
Abstract
Objective:
This study was designed to define fracture lines and comminution zones in OTA/AO 23C3 distal radius fractures from axial computed tomography (CT) images that would influence surgical planning, development of new classifications, and possible implant designs.
Methods:
Thirty-four consecutive OTA/AO 23C3 fractures treated by a single surgeon between January 2014 and December 2014 were analyzed. For each fracture, maps of the fracture lines and zones of comminution were drawn. Each map was digitized and graphically superimposed to create a compilation of fracture lines and zones of comminution. Based on this compilation, major and minor fracture lines were identified and fracture patterns were defined.
Results:
All major fracture lines were distributed in the central region of the radius distal articular surface. There is a recurrent fracture pattern with a comminution zone including the scaphoid and lunate fossa; Lister’s tubercle; and ulnar, volar, and radial zones.
Conclusion:
It is important for the practicing surgeon to understand these four main fragments. Knowledge of this constant pattern should influence the development of new classifications and possible implant designs.
Introduction
Assessment and management of distal radius fractures have been aided by two widely used classification systems: the Orthopaedic Trauma Association/Arbeitsgemeinschaft für Osteosynthesefragen (OTA/AO) classification system 1 and Fernandez classification system. 2 These classification systems describe the types of injuries, but they may be limited in their ability to provide accurate and consistent information about the actual fracture morphology. Of these, the OTA/AO type 23C3 is the most complex type of distal radius fracture, indicating extensive injury to the radiocarpal and distal radioulnar joint surfaces of the distal radius. This complexity is due to the comminution at the metaphyseal and articular surfaces and due to the vulnerable soft tissue envelope of the wrist. 3 OTA/AO classification 3 divides distal radius fractures into type A (extra articular), type B (partial articular), and type C (complete articular), but does not address fracture lines or their vectors. The Fernandez classification system is based on the mechanism of injury as bending, compression, shearing, avulsion, and combination of former mechanisms. 2 This classification system also does not address articular fracture lines or their vectors.
Detailed identification of OTA/AO type 23C3 distal radius fracture patterns and comminution zones may help to facilitate surgical planning, new classification systems, and perhaps implant designs.
With the limited available knowledge about anatomic patterns of articular comminution in OTA/AO type 23C3 distal radius fractures, we aimed to create a map of fracture lines from CT examinations of the distal radius fractures. Goals of this study were determined as (1) mapping the common fracture lines and (2) mapping the most common zones of comminution.
Materials and methods
Between January 2014 and December 2014, 34 consecutive fractures were recruited retrospectively. For each patient, CT scans and two standard radiograph views (Antero-posterior [AP] and lateral) of the wrist were obtained after provisional closed reduction and circular casting. The aim of the provisional closed reduction and circular casting was to provide bony relationship as possible. Inclusion criteria were a closed OTA/AO type 23C3 distal radius fracture (age > 18 years) and availability of radiographic and CT images. Patients were excluded if they had an open fracture, wrist or hand surgery history, any contraindication to casting like edema or poor skin conditions, and an articular step off greater than 3 mm after provisional reduction. The methodology for this study was adapted from a previously described evaluation of pilon fractures. 4
A technique of fracture mapping was used for this study. 4 A brief description follows: After provisional closed reduction and casting, all patients received radiograph examination and a CT scan (Figure 1). The CT axial cut, which was perpendicular to the longitudinal axis of the radius, was located 3 mm above the distal radius subchondral surface from each of the 34 patients selected for fracture mapping. The 3-mm measurement was recorded from the ulno-carpal joint subchondral surface that allowed for an analysis of all relevant fragments involving distal radius articular surface. Suitability of 3-mm cuts was verified in three OTA/AO type 23C3 fractures included in the pilot study.

Preoperative axial computed tomography (CT) scan of a distal radius fracture 3 mm above the articular surface. Note the (1) dorsal, (2) radial, (3) volar, and (4) ulnar fracture fragments.
Each image was taken digitally and subsequently enlarged to fit a grid to standardize the size of the images, which were then uploaded into the graphic design program Adobe Illustrator CC software® (Adobe Systems Incorporated, San Jose, CA, USA).
Individual maps of all fractures were drawn first. Subsequently, all 34 individual maps were superimposed to create a fracture line map for identifying common fracture patterns (Figure 2). Superimposed images resulted in a frequency diagram based on the density of fracture lines. The integrity and continuity of anatomic landmarks (Lister’s tubercle, radial styloid, sigmoid notch, and volar cortex) were matched for proper alignment and rotation. In addition, the variability of radius size and shape was standardized with a 4 × 4-cell grid oriented to the ulnar margin of the radius.

