
Abstract
Background:
There were very few options available for distal foot and toe defects that required a vascularized flap for coverage. As such, the use of a free flap was often justified in this region of the foot. The use of perforator flaps has created a new subset of local tissue transfer alternatives that increases the potential that the difficulties associated with microvascular tissue transfers could be avoided. The first dorsal metatarsal artery (FDMA) perforator flap was one variant of this new type of tissue transfer. The aim of this report was to describe our experience using FDMA perforator flap to cover great toe defect.
Methods:
A standard FDMA flap from the dorsum of the foot was raised in reversed fashion based on the distal communicating branch or “perforator” from plantar foot circulation in two patients with great toe defect.
Results:
Salvage of the great toe was achieved in both patients. FDMA perforator flap achieved both reconstructive goals, and the donor site closure can be successfully performed without tension. Donor site healing was achieved in both patients with no associated complications by the 1-year follow-up.
Conclusions:
FDMA flap can be successfully used as a local flap to cover distal foot and toe wounds. However, direct donor site closure can be problematic and may need skin graft.
Background
Graft and transfer options for covering distal foot, toe, and web space defects were exceedingly limited. Skin grafts often lack long-term durability, and free flaps were associated with technical challenges and less than optimal postoperative aesthetic and functional results. 1 Toe fillet and partial toe island flaps jeopardized the toes themselves. 2,3 Plantar-based flaps, including intrinsic muscle flaps, have limited reach and size. 3,4 A distal-based dorsalis pedis flap may be used, but at the price of well-documented, significant, and possibly permanent donor site sequela. 5,6 The reverse first dorsal metatarsal artery (FDMA) fasciocutaneous flap offered greater reach than the dorsalis pedis flap. 2,7 –10 The adipofascial version of this flap can yield a larger-sized flap and largely avoid the donor site complications associated with the dorsalis pedis flap, but this flap may need skin grafted at the recipient site. 5
The aim of this report was to describe our experience using FDMA perforator flap to cover great toe defect.
Materials and methods
During 2016, two young children were involved in separate motorcycle accidents and both sustained great toe pathology with exposed bone or joint that required vascularized soft tissue coverage (Table 1). Both patients were referred for treatment. Great toe amputation was not an acceptable option at the insistence of the parents of both children. As an alternative, an FDMA perforator flap was selected for salvage of the great toe in both cases. Written informed consent was obtained from the parents of both children approving the inclusion of their data in this report.
Demographic and clinical characteristics of FDMA perforator propeller flap patients.
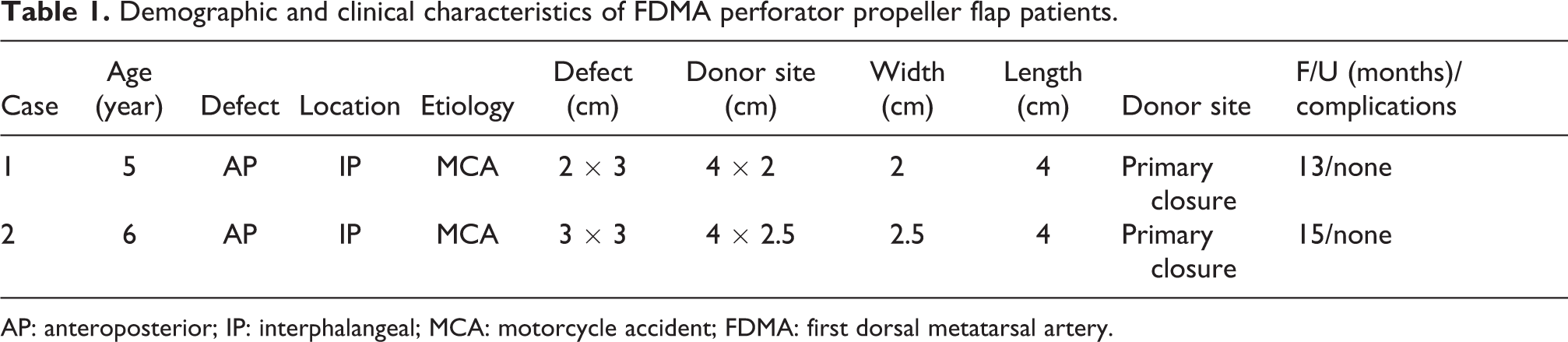
AP: anteroposterior; IP: interphalangeal; MCA: motorcycle accident; FDMA: first dorsal metatarsal artery.
