
Abstract
Purpose:
To assess the anatomic path of the middle sacral artery (MSA) at the presacral area and its relationship to the spinal midline during an axial lumbar interbody fusion (AxiaLif) approach.
Methods:
Fifty human cadavers (25 males, 25 females) were used in this study. A transabdominal approach was used to expose the anterior aspect of the L5/S1 intervertebral disc and the presacral space. We measured the size and distance from the spinal midline at the following positions: (a) middle of the L5/S1 disc level, (b) 1 cm below the sacral promontory (SP), and (c) 2 cm below the SP. Each parameter was measured three times by two observers, and the mean value analyzed.
Results:
The MSA was present and originated from the left common iliac artery in all cadavers with a mean width of 2.14 mm. The position of the MSA in relation to the midline was most commonly on the left side (LS, 56%) followed by the right side (RS, 34%) and midline (ML, 10%). In the LS group, the distance from the midline is relatively constant in the three measured positions with a mean value of (a) 1.78 mm (range, 0–8.17 mm), (b) 2.08 mm (range, 0–7.10 mm), and (c) 2.06 mm (range, 0–9.76 mm). In the RS group, the distance from the midline increased from cephalad to caudad, with a mean value of (a) 1.44 mm (range, 0–9.64 mm), (b) 2.19 mm (range, 0–9.95 mm), and (c) 2.92 mm (range, 0–10.03 mm).
Conclusions:
Our study found the presacral anatomic path of the MSA was most commonly at the left of midline. In addition, the right-sided MSA variant had increasing distance from the midline along its anatomic path from cephalad to caudad. Our findings suggest an AxiaLif approach at the left of midline may place the MSA at greatest risk.
Introduction
Axial lumbar interbody fusion (AxiaLif) has gained in popularity as a minimally invasive spinal surgery. 1,2 AxiaLif is a procedure used to fuse L4-5 and L5-S1 under fluoroscopic C-arm guidance without direct visualization of the lumbosacral spine. The implant is inserted from a small incision near the tip of the coccyx through the presacral potential space to the anterior aspect of S1 with a starting point near the sacral promontory (SP). Vascular structures in the presacral space below the SP are at risk of injury during the implant insertion procedure (Figure 1). A recent meta-analysis reported the AxiaLif complication rate of 12.9%, with 14.4% requiring reoperation. 3 Lindley and colleagues also reported the AxiaLif complication rate of 26.5%, but noted a 2.9% rate of pelvic hematoma. 4 During the anterior lumbosacral surgery, the middle sacral artery (MSA) is an important structure at risk of bleeding, if injured. 4 –6 Previous studies described the variable course of the MSA but focused on the anatomic course at or above the SP. 6 –10 There has been limited anatomic evaluation of the MSA in the presacral area as a structure at risk during the AxiaLif approach. 6 Therefore, we set out to evaluate the anatomic pathway of the MSA and its relation to the spinal midline at the presacral area during an AxiaLif approach.

AxiaLif approach [lateral view (1(a)), AP view (1(b))] and its relation to MSA. MSA: middle sacral artery; AxiaLif: axial lumbar interbody fusion.
Methods
We used 25 male and 25 female fresh-frozen cadavers from Chulalongkorn Cadaver Training Center. All donated specimens were of Thai racial origin and did not have a history of abdominal or spinal surgery. The cadavers were stored at −25°C, which were then thawed at room temperature prior to dissection and study measurements. The texture and softness of cadavers were evaluated before dissection. We performed a transabdominal approach and carefully exposed the anterior aspect of the L5/S1 intervertebral disc and the presacral space.
The following parameters were analyzed or measured using metric calipers (Figure 2), with each measurement repeated three times by two independent observers, and the mean value analyzed. level of the aortic bifurcation; position of the MSA (center, left, or right of midline variants); width of the MSA at mid-height of L5/S1 disc level; distance from the spinal midline to the MSA, with the midline identified as the midpoint between the lateral aspects of L5/S1 disc, and measurement was done at three positions: the middle of the L5/S1 disc level, 1 cm below the SP, and 2 cm below the SP; and anterior L5-S1 disc height at midline.

