
Abstract
Purpose:
We aimed to present our novel technique in the surgical treatment of Achilles tendon avulsions and compare the clinical results of such technique with the repair method using suture anchors.
Methods:
A retrospective study was made of patients with Achilles tendon sleeve avulsion and patients where distal portion of the tear prohibited primary repair, surgically treated between January 2009 and January 2013. Twenty-one patients who met the criteria were examined and called for final examination: 9 patients were treated with the novel technique (group 1) and 12 patients were treated with suture anchor repair (group 2). Data were gathered from patient registry and final evaluation. The patients of both groups were compared in respect of mean age, follow-up, gender and AOFAS and VAS scores at final evaluation.
Results:
There was no significant difference between two groups in terms of follow-up period (p = 0.478) and mean age (p = 0.274). Three of 9 patients in group 1 and 4 of 12 patients in group 2 were female. A significant clinical difference was determined between two groups according to the AOFAS and VAS scores (p = 0.034 and p = 0.043, respectively).
Conclusions:
Both techniques are beneficial in the treatment of avulsion injuries of Achilles tendon. Better clinical results can be obtained with the presented novel technique and such technique can be considered for the surgical fixation of Achilles tendon avulsions.
Introduction
Achilles tendon ruptures usually occur 2–6 cm proximal to the insertion on the calcaneus bone, while avulsions from the calcaneal insertion are less commonly encountered. 1 Avulsions from the calcaneal insertion or tears occurring in close proximity to the distal end of the tendon insertion represent a challenge in surgical repair due to insufficiency of the distal end, although these tears can be repaired using a suture anchor. 2 Avulsions from the calcaneal insertion with bony fragments can also be observed, for which open reduction and screw fixation are the preferred method in the presence of large bone fragments; however, this method is not effective in the presence of small bony fragments. 3 The use of two anchors is recommended due to the excessive loading on a single anchor in such tendon tears. 4 There is no standard repair method recommended for avulsions without bony fragments or with small fragments where fixation to calcaneal insertion is not possible. The aim of this study was to present a new technique using percutaneous transosseous sutures in order to repair Achilles tendon avulsions from the calcaneal insertion and compare the clinical results of such technique with the repair method using suture anchors.
Materials and methods
Patient selection and study design
This was a retrospective study of patients with Achilles tendon sleeve avulsion and patients where distal portion of the tear prohibited primary repair due to its close proximity to the distal end, surgically treated between January 2009 and January 2013. Inclusion criteria included the patients between the age of 18 and 55 years, surgically treated either two techniques (by surgeon A: the novel technique or by surgeon B: repair with suture anchors. The surgeons were similar in terms of surgical experience) and underwent a rehabilitation programme. Patients who were lost in follow-up have a history of previous ankle surgery or patients with rheumatoid diseases were excluded from the study. The patients in both groups were treated and followed up in the same department and surgery unit. The treatment protocols were standard, except surgical techniques.
A total of 21 patients who met the criteria were examined and called for final examination: 9 patients were operated by surgeon A (group 1) and 12 patients were operated by surgeon B (group 2). Data were gathered from patient registry and final evaluation. The patients of both groups were compared in respect of mean age, follow-up, gender and AOFAS and VAS (0 = No pain, 10 = Worst pain) scores at final evaluation.
