
Abstract
Introduction:
Chronic lateral ankle instability occurs in up to 20% of ankle injuries. Most can be treated conservatively, but surgical reconstruction is required if conservative treatment fails. Modified Broström–Gould procedure is an effective surgical treatment and the augmentation of this procedure with a periosteal flap may confer additional stability. We report on the outcome of a technique combining a modified Broström–Gould procedure augmented with a periosteal flap in patients with chronic lateral ankle instability.
Method:
Twenty-four males aged 18–42 (mean, 24) with chronic lateral ankle instability affecting 24 ankles underwent the modified Broström–Gould procedure augmented with a periosteal flap, and these surgeries were performed by a single surgeon. The mean follow-up period was 28.7 months. Patients were assessed pre- and post-operatively with the American Orthopaedic Foot and Ankle Society (AOFAS) ankle and hind foot score.
Results:
Preoperatively, the mean AOFAS ankle and hind foot score was 67.38. Post-operatively, significant improvement was seen, with a score of 88.71 (p < 0.05). None of the patients reported surgical or wound complications.
Conclusion:
The technique of modified Broström–Gould procedure with periosteal flap augmentation appears to be a simple and safe operation for chronic lateral ankle instability. Patients with poor quality local ligamentous tissue, obese patients or high demand athletes generally benefit from this procedure. It allows effective augmentation of the reconstruction without causing any harm to local tendons or using additional costly implants.
Introduction
Injuries to the lateral ligamentous complex of the ankle are common, especially in the younger age group that are actively involved in sports. 1 –3 Most of these injuries improve with conservative management and physiotherapy, but up to 20% of patients develop symptoms of chronic ankle instability. 4 –7 Chronic instability occurs as a result of healing of the torn ligament with weak fibrous tissue or, in an elongated state, proprioceptive deficit or peroneal muscle weakness. 8 –10
Surgery is indicated when conservative management fails. A variety of surgical techniques have been described for chronic lateral ankle instability, which can be broadly classified into two groups, anatomic and non-anatomic reconstructions.
In the anatomic reconstruction, local tissue is used for reconstruction as in the Brostrom technique which involves shortening and imbricating the damaged elongated lateral ankle ligaments. 11 This technique was further modified by Gould in 1980 by mobilizing the ankle’s inferior extensor retinaculum and suturing it to the distal fibular over the ligamentous repair, reinforcing the repair and limiting inversion. 12
The non-anatomic reconstruction uses tissue grafts harvested at a distance to reconstruct the disrupted ligaments. Examples include the Evans, Chrisman-Snook and the Watson-Jones procedures. 13 –15
The anatomic reconstructions such as the modified Broström–Gould procedure are generally the preferred method of reconstruction. They restore anatomy, preserve ankle and subtalar motion and joint mechanics and maintain normal gait as compared to the non-anatomic procedures. 16 However, a point to note is that although the end-to-end repair of the ruptured ankle ligaments maintains feasibility for up to a few years after the initial injury, subsequent healing with fibrous tissue or gradual lengthening of the reconstructed ligaments over time results in insufficiency. 17
Glas et al. originally described a method of reconstructing the lateral ankle ligaments using a flap of periosteum taken off the fibula proximally and reflecting distally, thereby providing reinforcement to the anterior talo-fibular ligament (ATFL). 18
We believe that by combining these two techniques, where a modified Broström–Gould procedure followed by further reinforcement of the reconstruction with a periosteal flap from the distal fibula, further stability can be given to the reconstruction. This study reports on the outcome of a modified technique combining a modified Broström–Gould procedure augmented with a periosteal flap in patients with chronic lateral ankle instability.
