
Abstract
Purpose:
Although several cases of anatomical variants of the proximal portion of the long head of the biceps brachii tendon have been reported, most are case reports on single patients; few studies have investigated the classification and incidence of this phenomenon. We aimed to classify the variants of the long head of the biceps brachii tendon by their morphology and characterize them in regard to incidence, demography, and the relationship with biceps tendon or other shoulder diseases.
Methods:
We retrospectively reviewed 760 arthroscopic images spanning 31 months from October 2008 and found 45 variations of the proximal portion of the long head of the biceps brachii tendon. We classified the variants using Dierickx classification system and calculated the incidence of each subtype. We investigated age, gender, bicipital morbidity rate, procedure rate, and the frequency of related shoulder disease among the variant groups using patient data and compared the groups to normal patients.
Results:
The overall incidence of variants was 6.5% (67.4%, mesotenon; 32.6%, adherent; 0% split (SPL); and 0% absent (ABS) type). Morbidity and procedure rates of the long head of the biceps (LHB) tendon in the variant group (27.9% and 25.6%, respectively) were lower than in the normal group (40.5% and 38.9%, respectively), but the difference was not statistically significant (p = 0.102 and 0.082, respectively). Rotator cuff tear was significantly less common in the mesotenon (44.8%) group than in the normal group (62.4%; p = 0.004). Shoulder joint instability was more prevalent in the mesotenon (27.6%) group than in the normal group (14.9%), but the difference was not significant (p = 0.305). The distribution of other shoulder diseases in the adherent group was similar to that in the normal group.
Conclusions:
The incidence of variants of the long head of the biceps brachii tendon was 6.5%, and most variants were mesotenon or adherent type. The SPL and ABS types were rare. Morbidity and procedure rates of the LHB were not significantly different between the variant group and the normal group, and rotator cuff tear was less common in the mesotenon group.
Introduction
The biceps brachii has two origins, and the long head of the biceps (LHB) tendon is known to have its origins in the superior labrum or the supraglenoid tubercle, with a 50% frequency for each origin. 1 The tendon typically runs free along its intra-articular, extrasynovial course and is ensheathed by the continuation of the synovial lining of the articular capsule that extends to the inferiormost extent of the bicipital groove.