Surgical anatomy
In 86% of feet, FDMA origin is the dorsalis pedis artery or its branch, the deep plantar artery. 11 FDMA origin is typically within 1 cm distal to the tarsal-first metatarsal joint and 5.5 mm plantarwards from the dorsal surface of the second metatarsal bone. 12,13 In about 4% of cases, the artery is either absent or too small to be of any practical consequence. 11 The remaining FDMA arises from plantar circulation. 14 FDMA has three variations. In 11% of cases, the FDMA runs superficial to the first dorsal interosseous muscle. 11 In 84% of cases—after its dorsalis pedis–based origin—the artery passes under the muscular arch formed by the tibial head of the first dorsal interosseous muscle to run adjacent to the first metatarsal bone. 11 At the distal third of the space between the first and second metatarsal bones, it again, in most cases, assumes a superficial location. 11 For the third variation, numerous cutaneous perforators emanate from the FDMA, with the most distal perforator consistently located between the heads of the first and second metatarsals. 7 In all cases when it is present, the FDMA always eventually passes dorsal to the transverse metatarsal ligament before ending at its terminal branches. 11
The next issue of importance involves the branching pattern found in the first web space. The FDMA does not always bifurcate into dorsal digital branches, sometimes giving off a branch only to the great toe or the second toe. 11 However, in 85% of cases, a “perforator” or distal branch will communicate with the first plantar metatarsal artery and this will provide circulation to the FDMA perforator flap. Confirmation by conventional audible Doppler15 is possible, but Hou et al. 11 found color Doppler ultrasound imaging to be more reliable. The flap width should mirror that of the defect but should be limited to 2.5 cm if primary donor site closure is to be possible.
Surgical techniques
The audible Doppler is used to locate the blood flow of the dorsalis pedis artery and follows the course of the FDMA distally to the distal communicating branch with the plantar arterial network, which locates approximately between the first and second metatarsal head. Use of a tourniquet without limb exsanguination allows for identification of venous structures that should be included. Dissection begins at the distal edge and then proceeds toward the perforator found just distal to the transverse metatarsal ligament to confirm its location. The proximal edge is then elevated to expose the dorsalis pedis vessels. This dissection is continued distally in the usual subfascial plane to identify the origin and course of the FDMA. The proximal communicating branch with the plantar arterial network located just distal to the tarsometatarsal joint should be ligated and divided to allow flap rotation. Care is taken to preserve any perforators observed to course to the overlying integument. Flap elevation ceases when the distal communicating branch perforator is again encountered. Fibrous constraints about the distal communicating branch perforator must be released to allow unhindered clockwise or counterclockwise rotation of the flap into the defect. While in situ, the tourniquet is deflated to assess flap perfusion. Then the dorsalis pedis artery should be temporarily clamped and verified that flap has adequate blood supply from reversed flow FDMA. If adequate perfusion is observed, flap rotation is completed and the flap is inset into the defect (Figure 1(a) to (d)).