Materials and methods
The records of 24 patients who underwent the modified Broström–Gould procedure augmented with a periosteal flap for chronic lateral ankle instability by a single surgeon at the hospital were retrieved. The data were prospectively collected and a retrospective review of the data was performed. Patients included in the study were all skeletally mature patients with a history of an initial traumatic inversion injury of the ankle followed by repeated ankle sprains thereafter. Indications for surgery were based on the patient’s symptoms of persistent pain or instability and clinical examination such as local tenderness over the anterolateral aspect of the affected ankle as well as a positive anterior drawer test or a positive talus tilt test when compared to the normal contralateral ankle. They also must have had at least 3 months of physiotherapy which failed to achieve a satisfactory functional outcome. The exclusion criteria were a history of ankle fracture, previous ankle surgery and generalized ligamentous laxity. All surgeries were performed by the same surgeon who used a consistent technique.
Under general or regional anaesthesia, the patient was placed in a lateral decubitus position with a tourniquet placed on the affected leg. A 4–5 cm curvilinear incision was made about 5 mm distal to the distal fibular tip extending across the body of the ATFL (Figure 1). This allows both exposure to the ATFL and access to create the periosteal flap from the distal fibula. Care was taken not to damage the sural nerve and the dorsal intermediate cutaneous nerve. After reflection of the subcutaneous tissue, a rectangular periosteal flap, measuring about 3 cm × 1 m, was surface marked on the distal fibula in an oblique direction so that it could cover the ATFL repair when reflected down (Figure 2). The periosteal flap was then elevated from proximal to distal, but it remained attached to the fibula distally (Figure 3). The inferior extensor retinaculum was dissected from the underlying capsule and ligaments and the intra-capsular ATFL was incised, exposing the ankle joint, and a mid-body section of the ligament was then removed (Figure 4). At the same time, the joint can also be inspected for the presence of any osteochondral injury of the talus. With the ankle held in a slightly dorsiflexed and everted position, the ATFL was repaired with non-absorbable Ethibond 2-0 (Ethicon; Johnson and Johnson, Cincinnati, Ohio, USA). Following this, the inferior extensor retinaculum was identified, mobilized, and imbricated with Ethibond 2-0 sutures superficial to the repair (Figure 5). The periosteal flap was then flipped distally so that it covered the repair and secured at its two distal edges by mattress sutures using Ethibond 2-0 non-absorbable sutures (Figure 6). Gentle anterior drawer test was then performed to ensure ankle stability. The tourniquet was then deflated, haemostasis was obtained and the wound was copiously irrigated and closed.

Skin incision.

Surface marking of the periosteal flap and incision over anterior talo-fibular ligament (ATFL).

Dissection of the periosteal flap over the distal fibula.

Incision over the anterior talo-fibular ligament (ATFL).

Repair of the anterior talo-fibular ligament (ATFL) and imbrication of the inferior extensor retinaculum.
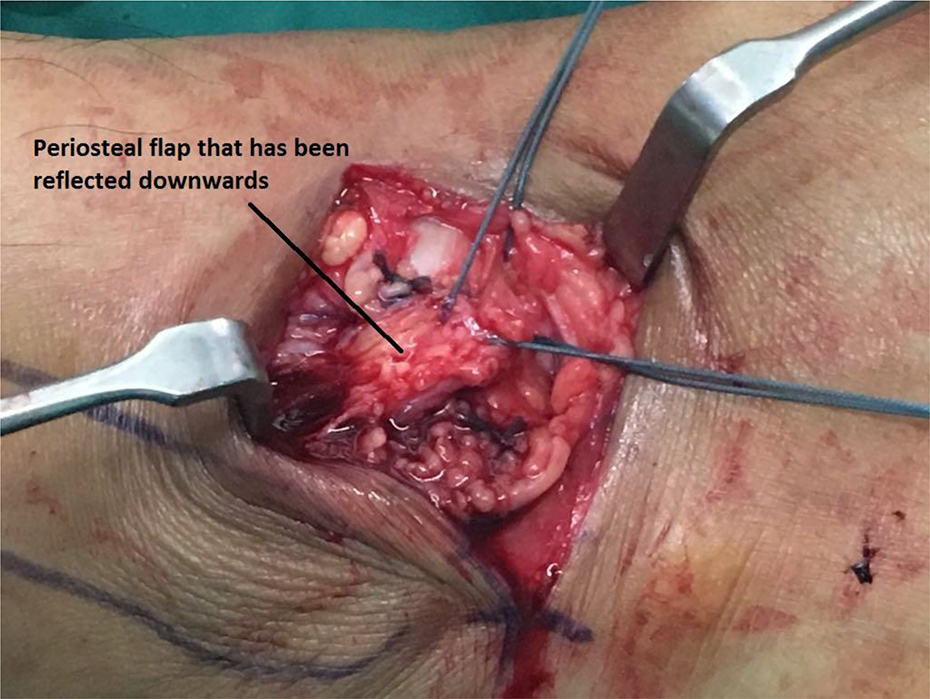
Reflection of the periosteal flap over the repair.
