
Abstract
Aim:
The aim of our study is to compare the improvement in clinical outcomes after conventional arthroscopic double-row rotator cuff repair and arthroscopic undersurface rotator cuff repair.
Method:
A consecutive series of 120 patients who underwent arthroscopic rotator cuff repair was analysed. Sixty-one patients underwent conventional double-row rotator cuff repair and 59 patients underwent undersurface rotator cuff repair. Several clinical outcomes, including numerical pain rating scale (NPRS), constant shoulder score (CSS), Oxford shoulder score (OSS) and University of California Los Angeles shoulder score (UCLASS), were prospectively recorded by a trained healthcare professional preoperatively and at 3, 6, 12 and 24 months after surgery.
Result:
Comparing both groups, there were no differences in age, gender and preoperative NPRS, CSS, OSS and UCLASS. However, the tear size was 0.7 ± 0.2 (95% confidence interval (CI) 0.3–1.1) cm larger in the conventional group (p = 0.002). There was no difference in the improvement of NPRS, CSS, OSS and UCLASS at all time points of follow–up, that is, at 3, 6, 12 and 24 months after surgery. The duration of operation was shorter by 35 ± 3 (95% CI 28–42) min in the undersurface group (p < 0.001).
Conclusion:
Both arthroscopic undersurface rotator cuff repair and conventional arthroscopic double-row rotator cuff repair showed marked improvements in clinical scores when compared preoperatively, and there was no difference in improvements between both groups. Arthroscopic undersurface rotator cuff repair is a faster technique compared to the conventional arthroscopic double-row rotator cuff repair.
Introduction
Arthroscopic double-row rotator cuff repair has been a commonly performed technique for rotator cuff repair. As part of a conventional repair, most surgeons perform subacromial arthroscopy, sometimes followed by acromioplasty and debridement of the subacromial bursa. This is frequently done before performing the rotator cuff repair to free up more subacromial space, to allow a better view of the torn edges of the rotator cuff and its footprint and to make the rotator cuff repair easier.
Because there is evidence in the literature 1,2 that performing subacromial arthroscopy, together with its associated procedures described earlier, does not reduce the rate of tendon re-tear and does not change the clinical outcomes of rotator cuff repair, some surgeons avoid performing such procedures.
Arthroscopic undersurface rotator cuff repair is a recent innovation in rotator cuff repair. Murrell devised a novel method of rotator cuff repair, which is called ‘undersurface repair’. 3 –5 In a nutshell, the undersurface rotator cuff repair is performed with the arthroscope solely in the glenohumeral space, with no subacromial arthroscopy performed, thus the repair is viewed solely from the ‘undersurface’ of the rotator cuff, rather than the subacromial space, or the bursal side of the rotator cuff. It is a single-row repair that is not performed commonly, as it is a new technique with limited literature comparing the results of the conventional arthroscopic rotator cuff repair and arthroscopic undersurface rotator cuff repair. These are all from the group who devised the arthroscopic undersurface rotator cuff repair. 4 Their study was a retrospective study comparing rotator cuff repair from the undersurface of the rotator cuff and rotator cuff repair from the bursal side of the rotator cuff. They showed that the average operative time was significantly shorter for the undersurface rotator cuff repair group. Their study also showed that at 2 years both groups of patients had less pain with overhead activities, less shoulder stiffness, lower frequency of pain during activity or sleep and increased range of motion when compared preoperatively. Comparing both groups, there was no significant difference between both groups at 2-year follow-up. However, their comparison was between conventional arthroscopic single-row rotator cuff repair (performed from the bursal side) and arthroscopic undersurface rotator cuff repair.
The aim of our study is to compare the improvement in clinical outcomes after conventional arthroscopic double-row rotator cuff repair and arthroscopic undersurface rotator cuff repair.
We hypothesize that there is no difference in clinical outcomes between conventional arthroscopic double-row rotator cuff repair and arthroscopic undersurface rotator cuff repair.