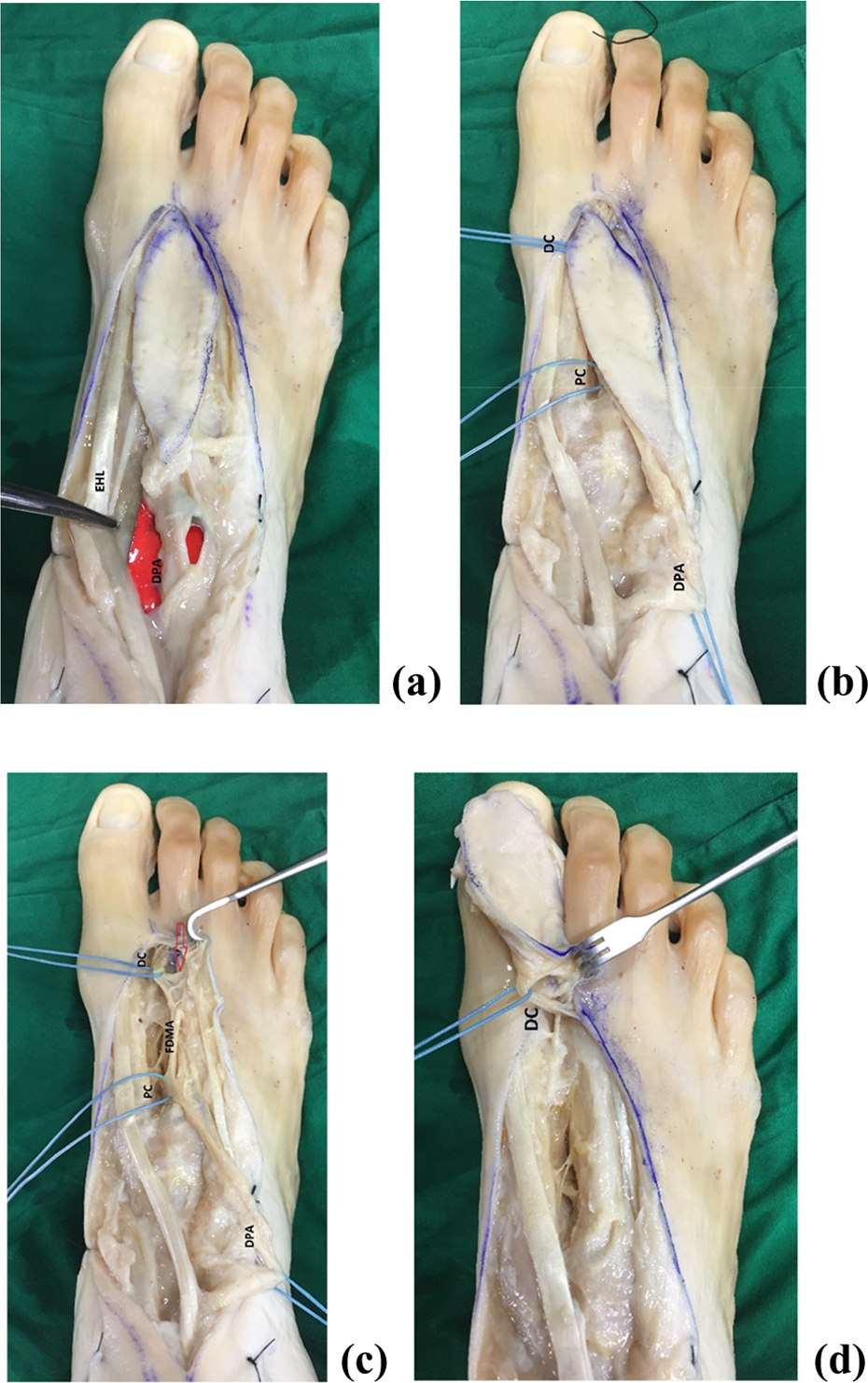
Dorsalis pedis artery was located, then follows the course of the FDMA distally to the proximal and distal communicating branch with the plantar arterial network (a, b). Fibrous constraints about the distal communicating branch perforator must be released to allow unhindered clockwise or counterclockwise rotation of the flap into the defect (c, red arrow). The tourniquet is deflated to assess flap perfusion. Then, the dorsalis pedis artery should be temporarily clamped and verified that flap has adequate blood supply from reversed flow FDMA. If adequate perfusion is observed, flap rotation is completed and the flap is inset into the defect (d). DPA: dorsalis pedis artery, DC: distal communicating branch, PC: proximal communicating branch, EHL: extensor hallucis longus; FDMA: first dorsal metatarsal artery.