All fracture lines of all 34 superimposed fractures.
Areas of comminution were transcribed from each cross section of the radius to a computerized 4 × 4 grid. Areas with fracture fragments less than 5 mm in diameter and gaps between fragments were defined as comminution zones. The 5-mm measurement was chosen according to previously demonstrated depth of the radius, which ranges from 14 to 20 mm. 5 A 1-cm diameter selection in a pilon map study 4 did not seem appropriate when applied to the distal radius.
Two different sets of computer image files were created and stored in the graphic design program: one fracture line map and one comminution zone map (Figures 2 to 4).
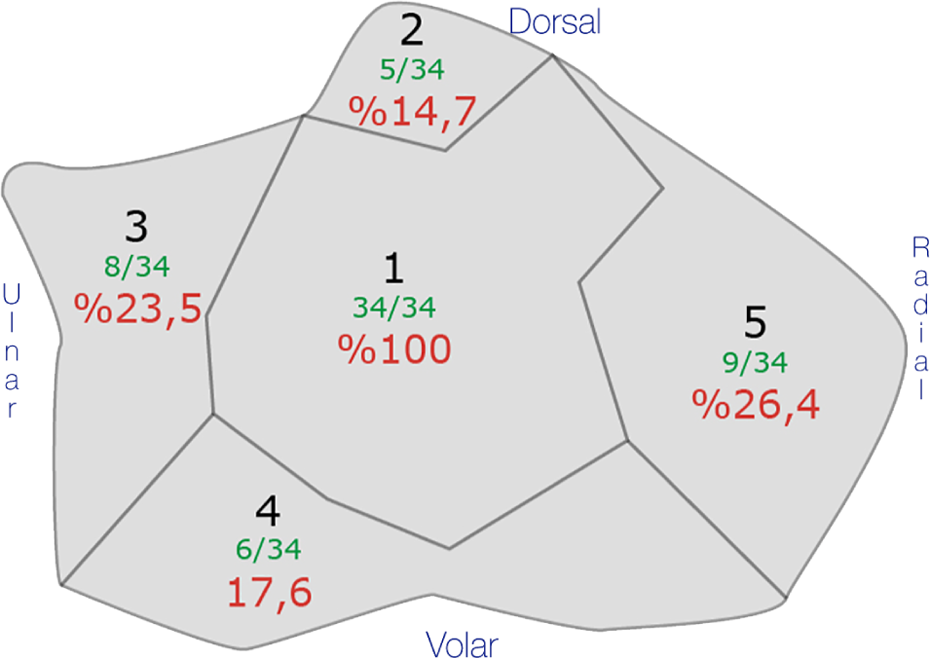
Distribution of fracture lines on the distal radius articular surface. One major fracture corridor and four minor peripheral zones are described. Black numbers indicate zones, green numbers indicate count of fractures, and red numbers indicate proportions of fracture lines.

The comminution zone map of OTA/AO type 23C3 distal radius fractures. The major zone of comminution was located in the middle of the articular surface with proximity to the dorsal cortex. Minor comminution zones occurred around the major comminution zone. The intensity of white represents the frequency of the fracture line occurrence.
To create a comminution zone map, we applied a white fill effect on the black floor of each comminution zone. The transparency level was inversely proportional to opacity. A layer’s opacity determines to what degree it obscures or reveals the layer beneath it. A transparency level of 5% was applied to each layer, which represented one fracture, so that the comminution zone of each fracture layer had a dark gray color resulting in an increased intensity to white color when multiple fracture lines overlapped. In this way, a frequency diagram based on the density of zones of comminution was created. The senior author and an experienced graphic designer performed all mapping processes using a mouse. All fracture line interpretations were verified by a fellowship-trained hand surgeon and an experienced graphic designer. Verification was based on every single case and the created maps. A fellowship trained hand surgeon visually verified all layers and maps. A graphic designer verified all layers and maps with numerical data on the program. In addition, axial, coronal, and sagittal sections were investigated to evaluate fracture lines proximal or distal to the watershed line.
All analyses were descriptive. Patient characteristics were summarized as mean and SD or proportions. Separate maps were prepared and visually compared for differences.
Results
Mean patient age was 56 years (range, 39–72). Twenty-three patients (67%) were male, and 11 patients (33%) were female. The injury mechanisms included falls onto an outstretched hand while walking on snowy ground in 8 patients (24%) and high-energy injuries like a motorcycle accident in 26 patients (76%).