Methods
Ethical approval for our study was obtained from our institution’s centralized institutional review board. Our study design is a retrospective temporal cohort-controlled study using prospectively collected data. Two groups of patients were compared: one that had a conventional arthroscopic double-row rotator cuff repair (conventional group) and one that had an arthroscopic undersurface rotator cuff repair (undersurface group). The two groups were temporal cohorts. In May 2012, we started to adopt the arthroscopic undersurface rotator cuff repair as the preferred method of rotator cuff repair. Prior to May 2012, the conventional arthroscopic double-row rotator cuff repair was routinely performed at our institution. All patients who underwent arthroscopic rotator cuff repair by a fellowship-trained sports surgeon were evaluated over the study period of 4 years, that is, the conventional arthroscopic double-row rotator cuff repair performed routinely in the first 2 years and the arthroscopic undersurface rotator cuff repair performed routinely in the next 2 years.
The inclusion criteria for our study were all patients with small- and medium-sized supraspinatus tears who had an arthroscopic rotator cuff repair performed by the senior author. The exclusion criteria for our study were patients who underwent an isolated subscapularis repair, had a large or massive supraspinatus tear, or had a partial thickness supraspinatus tear. Patients who had a concomitant fracture in the same limb or previous surgery of the same shoulder were also excluded from our study as the results will be confounded.
Both surgeries were performed by making the patients sit in the beach chair position under general anaesthesia, with standard posterior, anterior and lateral arthroscopic portals inserted in a similar fashion. A standard posterior portal was used for evaluating the glenohumeral joint. For the conventional rotator cuff repair, the posterior arthroscope was subsequently redirected into the subacromial space and the supraspinatus tendon was visualized from its bursal side. The subacromial bursa and the undersurface of the acromion were then debrided to allow visualization of the torn supraspinatus tendon from the bursal side, but no formal acromioplasty was performed. The edge of the torn rotator cuff tendon and footprint of the rotator cuff tendon on the greater tuberosity were then debrided using an arthroscopic shaver. Conventional rotator cuff repair was then performed in a suture bridge configuration using Healix suture anchors (DePuy Synthes Mitek, Raynham, Massachusetts, USA) for the medial row and Versalok suture anchor (DePuy Synthes Mitek) for the lateral row.
The undersurface rotator cuff repair technique was previously described by Murrell and associates in great detail 3,5 and thus would only be mentioned in brief here. The same standard posterior portal was used for evaluating the glenohumeral joint as with the conventional rotator cuff repair. This posterior portal allows visualization of the torn rotator cuff from the undersurface of the torn rotator cuff. The arthroscope was maintained in the glenohumeral joint throughout the whole surgery. A spinal needle was used to determine the position of the lateral portal. The main considerations were to allow for easy deployment of the suture-passing device across the torn edge of the rotator cuff, and at the same time, to allow the suture anchors to be placed at 90° to the footprint of the rotator cuff tendon on the greater tuberosity. The edge of the torn rotator cuff tendon and the footprint of the rotator cuff tendon on the greater tuberosity were debrided using an arthroscopic shaver as performed in the conventional group. Undersurface rotator cuff repair was performed using the Opus Smart Stitch Suture Device (Arthrocare Corporation, Sydney, Australia) and the Opus Magnum suture anchors (Arthrocare Corporation).
Both groups were subjected to the same post-operative rehabilitation protocol. During the first 4 weeks, the affected upper extremity was placed in a sling with only passive mobilization allowed in the pain-free range. At 4 weeks post-operatively, active assisted range of motion was allowed in the pain-free range and full passive range of motion was allowed with light isometric exercises. From 6 weeks post-operatively onwards, gradual increase to full active mobilization was allowed, encouraging dynamic stabilization exercises.
All patients who underwent rotator cuff repair surgery in our institution were assessed by a trained healthcare professional blinded to the surgical procedure performed at our orthopaedic diagnostic centre preoperatively and also post-operatively at 3, 6, 12 and 24 months. The assessment included several parameters such as numerical pain rating scale (NPRS), constant shoulder score (CSS), 6,7 Oxford shoulder score (OSS) 8,9 and University of California, Los Angeles shoulder score (UCLASS). 10 The length of operation was recorded in the operation notes after the surgery, which also included whether any concurrent biceps tenotomy or tenodesis was performed.
The primary outcome measures were patient-determined shoulder pain and function scores, specifically the CSS. The secondary outcome measures were length of operation.
Power analysis was done prior to the conduct of our study, based on the difference in improvement of CSS at 24-month follow-up. The minimal clinically important difference in CSS was reported to be 10 points. 11 To detect a difference of ten points in CSS improvement from a baseline mean score of 33 with a standard deviation of 16 at a power of 0.80, a sample size of at least 42 patients in each group would be required. This calculation was done for a two-sided test with a type I error of 0.05. Including all patients who underwent arthroscopic rotator cuff repair by a fellowship-trained sports surgeon between May 2010 and April 2014, we had 61 patients in the conventional group and 59 patients in the undersurface group.