Results
Salvage of the great toe was achieved in both patients. FDMA perforator flap can achieve reconstructive goals, and the donor site closure can be successfully performed without tension. Donor site healing was achieved in both patients with no associated complications by the 1-year follow-up.
Case #1
A 5-year-old girl sustained a severe foot injury in a motorcycle accident. Within 3 weeks prior to being referred to our center, her toes became gangrenous after her right great toe and lesser toes became entangled in the gear mechanism of the rear wheel. Debridement with exposure of the dorsal bony structure, the nail plate area, and the interphalangeal joint was performed (Figure 2(a) and (b)). The FDMA and its distal communicating branch with plantar circulation was easily identified using audible Doppler. An FDMA perforator flap 4 cm long and 2 cm wide was designed. Following the described flap elevation, counterclockwise rotation allowed the flap to cover the exposed interphalangeal joint (Figure 2(c)). The donor site was closed by primary sutures. The great toe was salvaged, with no infection and good function (Figure 2(d)).

A 5-year-old girl who suffered a severe foot injury in a motorcycle accident: (a) Development of gangrene in the big toe and lessor toes; (b) after debridement of necrotic tissues; (c) FDMA perforator flap was raised in reverse fashion and inset to fill the defect; and (d) wound healing by secondary healing. FDMA: first dorsal metatarsal artery.
Case #2
A 6-year-boy suffered a serious foot injury in a motorcycle accident. After his right great toe and lessor toes became entwined in the gear of the rear wheel, gangrene developed in the affected toes. Radical debridement exposed the interphalangeal joint of the big toe. An FDMA perforator flap 4 cm long and 2.5 cm wide was designed (Table 1). Clockwise rotation of the flap facilitated complete coverage of the exposed great toe joint. Wound coverage and closure was achieved with no subsequent healing difficulties.
Discussion
Distal foot and toe problems vary in severity and complexity. Ideal surgical solution has yet to be established for each of the range of problems that can adversely affect this part of the foot. Although free flaps have the potential of solving any coverage problem anywhere on the foot, they tend to be bulky, aesthetically unattractive, and they can interfere with shoe wear. However and more importantly, free flaps can be very difficult in a region with limited recipient sites and in patients who, more often than not, cannot tolerate a lengthy procedure—especially one that has a high risk of failure. 15,16 Alternatively, it is reasonable to consider the merits of any local flap option when coverage is required in this region. Distal-based metatarsal artery fasciocutaneous flaps, including the FDMA flap, have so proven their value.2, 8 The adipofascial variant of this flap was proposed to circumvent potential donor site wound healing issues, 5 such as those associated with the long-established dorsalis pedis flap. 6 However, the adipofascial variant requires a skin graft at the recipient site and typically must be tunneled to the defect, which could compress and jeopardize venous outflow as a result of inevitable postoperative swelling. 5 Moreover, the dissection of these flaps is a tedious process that requires a microsurgical technique as true and meticulous as that needed for the dissection of any perforator flap, with no guarantee of adequate skin perfusion after flap elevation. Inadequate release of fascial bands around the communicating perforator after rotation can impede venous outflow, which may result in flap congestion. The emergence of perforator flap as a new flap selection alternative in the lower extremities broadens the number of local flap options and increases the probability that the risks of microsurgery can be avoided. 10,16–17 FDMA perforator flap, given the right anatomical conditions, represents another flap alternative for coverage of defects of the foot. Since 180° rotation of this flap is possible, it can also be used to reach and cover distal plantar foot and toe defects.
Conclusion
FDMA flap can be successfully used as a local flap to cover distal foot and toe wounds, but direct donor site closure can be problematic, similar to complications associated with donor site closure after dorsalis pedis flap transfer.
Footnotes
Acknowledgments
The authors gratefully acknowledge the parents and children for allowing case details to be disclosed in this case report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.