Surgical technique
Surgeon A (the novel technique): After general anaesthesia, a pneumatic tourniquet was applied to the thigh and the patients were placed in the prone position. The foot was placed outside of the operating table to permit dorsiflexion and plantar flexion of the ankle. A single longitudinal midline incision approximately 4 cm in length or two mini incisions each measuring 2 cm in length (when the proximal end of the ruptured tendon could not be accessed via a single incision; Figure 1(a) and (b)) were made running close to Achilles tendon insertion and ending at the upper most portion of calcaneus in the posterior. The ruptured end of the Achilles tendon and calcaneal insertion of the tendon were discovered and a debridement was performed. A double layer suture (polydioxanone) was passed through the skin and calcaneal body using a guide pin from the medial to the lateral portion of the heel (Figure 1(c)). Both ends of the suture were passed from medial and lateral sides of the calcaneal bone into the incision site using a curved clamp (Figure 1(d)). A similar suture (free ends of the suture remained in the medial and lateral aspects of the distal end of the tendon) is passed through the tendon often using the Krackow technique (Figure 1(e)). A suture anchor containing two sutures of different colours was placed at the mid portion of the calcaneal insertion at an angle of 45° to the long axis of the calcaneal bone. The sutures that attached to the anchor were passed through the mid portion of the distal end of the tendon. The transosseous suture that passed through the calcaneus bone was tied with the identical suture that passed from the tendon in an appropriate position. Then, sutures that attached to the anchor were tied using a sliding loop suture technique in order to ensure secure placement to the tendon insertion (Figures 2 to 4). Due to the risk of anchor pullout associated with excessive tension during looping, the transosseous suture was first tied with the identical suture placed on the tendon. The wound was closed in layers after motion control and fluoroscopic control (Figures 5 and 6). The leg was placed in a long circular cast with the ankle at a 10° plantar flexion.
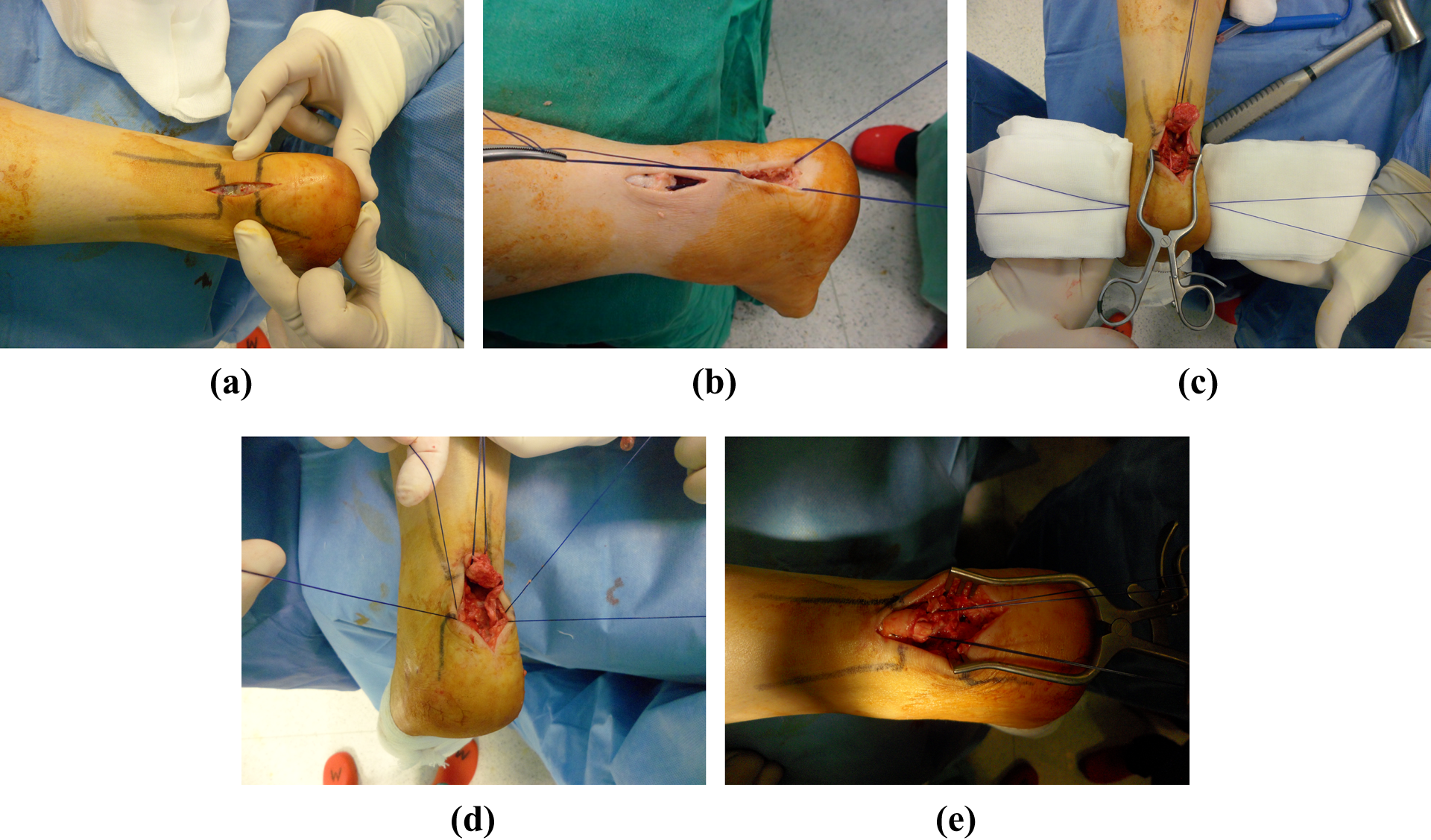
Preferred single (a) and double (b) incisions. (c) Insertion of the percutaneuos transosseous suture through the calcaneal bone using a guide pin. (d) The suture, which is passed through the calcaneus percutaneously, is pulled to the incision site using a curved clamp. (e) Suspension of the ruptured end of the tendon using the Krackow technique.
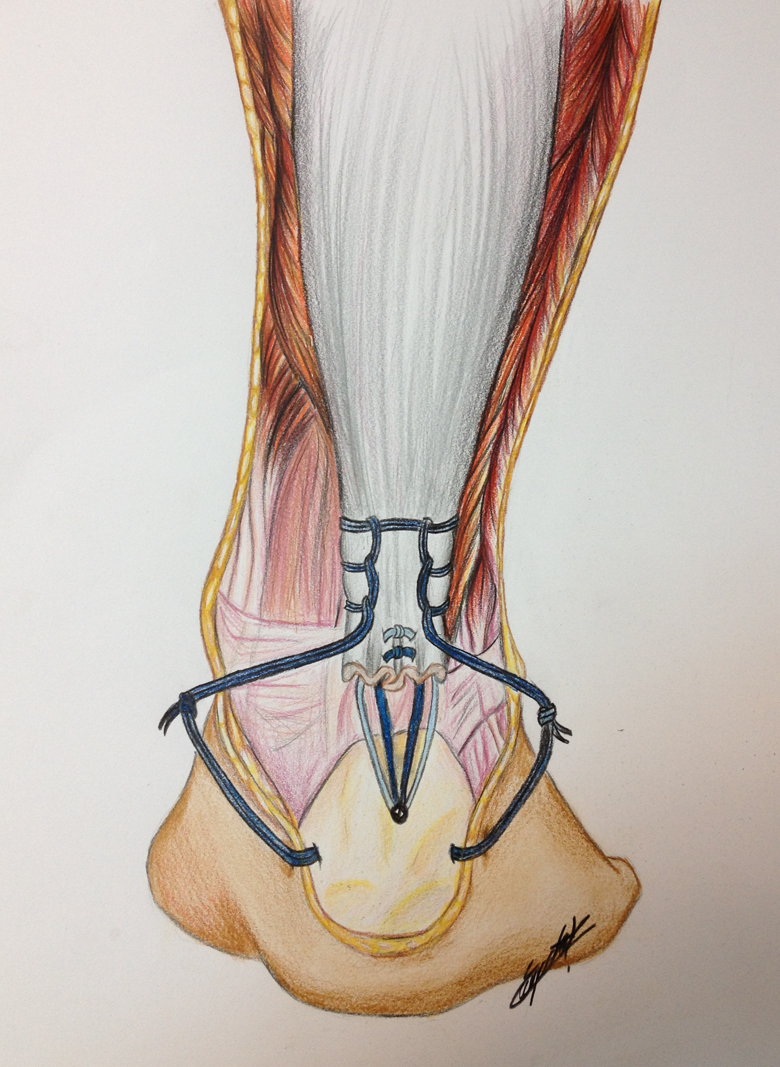
Illustration of the technique.

Fixation of the tendon to the bone.