We then carried out the statistical analysis using SPSS® 19.0 (IBM, Armonk, New York, USA). Statistical significance, in accordance with convention, was defined as a p value of less than 0.05. The Student’s unpaired t test was used for quantitative variables (age, body mass index (BMI), tear size and duration of surgery), while the Fisher’s exact test was used for categorical variables (gender, side of surgery and biceps procedures including tenodesis and tenotomy). To limit the confounding effect of patient’s age, BMI, gender, tear size and biceps procedures including tenodesis and tenotomy that can influence functional outcome scores, we used multiple linear regression analysis to adjust the preoperative score and improvement of score at 3, 6, 12 and 24 months’ follow-up observed for the two groups. This adjustment effectively accounted for any differences in the distribution of these covariates and their respective influences on the functional outcome scores within each of the two groups.
Results
A consecutive series of 120 patients who underwent arthroscopic rotator cuff repair by a fellowship-trained sports surgeon was evaluated. Sixty-one patients underwent conventional arthroscopic double-row rotator cuff repair (conventional group) and 59 patients underwent arthroscopic undersurface rotator cuff repair (undersurface group). There was an 11% lost to follow-up rate at 24 months, comprising seven patients from the conventional group and six patients from the undersurface group. Their scores at the latest follow-up were comparable to the others at the same time point.
There was no significant difference in age, BMI, gender and side of surgery between the two groups. However, the tear size was 0.7 ± 0.2 (95% confidence interval (CI) 0.3–1.1) cm larger in the conventional group (p = 0.002). The proportion of patients who underwent biceps tenodesis or tenotomy was comparable between the two groups (Table 1).
Patients’ demographics and operative factors.

The preoperative NPRS, CSS, OSS and UCLASS were comparable between the two groups. There was also no significant difference in the improvement of NPRS, CSS, OSS and UCLASS at all time points of follow-up, that is, at 3, 6, 12 and 24 months after surgery (Table 2). The duration of operation was shorter by 35 ± 3 (95% CI 28–42) min in the undersurface group (p < 0.001; Table 1).
Functional outcome scores (95% CI).
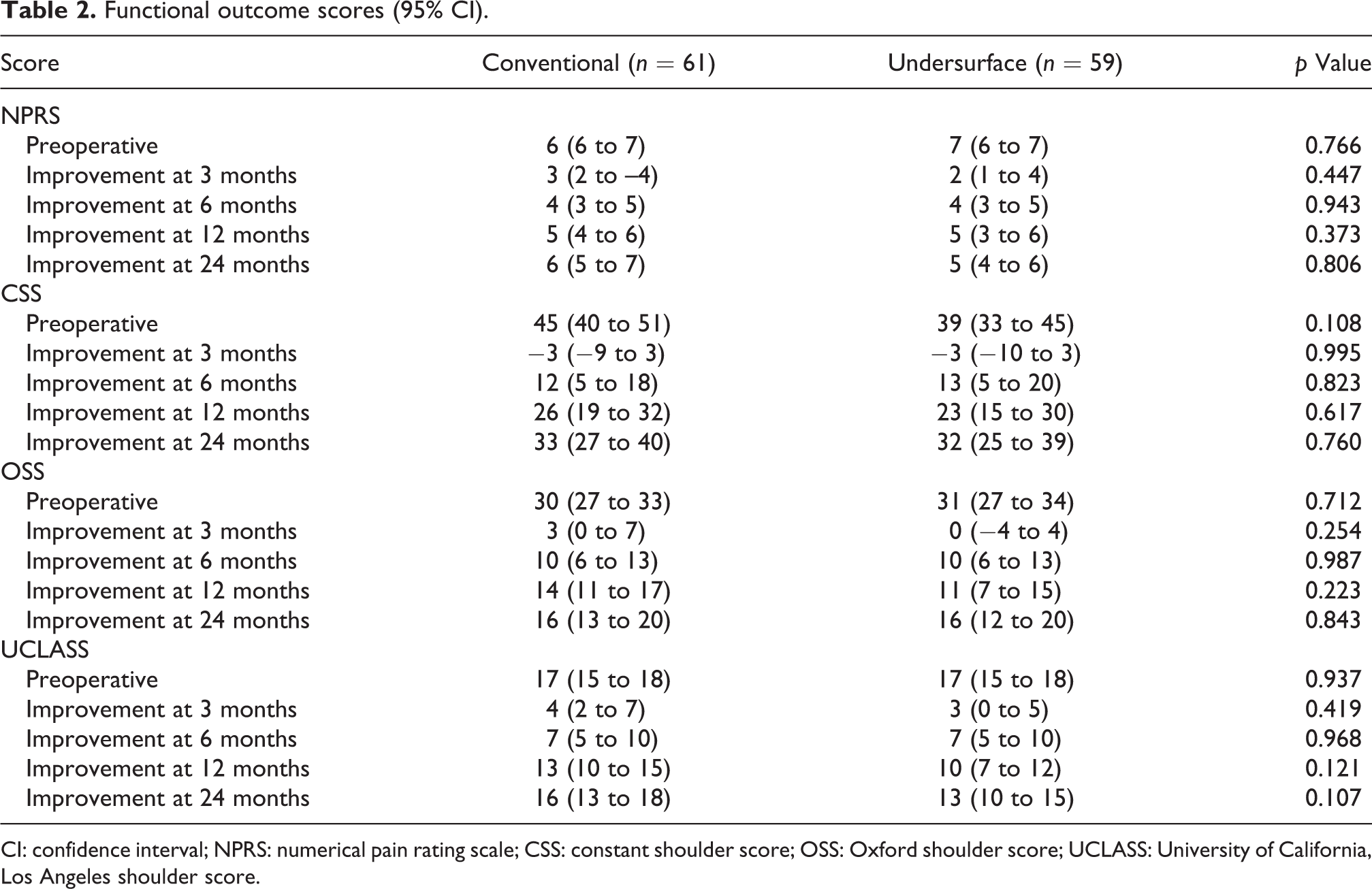
CI: confidence interval; NPRS: numerical pain rating scale; CSS: constant shoulder score; OSS: Oxford shoulder score; UCLASS: University of California, Los Angeles shoulder score.
Discussion