Photograph (2(a)) and drawing picture (2(b)) showing MSA and measured parameters [level of aortic bifurcation (a); emerging point of MSA (b); width of the MSA at mid-height of L5/S1 disc level (c); position of the MSA (center, left, or right position related to midline; d); distance from the spinal midline to the MSA, at the middle of the L5/S1 disc level (e), at 1 cm below the SP (f), and at 2 cm below the sacral promontory (g); and L5-S1 disc height at midline (h)]. SP: sacral promontory; MSA: middle sacral artery.
Statistical analysis
Mean ± standard deviation and median (minimum and maximum) were calculated for descriptive data. Unpaired t test was used to compare the variables between male and female. A p value of less than 0.05 was considered to be statistically significant.
Results
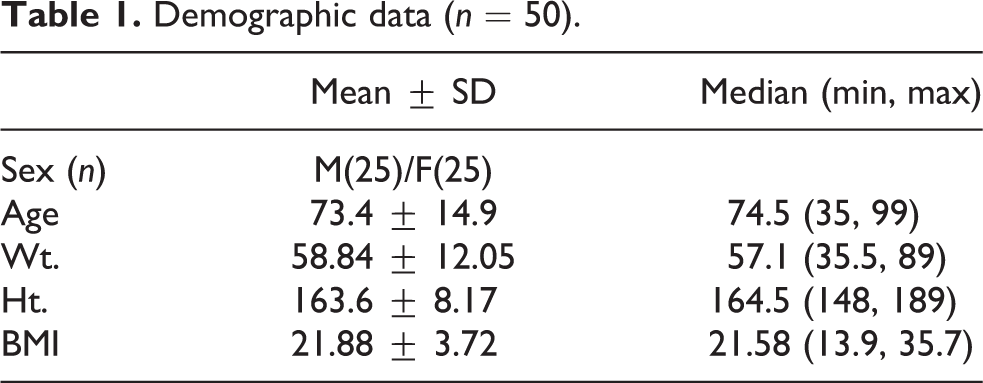
The demographic data of cadaveric specimens are outlined in Table 1. In this study, the MSA was found in 100% of specimens, and all originated from the dorsomedial aspect of the left common iliac artery (CIA), averaging 2.10 mm (range, 1.13–3.18 mm) in width at the mid-height of L5/S1 disc level. The level of aortic bifurcation was L4 body = 5 (10%), L4/L5 disc = 25 (50%), and L5 body = 20 (40%). The average height of the L5/S1 anterior disc at midline was 19.14 mm (range, 0–26.55 mm).
Demographic data (n = 50).
Analysis of distance from the midline (Table 2) found the MSA was midline in 5 (10%) of 50 cadavers. The MSA was at the left of midline in 28 of (56%) 50 cadavers, with a median of 1.78 mm (range, 0–8.17 mm) left of midline at the mid-height of L5/S1 disc, 2.08 mm (range, 0–7.10 mm) at 1 cm below the SP, and 2.06 mm (range, 0–9.76 mm) at 2 cm below the SP. The MSA was at the right of midline in 17/50 cadavers (34%), with a median of 1.44 mm (range, 0–9.64 mm) right of midline at the mid-height of L5/S1 disc, 2.19 mm (range, 0–9.95 mm) at 1 cm below the SP, and 2.92 mm (range, 0–10.03 mm) at 2 cm below the SP.
Analysis of distance from the midline in millimeters (total = 50).

SP: sacral promontory; SD: standard deviation.
