
Abstract
Purpose:
Venous thromboembolism prophylaxis is crucial. To facilitate active ankle movement in postoperative and bedridden patients, we developed a novel leg exercise apparatus (LEX). We investigated the effect of the LEX by comparing increases in lower extremity venous flow during different modes of exercise using the LEX.
Methods:
In eight healthy participants, we measured venous flow volume and velocity in the femoral vein using duplex ultrasonography at 1, 10, 20, and 30 min after completing three modes of 1-min LEX exercises. The exercises involved (1) rapid single motion (ankle dorsi–plantar flexion; 60 cycles/min); (2) slow single motion (30 cycles/min); and (3) slow combined leg motion.
Results:
Flow volumes after modes 1, 2, and 3 were 1.63-, 1.39-, and 1.53-fold above baseline at 30 min, respectively. Short periods of rapid single motion, with the LEX, improved postexercise lower extremity venous flow volumes at 30 min and mean venous flow velocity at 20 min, compared to slow single motion exercise. Even at slow speeds, combined-motion improved flow volume compared to single motion.
Conclusion:
Short periods of rapid single motion exercise, with the LEX, improved postexercise venous flow volumes in the lower extremities at 30 min and mean venous flow velocity at 20 min. These effects were greater than those produced by slow single motion exercises. However, even at slow speeds, combined-motion exercises improved flow volume compared to single motion. Therefore, LEX may prove effective at preventing thromboembolism in postoperative and bedridden patients.
Keywords
Introduction
Venous thromboembolism (VTE) is a serious condition for which prophylaxis is crucial. The components of Virchow’s triad—hypercoagulability, stasis, and endothelial dysfunction—are all risk factors for VTE. Bedridden patients (e.g. patients with cancer or those in the early postoperative period following orthopedic, gynecological, or major surgery) require such prophylaxis. Clinical practice guidelines by the American College of Chest Physicians, American Academy of Orthopedic Surgeons, and Japanese Circulation Society recommend both mechanical and pharmacological VTE prophylaxis. 1 –7 Pharmacological prophylaxis carries the risk of severe bleeding, and in patients who are at the risk of bleeding, such as those with cancer or postspinal surgery, mechanical prophylaxis must be used. 1 –17
One recommended method of mechanical VTE prophylaxis is active leg movement. 7,8,11,12 Combined ankle movement improves venous velocity in the lower extremities more effectively than single ankle movement. 12 However, postoperative and bedridden patients with weakness, fatigue, or pain may not be able to move their ankles adequately or perform combined leg movements. In collaboration with Nemoto, Co., Ltd (Ibaraki, Japan), we developed a novel leg exercise apparatus (LEX) to facilitate active leg movement. The LEX is designed to be used in the supine position, specifically for postoperative and bedridden patients. 18 –21 We previously reported that a short period of active ankle exercise with the LEX improved femoral venous flow volume compared to continuous intermittent pneumatic compression. 18 The LEX makes combined leg motion possible, which involves ankle dorsiflexion/plantar flexion, ankle inversion/eversion, and knee and hip flexion/extension. However, our previous report described only the effect of a single ankle motion dorsiflexion/plantar flexion exercise and did not describe the effects of exercise speed and combined leg motion with LEX. 18
Exercise increases cardiac output, and skeletal muscle contraction facilitates circulation in the lower extremities by attenuating sympathetic vasoconstriction to ensure proper blood flow to the muscles. 22,23 Exercises performed with the LEX are designed to increase venous flow in the lower extremities.
We hypothesized that short periods of LEX exercise would improve venous flow and that rapid exercise and combined leg motion would produce more improvement in venous flow in the lower extremities, compared to slow single ankle motion. This study aimed to clarify the effect of LEX by comparing changes in venous flow velocity and volume in the lower extremities, after different modes of leg exercise.
Methods
Ethical considerations
This study was carried out in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of the hospital. All participants provided written informed consent prior to completing any study-related tasks.