Post-operatively, the ankle was immobilized in a well-padded cast, in a neutral position with slight eversion and the patient was kept nonweight bearing. After 2 weeks, the cast was taken off and the stitches removed. The ankle was then placed in a long walking boot (Aircast, Summit, NJ, USA) for 6 weeks and the patient was allowed to bear weight as tolerated while the walking boot was on. The patient was also started on a physiotherapy regime consisting of ankle and subtalar range of motion exercises, peroneal muscle strengthening and proprioceptive training via balance board training. After 3 months, return to sports was allowed with the use of ankle braces for at least another 6 months.
Outcome was assessed using the American Orthopaedic Foot and Ankle Society (AOFAS) ankle and hind foot score pre- and post-operatively. The AOFAS ankle–hind foot score is a clinical rating system developed by Kitaoka et al. 19 It combines subjective scores of pain and function provided by the patient. This was coupled with objective scores based on the surgeon’s physical examination of the patient, assessing the sagittal motion, the hind foot motion, the ankle–hind foot stability and the alignment of the ankle–hind foot. The AOFAS ankle–hind foot scale is scored with a possible maximum of 100 points.
Data analysis comparing the pre- and post-operative AOFAS ankle–hind foot scores was done using IBM SPSS Statistics version 23 (IBM Corp, Armonk, NY, USA). Paired t test was used to analyse the data. A p value of <0.05 was taken to be statistically significant. Ethical approval was granted by the hospital’s institutional review board.
Results
The average age of the 24 patients at the time of presentation was 24.13 (range 18–42) years. The study group was exclusively male. Majority of the patients, 15 (62.5%), sustained injury while playing sports, 7 (29.18%) during sedentary activity, 1 (4.16%) had direct trauma to the ankle during work and 1 (4.16%) was involved in a motor vehicle accident. Intraoperatively, 13 (54.17%) of the patients were found to have complete tear of the ATFL; while in the remainder, the ATFL was attenuated. The mean follow-up duration was 28.7 months. The mean (standard deviation) preoperative AOFAS ankle and hind foot score was 67.38 (± 4.44). Post-operatively, significant improvements in the AOFAS ankle and hind foot scores was seen with a mean score (standard deviation) of 88.71 (± 10.49) (p<0.0001; Table 1). No patients had any wound complications. There were neither recurrence of instability nor was there any need for a revision surgery at the 24-month follow-up.
Patient demographics and pre- and post-operative AOFAS hind foot scores.