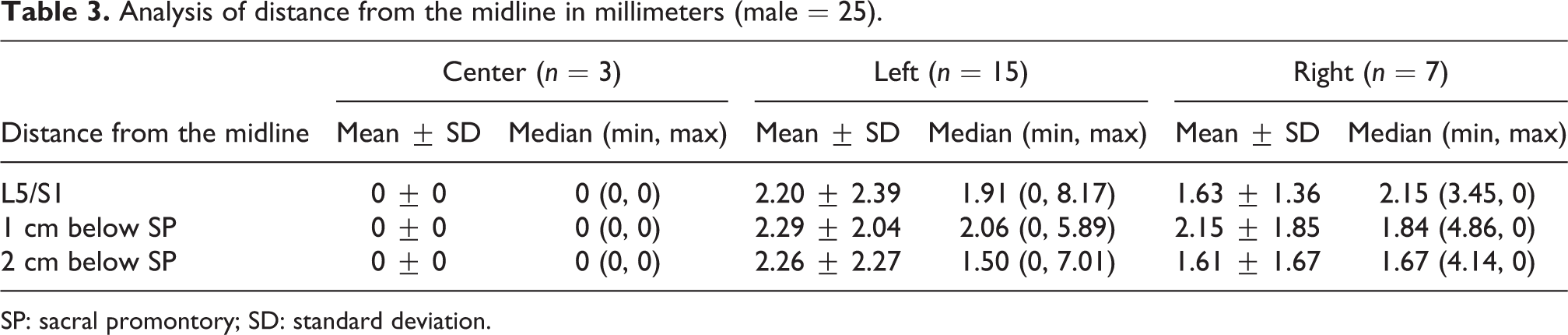
Analysis of distance from the midline in the male group (Table 3) found the MSA was at midline in 3 (12%) of 25 cadavers. The MSA was at the left of midline in 15 (60%) 25 male cadavers, with a median of 1.91 mm (range, 0–8.17 mm) left of midline at the mid-height of L5/S1 disc, 2.06 mm (range, 0–5.89 mm) at 1 cm below the SP, and 1.50 mm (range, 0–7.01 mm) at 2 cm below the SP. The MSA was at the right of midline in 7 (28%) of 25 male cadavers, with a median of 2.15 mm (range, 0–3.45 mm) right of midline at the mid-height of L5/S1 disc, 1.84 mm (range, 0–4.86 mm) at 1 cm below the SP, and 1.67 mm (range, 0–4.14 mm) at 2 cm below the SP.
Analysis of distance from the midline in millimeters (male = 25).
SP: sacral promontory; SD: standard deviation.
Analysis of distance from the midline in the female group (Table 4) found the MSA was midline in 2 (8%) of 25 female cadavers. The MSA was at the left of midline in 13 (52%) of 25 female cadavers, with a median of 1.65 mm (range, 0–6.84 mm) left of midline at the mid-height of L5/S1 disc, 2.75 mm (range, 0–7.10 mm) at 1 cm below the SP, and 2.53 mm (range, 0–9.76 mm) at 2 cm below the SP. The MSA was at the right of midline in 10 (40%) of 25 female cadavers, with a median of 1.38 mm (range, 0–9.64 mm) right of midline at the mid-height of L5/S1 disc, 2.24 mm (range, 0–9.95 mm) at 1 cm below the SP, and 3.63 mm (range, 0–10.03 mm) at 2 cm below the SP.
Analysis of distance from the midline in millimeters (female = 25).

SP: sacral promontory; SD: standard deviation.
Discussion
The MSA is an unpaired vessel forming the last branch of the aorta, 7 typically traveling along the ventral surface of the lumbosacral area terminating at the sacrococcygeal junction, and along its course contributing to the parietal and visceral branches of the lateral sacral arteries and posterior rectum. 6,8,9 The MSA is at risk during the AxiaLif approach in the presacral space; however, there has been limited anatomic evaluation of the pathway of MSA below the SP. 1,2
We performed a human cadaveric study of the MSA to analyze the anatomic pathway in relation to the spinal midline in the presacral region. Our study found the MSA originating from the left CIA in all specimens, with the level of aortic bifurcation not lower than the L5 vertebral body. We most commonly found the MSA at the left of midline (56%), with only 10% at the midline, and 34% at the right of midline. In the left MSA group, the artery pathway remained approximately 2 mm at the left of midline along its course from proximal to distal. This is compared to the right MSA group, where the artery pathway increased in distance from the midline along its course from proximal (1.44 mm at L5/S1 disc space) to distal (2.92 mm at 2 cm below the SP; Figure 3).

Drawing picture showing 10% of the MSA was midline, 56% was at the left of midline, and 34% was at the right of midline (3(a)). In the left MSA group (3(b)), the artery pathway remained approximately 2 mm at the left of midline along its course from proximal to distal. This is compared to the right MSA group (3(c)), where the artery pathway increased in distance from the midline along its course from proximal to distal. MSA: middle sacral artery.