Anatomical variants around the origins are reported to occur with a frequency of 1.9–7.4%, 2,3 and many variations in shape, including complete absence, split or Y-shaped variant, and extracapsular origin of LHB have also been reported. 4 –14 However, most of previous studies that have reported such findings only studied a small sample of participants. Only few authors classified or analyzed the variants systematically with a large participants group. 2,3 Moreover, the relationship between the variants and shoulder joint diseases is controversial. 3,6,12 –16
This study aimed to identify the frequency of variants observed during arthroscopic shoulder surgeries, to classify them based on the Dierickx classification system (Table 1), 2 and to analyze the frequencies, demographic characteristics, and relationship to shoulder disease, including disease of the LHB, for each type of variant.
Dierickx classification: 12 types of variations of the intra-articular portion of the long head of the biceps.
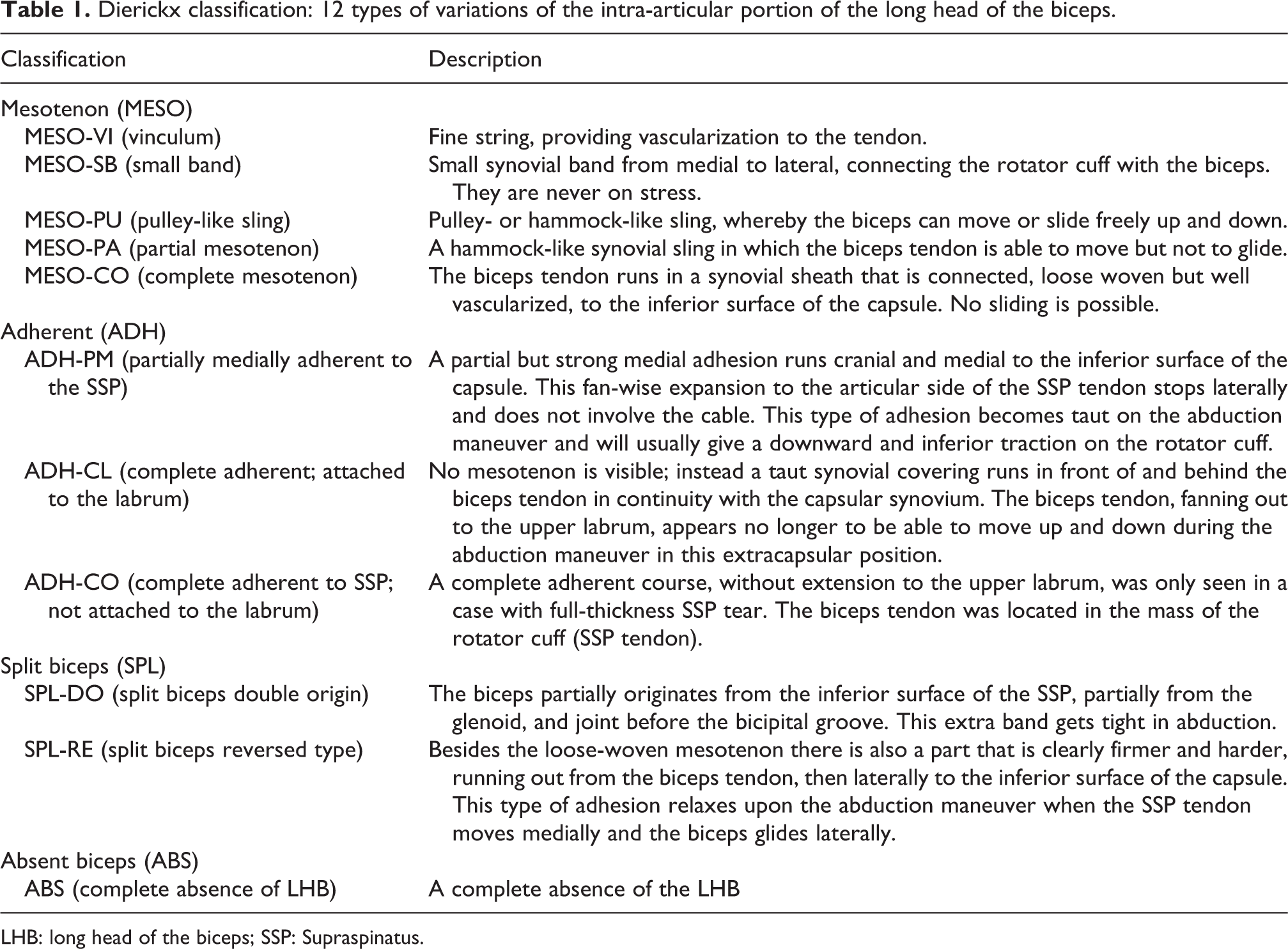
LHB: long head of the biceps; SSP: Supraspinatus.
Methods
Ethical committee approval was not required for this study because this was a retrospective review of 660 previous cases. No biopsies or special procedures were performed or needed for this study.
The study was conducted on 795 cases of shoulder arthroscopy that were performed in our hospital by a single surgeon over 2 years and 7 months from October 2008. Thirty-five cases in which the patients had received previous treatments on the LHB or the long head was completely self-ruptured were excluded. One hundred cases with large to massive rotator cuff tear were excluded too. Arthroscopic images and medical records were retrospectively analyzed for 660 cases. Arthroscopic videos were also used when arthroscopic images were not enough to figure out and classify the variants. In addition, the variants were classified according to the classification method suggested by Dierickx et al., 2 and the frequency of each type, age at the time of surgery, gender, morbidity rate/procedure rate of the LHB, and frequency of other shoulder diseases were compared with those of the normal group. Patients who underwent surgeries on both shoulders were identified, and the frequency of bilateral abnormality of LHB was investigated. In this study, LHB morbidity was divided into three types as dislocation, subluxation, and partial tear. We defined dislocation of the LHBT as when the tendon is positioned more medially within the bicipital groove than usual, and subluxation as when the tendon is positioned superior to the medial border rather than within the groove. 17
Statistical analysis of the data was conducted using the χ 2 test, Wilcoxon rank-sum test, Kruskal–Wallis test, and Fisher’s exact test using SAS version 9.4 (SAS Institute, Cary, North Carolina, USA) and R 3.2.5 (Vienna, Austria; http://www.R-projection.org/). p Values below 0.05 were considered significant.