Fixation of the tendon to the bone.

Lateral radiography of the left ankle shows an Achilles tendon avulsion with small bone fragment.
Control for the suture anchor placed during surgery.
Surgeon B (repair with suture anchors): The same patient setup and position was used by surgeon B and the foot was placed outside of the operating table. A single posteromedial incision approximately 10 cm in length was made running close to Achilles tendon. The ruptured end of the Achilles tendon and calcaneal insertion of the tendon were discovered and a debridement was performed. A 2 cm long trough was created on the calcaneal cortex using a burr in order to obtain a bleeding trabecular bone surface. Then, two (three, if there was enough space) 5.0 titanium anchors were threaded just beneath the trough (with 0.5 cm gap between the anchors). Both ends of the suture were passed through the tendon using the Krackow technique and the terminal portion of the tendon was inserted into the trough. The wound was closed in layers after motion control and fluoroscopic control. The leg was placed in a long circular cast with the ankle at a 10° plantar flexion.
Rehabilitation
Both surgeons implemented the same rehabilitation programme: The cast was removed in the second postoperative week. An ankle brace was applied after control of the wound site, and ankle mobilization exercises were initiated. Partial weight bearing with ankle brace was applied at the third postoperative week. Full weight bearing was started at the end of the sixth week, and muscle-strengthening exercises were initiated. The ankle brace was removed at the end of the tenth week (Figures 7(a) and (b) and 8(a) and (b)).

(a) and (b) In the postoperative tenth week, the patient had unlimited plantar flexion and dorsiflexion of the ankle.
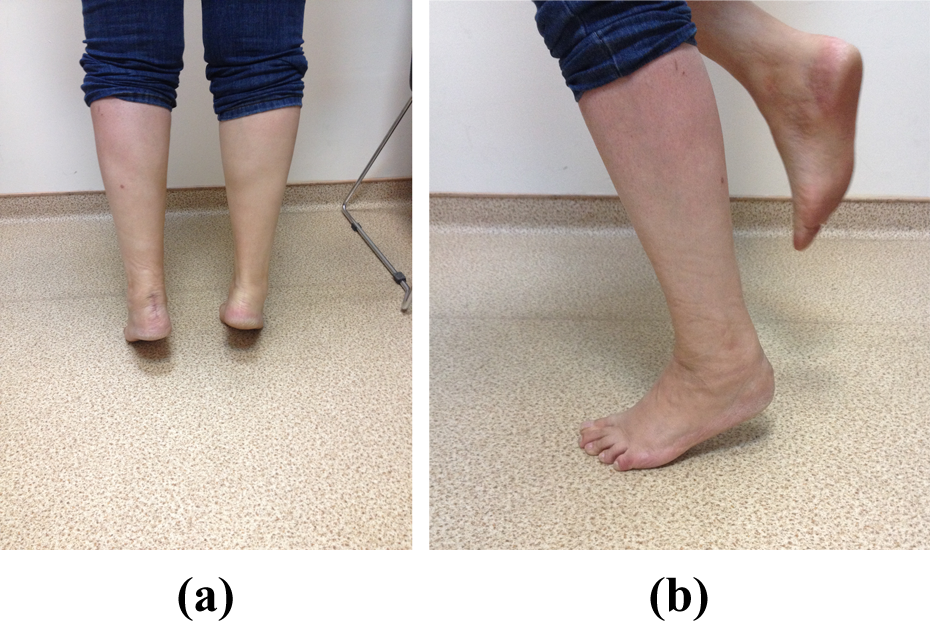
(a) and (b) The patient was able to bear their full weight on the ankle in the postoperative tenth week.
Statistical analysis
Statistical analysis of the data was made with IBM SPSS Statistics version 23 software. The Kolmogorov–Smirnov test was used for variable groups, Student’s t-test was used for variables with normal distribution and values were presented as mean. Pearson χ 2 test was used in comparison of categorical values. A two tailed p-value of <0.05 was considered statistically significant.