All fractures were OTA/AO type 23C3. In 13 fractures (38%), there was an extension to the radial diaphysis. According to the Fernandez classification, 26 patients (76%) had type 5 fractures, and 8 patients (24%) had type 3 fractures.
After a double review of all the images, consistent fracture lines were identified and deemed as “major fracture lines.” Specifically, in all patients, major fracture lines had located in a corridor that was in the central region of the radiocarpal joint with a dorsoradial extension (Figure 4). Twenty-three percent of all fracture lines entered into the distal radioulnar joint. Four main fragments existed in every case. All other fracture lines, which were not seen in every fracture, located outside of the major fracture line corridor were named “minor fracture lines.” Minor fracture lines did not always occur and were more variable when they were present. According to the fracture map that was formed by major and minor fracture lines, five different fracture areas were determined as (1) central area (involving scaphoid and lunate fossa with proximity to dorsal cortex), (2) Lister’s tubercle area, (3) ulnar area (involving distal radioulnar joint surface and dorsal cortex), (4) volar area, and (5) radial area (involving scaphoid fossa, radial cortex, radial styloid, and radial side of the dorsal cortex). Distribution of fracture lines is summarized in Figure 5.

Comminution zones according to major and minor fracture line frequency. Zone “1” depicts major comminution zone that was located in the middle of distal radiocarpal articular surface; zones “2” to “5” depict the minor comminution zones. Intensity of white represents the frequency of occurrence.
One major zone of comminution was present, which occurred with the greatest frequency and size. This major zone of comminution was included in the scaphoid and lunate fossa of the distal radiocarpal joint with proximity to the dorsal cortex.
Discussion
In this study, an identified fracture mapping technique 4 was applied to a series of complex distal radius fractures. Our analysis identified five recurrent patterns in OTA/AO type 23C3 fractures: (1) a zone of comminution including the central articular surface with proximity to dorsal cortex, (2) Lister’s tubercle fragment, (3) ulnar fragment including the distal radioulnar joint surface, medial cortex, and dorsal and ulnar cortex, (4) volar fragment, and (5) radial fragment including the radial cortex, radial styloid, and dorsal cortex.
Classic distal radius fracture classification systems have limited reliability and cannot perfectly guide the surgical approach and fixation technique. 6 –8 The definition of complex distal radius fractures with the use of features that were presented in this study may be more reliable than conventional classification systems.
Comminuted distal radius fractures require great understanding for optimal preoperative planning, surgical exposure, and proper fixation method. 9 Knowledge of fracture patterns in the distal radius may be helpful.
The OTA/AO classification system is based on whether the articular surface is fractured, the number of fracture lines involving the articular surface (one vs multiple), and the degree of comminution in the metaphyseal region, whereas the Fernandez classification system is based on the mechanism of injury (bending, shearing, compression, avulsion, and combined). The Melone fracture classification system is based on articular joint surface involvement of the distal radius. 10 According to this classification system, four fragments were described as (1) shaft, (2) radial styloid, (3) the dorsal medial fragment, and (4) volar medial fragment. However, in standard radiographs, compliance and accuracy of the Melone classification have not been confirmed with clinical trials. In addition, many intra-articular fractures can only be included into two groups due to medial articular facet emphasis. The OTA/AO and Fernandez classification systems are the most widely used classifications in clinical practice but neither of these classification systems can address fracture lines. 1,2
Our aim was not to establish a new subclassification system; however, mapped patterns in this study may help to develop a more relevant classification system based on real fracture patterns and comminution zones.
In comminuted distal radius fractures, dorsal cortical comminution is more prominent. 11 Volar cortical durability, relatively less comminution, good soft tissue coverage, and less complication rates are advantageous during the internal fixation of distal radius fractures with volar approach. 12,13
In fractures involving the intermediate and lateral column, it is important to provide equal fixation to the scaphoid and lunate facets. 14 In a biomechanical study with AO 23C3 type fractures, loss of fixation in dorsal ulnar side of the distal fragment was first observed. They concluded that stable fixation of distal fragments significantly increased total stability. 15 In our study, all fracture lines and comminution zones were involved in the radial and intermediate columns. Major fracture line corridor, the zone of highest density of fracture density, was involved in the scaphoid and lunate fossa. The force transmitted through the carpal bones, the volar/radial inclination of the distal radius, and the lesser durability of the dorsal cortex may cause the formation of the main fracture line and formation of a corridor. Also, force distribution differences at the ligament attachment sites and cortical bone between these attachment sites may contribute to development and distribution of major fracture lines. Future biomechanical and radiologic studies are needed for objective assessment of this issue.