Results
Of the 660 cases of shoulder arthroscopy, 359 involved male patients (54.4%), 301 involved female patients (45.6%), and the average age at surgery was 52.4 years. Anatomical variants in the LHB were observed in 43 cases (6.5%). Patient ages at the time of surgery, gender, LHB morbidity rate/procedure rate, and main shoulder diseases were analyzed and compared with 617 cases of normal LHB. The variant group comprised 27 male (62.8%) and 16 female (37.2%) patients, and the average age at the time of surgery was 47.8 years. The normal group comprised 332 male (53.8%) and 285 female (46.2%) patients, and the average age at surgery was 52.7 years.
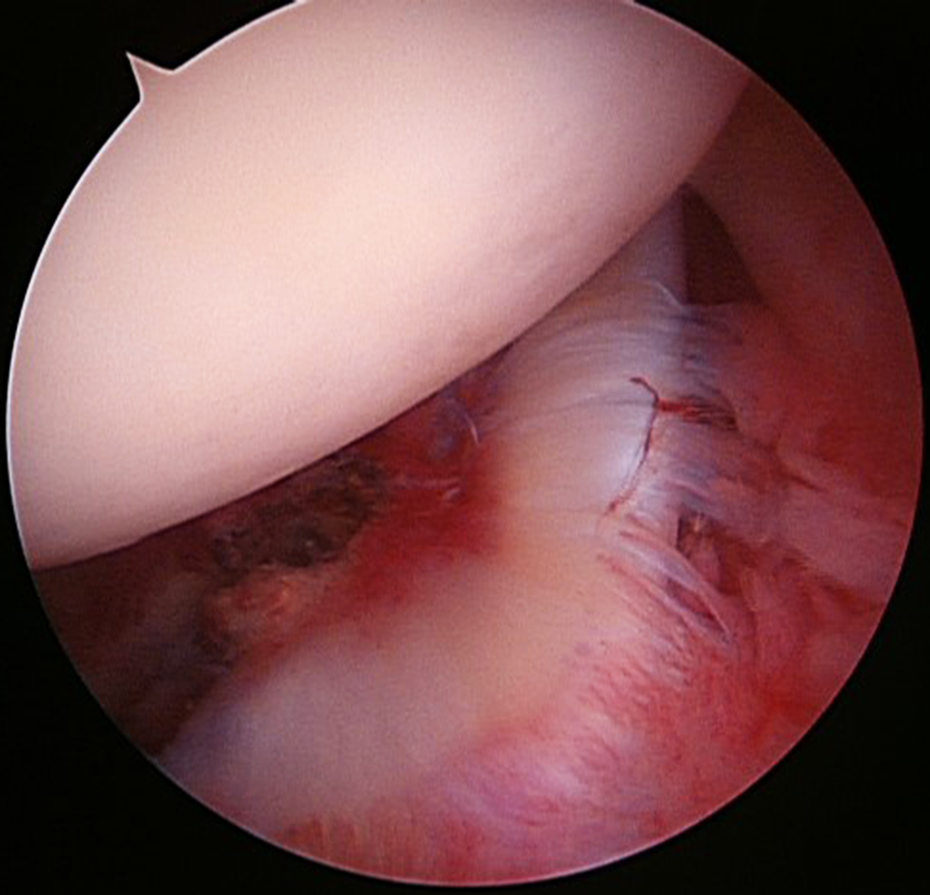
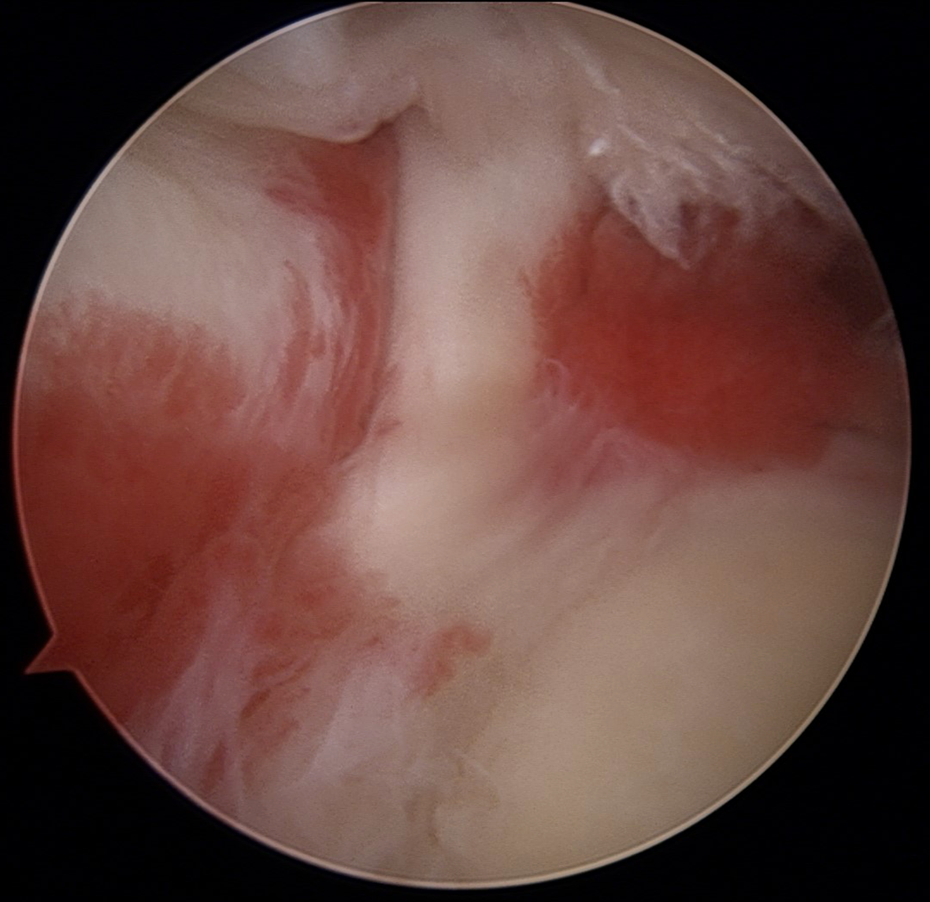
When the variants were classified by shape according to the Dierickx classification system, 29 cases (67.4%) were the mesotenon (MESO) type, and 14 cases (32.6%) were the adherent (ADH) type. Of the 29 MESO cases, 26 cases were pulley-like sling (MESO-PU; Figure 1(a) and (b)), and 3 cases were complete mesotenon (MESO-CO; Figure 2). Of the 14 ADH cases, 4 cases were partially medially adherent (ADH-PM; Figure 3), 9 cases were complete adherent and attached to the labrum (ADH-CL; Figure 4), and 1 case was complete adherent and not attached to the labrum (ADH-CO; Figure 5). Absent (ABS) type and split (SPL) type were not observed.

(A,B): MESO-PU (pulley-like sling) biceps variation type.
MESO-CO (complete mesotenon) biceps variation type.

ADH-PM (partially medial adherent to the supraspinatus tendon) biceps variation type.

ADH-CL (complete adherent and attached to the labrum) biceps variation type.
ADH-CO (complete adherent and not attached to the labrum) biceps variation type.
In the variant group, 3 cases (7.0%) had LHB dislocation or subluxation, and 9 cases (20.9%) had partial tears. In the normal group, 46 cases (7.5%) had LHB dislocation or subluxation, and 204 cases (33.1%) had partial tears. The frequency of LHB lesion was lower in the variant group, but this difference was not statistically significant (p = 0.102; Table 2).