Results
Of the patients who were operated by surgeon A, four had bony fragments, and five patients had tendon rupture without avulsing bony fragments from the calcaneus, whereas seven patients had tendon avulsion and five patients had bony fragments that were operated by surgeon B. Due to retraction, a double incision was preferred in three patients, assuming that the ruptured end of the tendon and the calcaneal insertion could not be reached via single incision. All incisions made by surgeon A fully recovered without complication (Figure 9(a) and (b)), and all patients achieved tendon recovery without requiring a second surgical intervention. One patient operated by surgeon B had a failure caused by anchor displacement (pull-out from calcaneus) and needed a revision surgery. Such patient was revised with suture anchor repair following debridement of scar tissue.
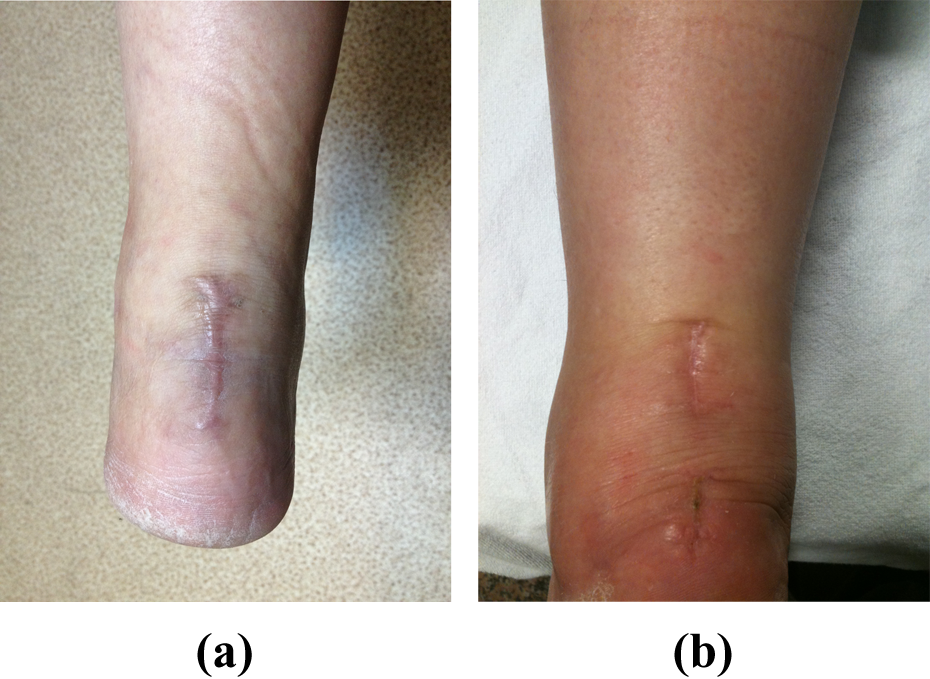
Single (a) and double (b) incisions showed full recovery without any complications.
The mean follow-up period of group 1 was 62 ± 17 months and group 2 was 59 ± 23 months. The difference was not significant (p = 0.478). Mean age of group 1 was 37 ± 11 and group 2 was 40 ± 13. The difference was not significant (p = 0.274). Three of 9 patients in group 1 and 4 of 12 patients in group 2 were female.
A significant clinical difference was determined between two groups according to the AOFAS score (p = 0.034): The mean AOFAS score was 91.6 ± 12.3 in group 1 and 84.4 ± 14.8 in group 2. The difference between VAS scores was also significant (p = 0.043). Mean VAS score was 1.1 ± 0.2 in group 1 and 2.2 ± 0.8 in group 2.
Discussion
There is no widely accepted standard treatment method for Achilles tendon rupture, and information in literature is very scarce regarding the treatment of Achilles tendon avulsions. 5 Although screwing, tension band wire or Steinmann pin fixation is preferred in the repair of calcaneus avulsion fractures, poor bone quality, the lack of sufficient bone tissue or sleeve avulsions without avulsing a bony element prompt surgeons to search for alternative fixation methods. 3,6 We performed open reduction and fixation in 11 cases over the last 5 years using one transosseous suture and one suture anchor in the repair of Achilles tendon avulsions. Using this technique, we were able to pull down the tendon to the original insertion level. Using transosseous suture to pull down the tendon to its original site, we fixated the tendon to the calcaneal insertion with a suture anchor so as to create a large tendon–bone interface.