During the AxiaLif procedure, the MSA and its course below the SP may not be adequately visible in standard MR or computed tomography (CT) imaging. Therefore, preoperative MR or CT angiography of this region can be considered to identify the pathway of the MSA. However, the validity and necessity of routinely obtaining advanced imaging with angiography to identify the MSA prior to the AxiaLif approach is unknown. When the exact location and pathway of the MSA cannot be determined based on preoperative imaging, the findings of our study suggest the AxiaLif approach can still be considered if performed along the right side of the presacral area prior to localizing the starting point at midline of S1, because the majority of MSAs were found away from the right side (66%). However, even in the setting of a right-sided MSA (34% of specimens), the artery shows increasing distance from the midline as it courses from proximal to distal (Figure 3), theoretically placing the MSA at less risk even with a right-sided approach. Future clinical studies are needed to determine the efficacy and safety of routinely using a right-sided approach, and whether there may be a cutoff value regarding the course of the MSA that would place this vascular structure at risk.
To our knowledge, there have been only a few previous studies evaluating the MSA and its relationship to the AxiaLif approach. Yuan et al. 6 in 2006 evaluated the paracoccygeal approach and defined a “coronal safe zone” within the presacral space between the internal iliac vessels. The authors concluded that the coronal safe zone is 6.9 mm and 6.0 mm on magnetic resonance image (MRI) and CT, respectively. However, this study was primarily based on measurements from imaging studies, with a review of 12 MRIs and 14 CTs, with direct measurements of the MSA in only two human cadaver specimens. The MSA was found to be midline in one specimen, and at 4 mm left of the midline in the other. This is compared to the current study that directly measured the MSA distance from the midline in 50 cadaveric specimens.
In another study, Tribus and Belanger 10 evaluated 35 human cadavers (17 males and 18 females). The anterior L5/S1 disc space and great vessel bifurcation were exposed through a transabdominal approach to study the vascular anatomy anterior to L5/S1 disc space. The authors found MSA in all cadavers, with a mean width of 2.5 mm at the L5/S1 disc level but had a variable course. The authors suggested that MSA be identified and controlled during the exposure of L5/S1 in an ALIF approach and that MSA was not a reliable anatomical landmark for the spinal midline at the L5/S1 disc space. This study, however, did not evaluate the course of the MSA below the SP, which is the focus of the current study on the AxiaLif approach to the presacral space.
A more recent study by Sae-Jung and colleagues 11 evaluated the MSA at the L5/S1 interspace in 54 embalmed cadavers. The authors also found the MSA course along the left side of the L5 body with an average of 2.39 cm (2.25–2.52 cm with 95% CI) medial to the left lateral border of the vertebral body, compared to 3.31 cm (3.17–3.46 cm with 95% CI) from the right lateral border. However, similar to previous studies, the course of MSA distal to the SP was not evaluated.
Overall, our study provides important findings on the anatomic course of the MSA below the SP and is specifically relevant for the AxiaLif procedure because of the minimally invasive approach and inability to directly visualize the MSA during exposure. However, according to Marotta and colleagues, 2 “bleeding from the transverse sacral vein and the middle sacral artery is also possible” but suggested MSA is often small or nonexistent below the SP in the S1–S2 presacral area. Our study does not support this claim based on the finding that MSA was found below the SP in the presacral area in all specimens, and previous studies reported bleeding complications due to the AxiaLif technique. 4 As in any cadaveric study, there are inherent limitations, and although to our knowledge this is the largest cadaveric study to date evaluating this topic, the limited sample size may not represent all demographics or patient populations. In addition, anterior osteophytes or other spondylotic changes that may alter the anatomic course of the MSA were not addressed in our study, and the absence of body habitus measurements (e.g. height, weight, abdominal girth), which were not available for analysis, could have affected study measurements. Another limitation is the use of transabdominal approach, with the specimen in the supine position to access the presacral space while performing direct cadaveric measurements in our study. The AxiaLif approach is a minimally invasive approach performed in the prone position, and although there is a possibility that the course of the MSA may be different between the supine and prone positions, open dissection and measurement of the anteriorly located MSA in the prone position were not feasible. Thus, the transabdominal approach provided the widest dissection with the least amount of disruption to the native anatomy.
Conclusions
Our study found MSA in 100% of specimens, which was predominantly (56%) at the left of midline in the presacral area, with an average distance of 2 mm lateral to the midline throughout its anatomic course from cephalad to caudad. When the right of midline MSA variant (34%) was encountered, the MSA’s course distal to the SP became more lateral to the midline. Our study confirms MSA has a variable anatomic course, and the AxiaLif procedure may place the MSA at greatest risk of injury when placed at the left of midline.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.