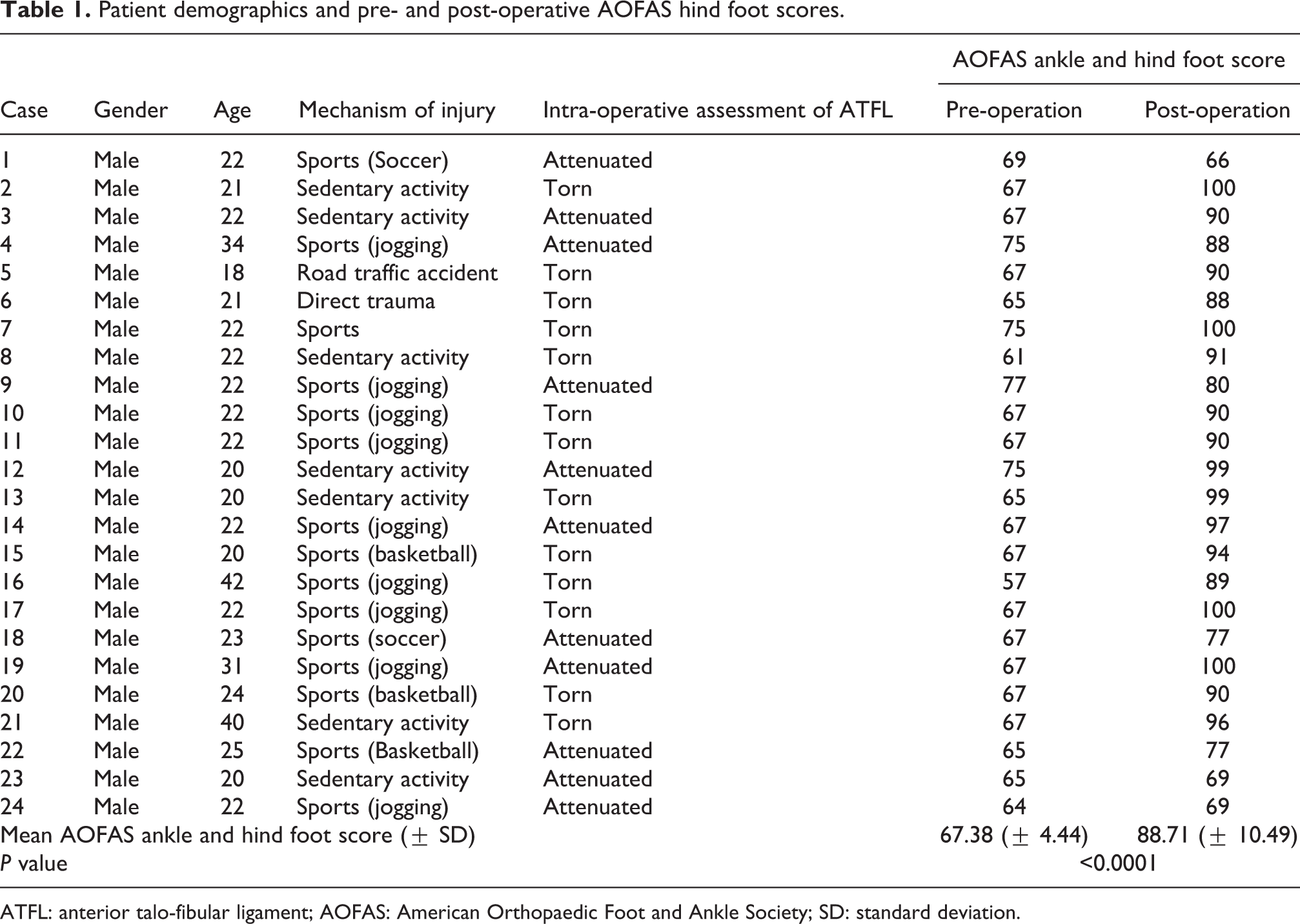
ATFL: anterior talo-fibular ligament; AOFAS: American Orthopaedic Foot and Ankle Society; SD: standard deviation.
Discussion
Currently, there are a myriad surgical procedures described for chronic ankle instability. These can be divided into anatomic or non-anatomic reconstructions. Non-anatomic reconstructions do not repair or recreate the native anatomy of the lateral ligament complex. Instead, they use local tissue or tendon to reconstruct the incompetent native ligamentous complex. Common non-anatomic reconstructive procedures such as the Evans, Chrisman-Snook and the Watson-Jones tenodesis have consistently reported 80–85% good to excellent results. 11,20,21 However, they have their disadvantages. These include sacrificing normal anatomical structures, eversion weakness, abnormal ankle and subtalar joint kinematics, increased hind foot stiffness and higher surgical complication rates such as wound infection and sural nerve injury. 11,20,22,23 Hence, these procedures tend to be used more commonly in revision cases.