Lui reported good outcomes with a double suture anchor in the presence of avulsions with small bony fragments, and the technique was suggested to be an alternative to screw fixation that reduced pull-out resistance. 4 Screw heads and other metallic fixation methods can cause skin irritation, but with this technique, the use of suture anchors prevents such complications by being embedded into the bone. Based on the same logic, we came up with the technique described above in order to increase resistance against pull-out and to circumvent the need for the later removal of the fixation material due to skin irritation or other reasons. As an advantage to the method put forward by Lui, we did not require a large incision, in that the suture passed through the calcaneal bone using a percutaneous transosseous guide pin, as we did not require visualization of the posteromedial or posterolateral portion of the calcaneus during the placement of the suture anchor. Access was gained to the insertion and ruptured end of the Achilles tendon through a small midline incision, and we were also able to pass a transosseous suture beneath the soft tissue planes and attach the bone at the incision site using a curved clamp. The sutures running through the medial and lateral aspects of the calcaneus were tied together using the sutures that passed from medial and lateral aspects of the tendon. Then, the tendon was placed at the insertion site using the suture anchor. We therefore consider that sufficient fixation was achieved in the Achilles tendon avulsion using a technique that could be regarded as a minimally invasive. In this context, there were significant differences between two groups in terms of AOFAS and VAS scores. We believe that our novel technique was less invasive and it necessitated a shorter incision. So, it is expected that there would be less scar tissue in the surgical area which might play a role in the clinical results.
There has also been debate about the site of the skin incision due to such complications as wound dehiscence, infection, adhesions and nerve injury. Although longitudinal skin incisions are used in various lengths, there are reports also of the use of transverse incisions. 7 Longitudinal incisions can be made on the medial or lateral aspects, or precisely over the tendon, although the preference in the present study was a short midline longitudinal incision, as described above, with the intention being to minimize injury to the sural nerve, which occurs most frequently after lateral incisions or adhesions and leads to wound problems associated with large incisions.
Bibbo used a different transcalcaneal suture for the repair of an Achilles sleeve avulsion, first resecting the postero-superior calcaneal prominence using an extensive approach and then performing a fixation by passing the sutures attached to the Achilles tendon through a tunnel created from the postero-superior to inferior portion of the calcaneus. Then they described a new technique similar to the first one, in which they pulled down and suspended the tendon using two incisions, measuring approximately 4 cm, at the level of the gastrosoleus muscle and the posteromedial aspect of the calcaneus. These sutures were then passed through the bone tunnel and tied together above the plantar fascia using a transverse incision to the plantar aspect of the heel. This technique was later modified by Pavlou et al. 8 –10 In our technique, the suture is passed through the calcaneus in a transverse rather than longitudinal direction. We ensured a more durable bony bridge in the distal end of the repair by passing the suture through the calcaneus across its mediolateral diameter. In addition, no additional incision was required for the tying of the sutures passing through the calcaneus, and plantar fat pad was left intact. We consider that a transverse percutaneous transosseous suture combined with suture anchor provided sufficient resistance against pull-out tension of the triceps surae muscle. All patients started a range of joint motion exercises at the end of the second week and partial weight bearing at the end of the third week. None of the patients experienced a loss of fixation or re-rupture.
Another advantage of our technique is the removal of the need for such additional and complex procedures as the use of the plantaris tendon, gastrocnemius fascia or peroneal tendons. The technique is also cost-effective based on the lack of need for the use of such expensive materials as allografts or artificial tendon implants.
Conclusion
Achilles tendon avulsions can be treated successfully with a combination of a transosseous suture and a suture anchor through a minimal incision. Both techniques are beneficial in the treatment of avulsion injuries of Achilles tendon. Better clinical results can be obtained with the presented novel technique and such technique can be considered for the surgical fixation of Achilles tendon avulsions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.