In terms of clinical outcome, both groups showed significant improvements in NPRS, CSS, OSS and UCLASS compared to preoperation. Among those with validated minimal clinically important difference (MCID), the improvements were all higher than the MCID of 10.0 for CSS 11 and 6.0 for OSS 12 at 6, 12 and 24 months after surgery.
However, there was no difference in the improvement magnitude of the absolute scores between both groups. The other published studies 3 –5 compared the results based on a shoulder service questionnaire and not the validated scores that we used in our study.
Our study showed that there is a shorter operative time in performing the arthroscopic undersurface rotator cuff compared to the conventional arthroscopic double-row rotator cuff repair. This is similar to the other published studies on undersurface rotator cuff repair, which showed a shorter operative time for the arthroscopic undersurface rotator cuff repair compared to the conventional arthroscopic bursal-sided rotator cuff repair. 3 –5 The use of a single-row repair and the omission of subacromial arthroscopy and decompression are contributory factors to the shorter operative time for the undersurface rotator cuff repair.
A theoretical advantage of the undersurface rotator cuff repair is that there is less interruption to the blood supply of the torn rotator cuff if all the soft tissues on the bursal side are not stripped off the rotator cuff. This would theoretically lead to better healing of the rotator cuff tear. However, there is a need for basic science studies on the blood supply of the rotator cuff after undersurface rotator cuff repair to prove this.
Limitations of our study include the lack of post-operative imaging studies to monitor for re-tear rates. This was also a non-randomized study, and the two groups were temporal, thus there is a potential for selection bias. Another limitation of our study is the different tear sizes of both groups. However, multiple linear regression analysis was used to reduce the confounding effect of the difference in tear sizes. Based on our study, we recommend that patients with small- to medium-sized supraspinatus tears may be considered for arthroscopic undersurface rotator cuff repair.
Conclusion
Both arthroscopic undersurface rotator cuff repair and conventional arthroscopic double-row rotator cuff repair showed marked improvements in clinical scores when compared preoperatively, and there was no difference in improvements between both the groups. Arthroscopic undersurface rotator cuff repair is a quicker technique compared to the conventional arthroscopic double-row rotator cuff repair.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.