Anatomic reconstructions, where the native anatomy of the lateral ligamentous complex is repaired or recreated, are preferred by the majority of surgeons whenever possible. They address the underlying pathology, resulting in almost normal biomechanics of the ankle and subtalar joint. 16 The modified Broström–Gould procedure with reported success rates of nearly 90% continues to be the gold standard for anatomic reconstructions. 10,12,24,25 However, some studies reported that the modified Broström–Gould procedure may stretch out and fail over time, especially in overweight individuals or highly active sportsmen with higher than usual functional demands. 21,26,27 Hence, this has led to the development of various augmentation techniques to supplement the reconstruction, including the use of suture anchors, 28,29 part of the peroneus brevis tendon 27 or periosteal flaps from the distal fibula. 30
The advantages of a periosteal flap as an augmentation technique compared to suture anchors or tendon grafts are that it is relatively simple to harvest the flap, it needs only a small 5cm incision and it does not require any costly special devices or implants. It does not cause harm to any local tendon and it is also anatomic with resultant close to normal ankle and subtalar kinematics. 31 A periosteal flap has also shown good biomechanical strength. Bohnsack et al. reported on the biomechanical properties of various autogenous transplants commonly used for the reconstruction of lateral ankle ligaments. He found no significant difference in the biomechanical stability between periosteal flap and the ATFL. 32 Furthermore, periosteal tissue serves as a scaffold for the formation of fibroblastic tissue and subsequent transformation into ligament. At 12 months’ follow-up after the use of a periosteal flap for ankle ligament reconstruction, histological analysis of the reconstructed ligament showed longitudinally aligned collagen fibres with spindle-shaped nuclei suggesting a transformation of periosteum to ligamentous tissue. 31
Periosteal flap augmentation therefore becomes a good adjunct procedure especially in cases where the quality of the torn lateral ankle ligaments to be repaired is poor, such as those with recurrent ankle sprains or in obese or high-demand athletes with higher than usual functional demands. 26,27,31,33
In our study, the post-operative AOFAS mean (standard deviation) scores at 28.7 months’ follow-up was 88.71 (± 10.49). This result compares well with studies of other tenodesis or suture anchor augmented anatomic reconstructive procedures. Hua et al. using a suture anchor augmented technique reported mean AOFAS scores of 86.5 in 87 ankles at 29 months’ follow-up. 34 Yong et al. reported on 15 patients who underwent a peroneus brevis augmentation of anatomic reconstruction. Mean AOFAS scores at 13.6-month follow-up was 91.5. 35 Hence, using our modified technique, we were able to achieve similar scores, yet at the same time, not having to resort to the use of additional costly implants or harvest any local tendons that may alter ankle and subtalar joint biomechanics.
Our study was not without its limitations. Firstly, this was a retrospective study of a technique of lateral ankle reconstruction and not a randomized-controlled trial. To further validate the efficacy of this technique, future randomized-controlled trials comparing the modified Broström–Gould procedure with the modified Broström–Gould procedure with periosteal flap augmentation may be warranted. Secondly, it was assumed that the 24 patients included in this study can be considered sufficiently large enough to draw a meaningful interpretation. Thirdly, we do note that there is some controversy over whether AOFAS scores are the best way to determine the outcome following ankle instability surgery. 11 However, recent studies on lateral ankle instability tend to use the AOFAS scoring systems, and it does provide a good indication of patients’ symptoms and functional level in their everyday activities.
In conclusion, our modified technique of the modified Broström–Gould procedure with periosteal flap augmentation appears to be a simple and safe operation for chronic lateral ankle instability, especially in those with poor quality local ligamentous tissue, obese patients or high-demand athletes. It allows effective augmentation of the reconstruction without causing harm to local tendons or using additional costly implants.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.