LEX
The LEX is a portable apparatus that enables patients to move their legs while in the supine position. It consists of metal footplates, leather soles, straps for attaching the feet to the footplates, a metal base, and suspension arms for the bedrail to provide stability while exercising (Figure 1). It allows patients to move their ankles to 30° dorsiflexion and 60° plantar flexion. In addition, both footplates are connected by a V-shaped rotating shaft with two-degrees-of-freedom dorsi–plantar flexion of the ankle and subtalar eversion/inversion. The shaft rotation allows the user’s ankle to move proximally and distally. It also allows combined flexion and subtalar eversion/inversion and enables knee flexion/extension, hip flexion/extension/internal rotation/external rotation, and combined leg motion with three joint movements.
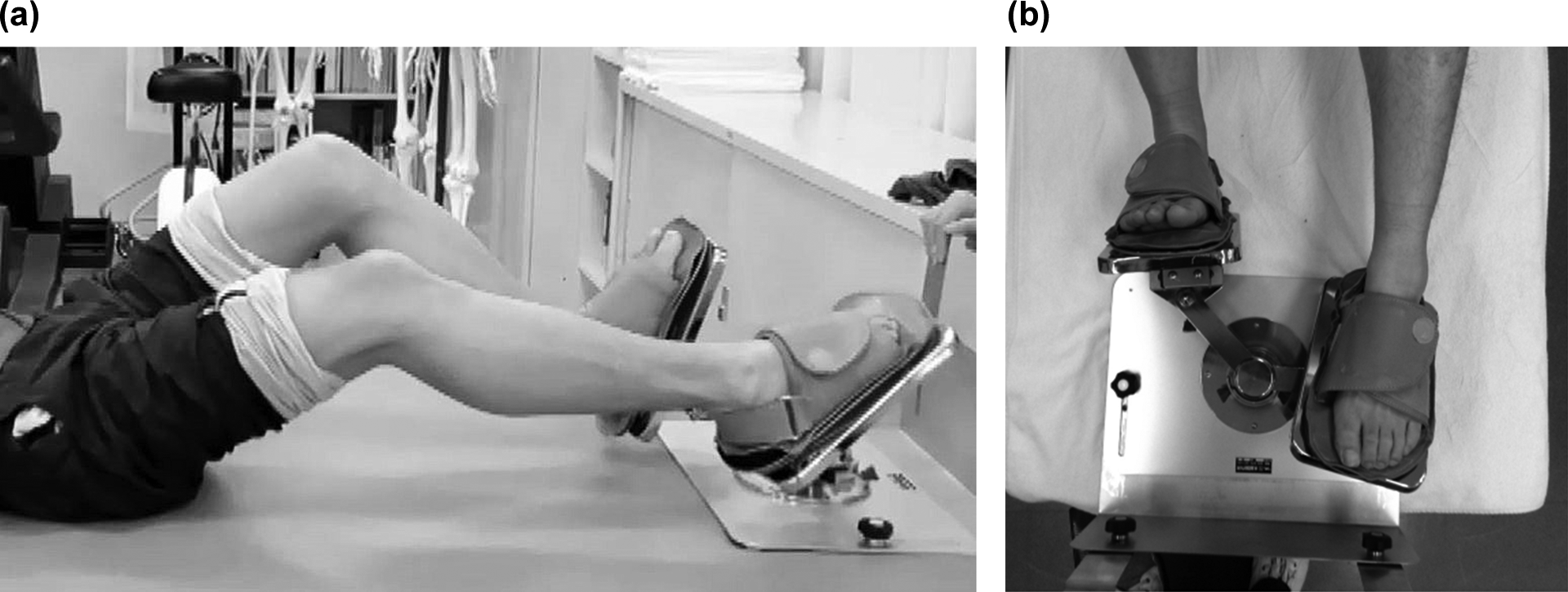
The LEX comprises metal footplates, leather protectors, and straps for fixing the foot to the footplates, axes for flexion and rotation, and a metal base. The figures show views from side (a) and above (b) of using LEX. LEX: leg exercise apparatus.
LEX can be configured for resistance exercises by adjusting the force required to push the footplates. In this study, we did not use this specific function, because our research focus involved the standard LEX functions.