Gender, age, disease of the long head of the biceps tendon, and treatment rate for each type of variant.

MESO: mesotenon type; ADH: adherent type; SLAP: superior labral anteroposterior.
aThe total bicipital morbidity rate in the variant group was 12/43 (27.9%) and was less than that in the normal group (250/617, 40.5%), but the difference was not significant (p = 0102).
In the variant group, common accompanying disease was rotator cuff tear with 23 (53.5%) cases, followed by 11 (25.6%) cases of superior labral tear from anterior to posterior (superior labral anteroposterior (SLAP) lesion), 8 (18.6%) cases of adhesive capsulitis, and 8 (18.6%) cases of anterior instability.
The MESO type variant group had a lower frequency of rotator cuff tear compared to the normal group (44.8%:62.4%, p = 0.004). Although the frequency of shoulder instability was higher in the MESO type variant group than in the normal group, the difference was not statistically significant (27.6%:14.9%, p = 0.305). The ADH type variant group had a similar distribution of diseases as that observed in the normal group.
Two of the 43 cases underwent arthroscopy in both shoulders during the study period. In these cases, LHB variants were only found in one shoulder.
Discussion
In this study, the frequency of anatomical variants of the LHB was 6.5%. All the variants were MESO and ADH types. SPL and ABS types were not observed. The variant group had lower LHB morbidity and procedure rates than the normal group, but the difference was not statistically significant. The MESO type variant group had a lower frequency of rotator cuff tear than the normal group, but the difference was not statistically significant. And the ADH type variant group showed a disease distribution that was similar to that of the normal group. Among patients who received surgery for rotator cuff tear, the average age at the time of surgery in the variant group was 2.6 years younger than that in the normal group, but the difference was not significant.
