatment. Yet our study revealed a difference in group outcomes prior to the treatment, which makes it difficult to find definitely the group that showed great improvement after the operation. Our analysis shows explicitly that the outcome of arthroscopic management of hip pathologies is closely associated with the progress of hip disease prior to the treatment. This may indicate that early treatment may guarantee better results. Therefore, it is crucial to undertake treatment at early stages of the disease—just like in the case of athletes—to obtain excellent results. Any treatment undertaken at later stages of FAI will not produce such satisfactory outcomes. Consequently, athletes with higher scores in both rating scales prior to the treatment also had higher scores after the treatment.
The data and comparison of improvement rates in both groups under study indicate that, if the preoperative scoring was similar for both groups, the results in all periods would also be similar. In other words, the arthroscopic treatment of athletes and nonathletes would show similar improvement.
The study also included a review of the length of hospital stay, which proved to be similar in both groups. Presumably, the length of hospital stay after the arthroscopic treatment of FAI is comparable in athletes and nonathletes. This does not bring athletes advantage despite their considerably lower age and larger (at least theoretically) potential of tissue regeneration.
Conclusions
Our study showed that the arthroscopic treatment of FAI is an effective method with visible effects in athletes as well as nonathletes in 2 years of follow-up. Male athletic population performed significantly better in NAHS, in all periods studied. MHHS was more forgiving, and in our opinion was not suitable for assessment of the results in active population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.