Participants
We enrolled eight healthy participants (five men and three women; mean age: 21.6 ± 2.3 years, range: 19–25 years, height: 168.0 ± 9.1 cm, and weight: 59.5 ± 10.1 kg), with no history of (or risk factors for) deep vein thrombosis or lower limb operations (Table 1). Before obtaining measurements, we ruled out the presence of any thromboses using duplex ultrasonography on both legs. 24 All ultrasound examinations were performed by an experienced cardiologist using the EUB 7500 (Hitachi, Tokyo, Japan) and a 5–13-MHz linear array ultrasound transducer. Environmental conditions were maintained at a temperature of approximately 20°C and a relative humidity of 50–60%.
Data of the participants.

LEX performance and ultrasonographic examination
Participants were asked to lie down in a supine position on the examination bed and breathe quietly for approximately 60 min. Next, we obtained a full longitudinal image of the right common femoral vein in color Doppler mode. After the resting period, the participants performed 1-min LEX exercises in three modes: (1) rapid single ankle motion (maximum active ankle dorsiflexion/plantar flexion at a rate of 60 cycles/min); (2) slow single ankle motion (maximum active ankle dorsiflexion/plantar flexion at a rate of 30 cycles/min); and (3) slow combined leg motion (ankle active dorsiflexion/plantar flexion and subtalar eversion/inversion at a rate of 30 cycles/min, with natural knee extension/flexion, hip/extension, and hip internal/external rotation). Each exercise was performed with the aid of a metronome to maintain the prescribed pace.
The right femoral venous flow volume and the maximum and mean blood flow velocities were measured at 1, 10, 20, and 30 min postexercise. These measurements were repeated three times for each participant, and the order of exercises was randomly assigned. Between each session, the participants rested until blood flow returned to the resting level; this rest time was approximately 60 min. All data are presented as the ratio of measured values relative to resting level values. The methodology is summarized in Figure 2. During the measurements, all participants wore knee-length graduated compression stockings that provide pressures of 18 mmHg at the ankle and 14 mmHg at the calf (Fine support® stockings, Toray Medical, Chiba, Japan).

Flow volume and venous velocity of the femoral vein were measured at 1, 10, 20, and 30 min after the completion of active ankle motion with the LEX. The same measurements were obtained by three methods; rapid single motion (ankle dorsiflexion/plantar flexion) at a rate of 60 cycles/min, slow single motion at a rate of 30 cycles/min, and combined leg motion at a rate of 30 cycles/min. LEX: leg exercise apparatus.
Statistical analyses
Sample sizes were calculated from an earlier report, using a two-way repeated measure analysis of variance (ANOVA), with an α level of 0.05 and power of 0.80 and an effect size of 0.40. 18 Eight participants were required, allowing for dropout of two participants.
Venous flow velocity data were analyzed using a two-way, 3 × 5 ANOVA ((methods: rapid dorsiflexion/plantar flexion, slow dorsiflexion/plantar flexion, and slow combined leg motion) × (times: rest, 1, 10, 20, and 30 min)) with repeated measures across both factors. Post hoc analyses were performed using the Bonferroni comparisons test. A p-value of <0.05 was considered statistically significant. Analyses were performed using IBM SPSS Statistics version 22 (IBM Corp, Armonk, New York, USA).
Data were obtained from the same participants as reported in a previous study. 21 However, in addition to the venous flow volume analyzed in that study, we included venous flow velocities and analyzed these data using distinct statistical procedures, for this study.
Results
Figure 3(a) shows the venous flow volume as the ratio of change from baseline resting venous flow. One minute after the end of the LEX exercise, the venous flow volume increased 2.29-fold from baseline after rapid ankle dorsiflexion/plantar flexion, 1.38-fold after slow single ankle motion, and 2.03-fold after slow combined leg motion. The flow volume after rapid flexion increased compared to the levels observed after slow flexion, and the flow volume after slow combined leg motion increased compared to the levels observed after slow single ankle motion. However, differences in the longitudinal flow volume data among the three modes of exercise were not statistically significant.