The LHB has traditionally been known to originate in the supraglenoid tubercle. However, a study by Pal et al. 18 reported that the tendon originated from the supraglenoid tubercles in only 25% of cases, while in 70% of cases, the tendon originated from the posterosuperior labrum. Vangsness et al., 1 who studied 105 cadavers, reported that 50% of LHBs originated from the supraglenoid tubercle, while the other 50% originated from the superior labrum. The tendons normally extend anterolaterally inside the joint and exit the joint through the bicipital groove after passing by the stabilizing pulley.
Embryologically, the LHB is known to transmigrate from outside the joint into the joint. 19 During this process, variants are caused when separation from the mesothelium or the synovial sheath is incomplete. 5,20,21
The frequency of morphologic variants with regard to the origin of the LHB is reported to be 1.9–7.4%. 2,3,8 Greig et al. 22 reported that of 130 cases in a cadaver study, the LHB originated from the joint capsule in 3 cases. With recent advances in arthroscopic technology, variants are now more frequently reported. The frequency of observed variants was 6.5% in this study, which was similar to the frequencies reported by previous studies. The study by Dierickx et al., 2 with 57 variant cases out of a total of 2976 arthroscopy cases, classified the variants into the MESO (50.9%), ADH (26.3%), SPL (15.8%), and ABS (3.5%) types. Each type was further classified into different subtypes based on the shape. In this study, the MESO type accounted for 67.4% of cases, while the ADH type accounted for 32.6% of cases. These results differed from the results of previous studies since the SPL and ABS types were not observed. One possible reason for this difference is racial difference, because most of the participants in our study were Korean.
Although the correlation of these variants with different diseases is unclear, it is traditionally known that these variants in themselves do not cause diseases. However, many researchers claim that the variants are related to supraspinatus tendon tear, 2,15 SLAP lesion, 13 glenoid avulsion of the glenohumeral ligaments, 12 and shoulder instability. 6 In this study, the MESO type variant group had a low frequency of rotator cuff tear. The cause of the difference of our study is unclear. One possible reason is the small number of participants in each study, including our study.
It is a debatable question whether the mesotenon and pulley-like sling have some stabilizing function or not. We believe that they have no stabilizing function. They can easily be removed with little additional effort and time so we usually take them down and release the biceps tendon.
Although some previous studies have reported variants occurring in both shoulders in an individual, 23 the two cases in this study for which surgeries were performed on both shoulders all showed variants in only one shoulder. Greig et al., 22 in their cadaver studies which aimed to determine variants in biceps including the LHB, reported variants in 28 of 130 cases (22%); bilateral variants were observed in 5 cases, and symmetrical variants were observed in only 3 cases. Greig et al.’s study supports this study’s results that bilateral variants are rare.
This study has several limitations. It is a retrospective study and two groups (normal and variant groups) showed different mean age and distribution of disease, so some bias can exist. Since this study was conducted on patients who underwent shoulder arthroscopy because of shoulder diseases, the frequency of variants in the normal population could not be determined. Moreover, patients were excluded due to previous tenotomy, tenodesis, or complete self-rupture, and these factors might be correlated with specific variant types, which were not identified in this study. This study was conducted on 43 patients’ variant group. Therefore, it is necessary to carry out further research on a larger number of patients in the future. Finally, comparison of the distribution of normal and variant groups by shoulder diseases (rotator cuff tear, SLAP, adhesive capsulitis, anterior instability) may result in a bias in the outcome because the difference between the two groups is too large (617:43).
Conclusions
LHB variants were observed in 6.5% of the patients who underwent shoulder arthroscopy. The MESO and ADH types accounted for the majority of cases, while the SPL and ABS types were not observed. The morbidity and treatment rates of LHB in the variant group and in the normal group were not significantly different. The MESO type variant group had a low frequency of rotator cuff tear, while the ADH type variant group had a similar shoulder disease distribution as that observed in the normal group. Multicenter prospective studies may elucidate other variant types and provide possible correlations between LHB variants and specific disease conditions or predilections.
Footnotes
Acknowledgment
This study was presented at the 28th Fall Congress of Korean Orthopedic Society for Sports Medicine, Seoul, South Korea.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.