Our study has some similarities with a published study, 16 which was not a formal study that used an image technique, and it described five distinct fracture types as (1) intra-articular fracture with displaced dorsal fragment, (2) dorsal split with dorsal dislocation, (3) palmar split with palmar dislocation, (4) complex distal radius fractures with metaphyseal separation, and (5) destruction of the articular surface. Our methodology focuses on the articular surface and detail patterns of four fracture fragments and one comminution zone that are useful in daily routine in the management of comminuted distal radius fractures. All 34 fractures in our study matched with these five types of fracture patterns.
All fracture lines were distal to the “watershed line” in our study. This was established by reviewing the axial, coronal, and sagittal CT images in every fracture determined by cross-linking. Proximal extension of fractures was measured to a maximum of 3.6 cm in the sagittal plane and 3.2 cm in the coronal plane. Therefore, to treat the majority of these fractures with implants, which could be placed proximal to the watershed line, fragments distal to the watershed line could be fixed with angled screws.
The most common location of comminution included the central articular surface involving both the scaphoid and lunate fossa with proximity to the dorsal cortex. This central comminution may be explained by the axial forces commonly seen on most of the distal radius fractures, whereas proximity to the dorsal cortex resulted from impact on the carpus, volar inclination of the distal radius, and a relatively thin dorsal cortex.
Historically, women have higher incidence of distal radial fracture across all adult age groups. 17 In our study, there was a predominance of male patients. This may be related to the high-energy injury mechanism seen in most of the male patients.
Based on our comminution map and current literature knowledge, it would seem that only the dorsal approach allows direct visualization of the central comminution, but offers a biomechanically less stable construct and includes implant related complications. The volar approach combined with the fixation technique, combined volar and dorsal approach, or the fragment specific fixation with individualized approaches may offer adequate access to common comminution zones and provide biomechanically more stable construct. In this context, modified or combined approaches may be developed to optimize ideal placement of reduction instruments and implants.
There are some limitations and strengths of this study. A major limitation was the qualitative manner of assessment methods. Also, fractures involved heterogenous patient group including high and low energy injuries. Theoretically the fracture pattern may be different in low and high energy injuries. A relatively small number of patients, qualitative assessment of the frequency map with visual appearance, two-dimensional (2-D) identification of a three-dimensional deformity, and lack of analysis of the rotational positions of the fracture fragments were the other limitations. In addition, position of the fracture lines would vary if the fracture lines were oblique in the axial plane. We set up CT cuts according to anatomical reference points to provide reproducibility and uniformity. An additional amount of noise in the heat mapping technique might have obscured the actual data. Future studies are warranted to investigate the validity and accuracy of this technique.
Constructing a durable image on surgeons’ mind with revealed maps is a major strength. This creates easier preoperative planning and surgical prediction expectancy. This is the first study identifying fracture line and comminution zone distribution of OTA/AO type 23C3 fractures, which are the most troublesome distal radius fractures on the distal radius articular surface. Findings of this study may be insufficient in preoperative planning. For a complete preoperative planning, a thorough review of all 2-D CT images and/or traction radiographs is recommended.
Previously, two mapping studies including the distal radius were published. 18,19 According to those studies, articular fractures of the distal radius were statistically more likely to occur between the ligament attachments. This is related to maximum tension of the ligaments at the extremes of motion. The ligaments transmit this tension to the radius, while the bone directly adjacent to the ligament does not receive the tensile forces. The bone fails at this interface, between the ligament attachments. It is different in high energy injuries where the fracture patterns are more complex. In our study, more fracture lines were observed between ligamentous attachment areas. The reasons may be that our cases included are mainly high energy trauma. Thus, the energy dissipation at the distal radius in high energy fractures is different from a relatively low energy fractures. The previous studies focused on only osseous fragments, injury mechanisms, two part intra-articular fractures, 18 and heterogenous types of intra-articular distal radius fractures. 19 Our study focused on only OTA/AO type 23C3 distal radius fractures.
In conclusion, constructed maps from this study of 34 patients with OTA/AO type 23C3 distal radius fracture suggest that there are repeatable fracture patterns.
This data may be helpful in drawing a roadmap for ideal diagnostic approaches, hardware placement, and optimum implant designs in the treatment of comminuted distal radius fractures. In addition, the same data may be useful for the development of new classification systems or subclassifications of existing classification systems. Commonly observed fracture patterns and comminution zones create opportunity for development of optimized diagnostic and therapeutic protocols in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.