The ratio of (a) venous flow volume, (b) maximum venous flow velocity, and (c) mean venous flow velocity, with respect to baseline. Data are represented as means ± SEM. One minute after using the LEX, the venous flow volume, maximum venous flow velocity, and mean venous flow velocity increased (a) 2.29-, 2.03-, and 1.03-fold; (b) 1.38-, 1.26-, and 0.9-fold; and (c) 2.06-, 1.43-, and 1.02-fold after rapid single motion, combined leg motion, and slow single motion, respectively. Statistical analysis was conducted by means of two-way repeated measure ANOVA with post hoc Bonferroni comparisons test (α = 0.05). LEX: leg exercise apparatus; ANOVA: analysis of variance; SEM: standard error of the mean.
Significant main effects of time were detected (F (4, 28) = 8.675, p < 0.001, and ηp 2 = 0.553; two-way repeated measures ANOVA, α = 0.05). After rapid single ankle motion, the flow volumes remained 1.63-fold above baseline at 30 min postexercise, and there were statistically significant differences from rest at 1 (p = 0.023), 10 (p = 0.046), 20 (p = 0.043), and 30 min (p = 0.043) on post hoc Bonferroni correction. After slow single ankle motion and slow combined motion, these values increased 1.39- and 1.53-fold, respectively, at 30 min postexercise. However, there was no significant difference between rest and 30 min after, for both modes of exercise. There was a statistically significant difference between rest and 1 min after slow combined leg exercise (p = 0.020, with post hoc Bonferroni correction).
Figure 3(b) shows the maximum venous flow velocity ratios relative to baseline. There were statistically significant differences in longitudinal flow velocity among the three exercise modes (F (2, 14) = 4.472, p = 0.031, and ηp 2 = 0.390); however, there were no statistically significant differences on post hoc Bonferroni correction. Significant main effects of time were not detected (α = 0.05), and at 30 min postexercise, the maximum venous flow velocities were maintained around baseline levels for all three modes (0.98–1.38).
Figure 3(c) demonstrates the change in mean venous flow velocity. The main effect of the methods (F (2, 14) = 4.653, p = 0.028, and ηp 2 = 0.399) and times (F (4, 28) = 4.747, p = 0.005, and ηp 2 = 0.404) was statistically significant, and there was no interaction effect between the methods and time (α = 0.05). One minute after LEX exercise, the mean venous flow velocities had increased 2.06-fold after rapid single ankle motion and 1.43-fold after slow combined leg motion. Twenty minutes after rapid single ankle motion, the mean flow velocities had increased 1.34-fold. After rapid single ankle motion, there were statistically significant differences in mean flow velocity, from rest, at 10 (p = 0.021) and 20 min (p = 0.040) postexercise. After slow combined leg motion, there was a statistically significant difference from rest at 1 min (p = 0.030 with post hoc Bonferroni correction) postexercise. At 10 min, mean venous flow velocity after rapid single ankle motion increased 1.67-fold. In contrast, after slow single ankle motion, this value decreased to below baseline (0.98-fold; p = 0.031).
Discussion
We compared the effects of three different modes of active leg exercise with LEX on venous flow in the lower extremities. We showed that rapid ankle dorsiflexion/plantar flexion with the LEX device improved femoral venous flow volume, the effect of which persisted at 20 and 30 min postexercise (for mean venous flow velocity).
Furthermore, rapid single ankle motion induced higher venous flow volume and mean velocity, compared to slow single ankle motion. However, even at a slow speed, combined leg motion involving the knee and hip exhibited an equivalent effect to that of rapid single ankle motion on flow volume and mean venous flow velocity.
McNally et al. 11 investigated the effect of 1 min of active ankle dorsiflexion/plantar flexion, at a rate of 30 cycles/min, in patients who had undergone total hip replacement. They measured the mean venous outflow using strain-gauge plethysmography and reported an increase of 22% from baseline; this value increased 12–30 min after exercise. The current study showed that even slow ankle dorsiflexion/plantar flexion LEX exercise (at the same speed used in the McNally study) improved femoral venous flow volume (increase of 39% from baseline), with persistent treatment effects at 30 min postexercise. The two other exercise methods, rapid flexion and combined leg motion, induced larger increases.
To investigate the most beneficial type and direction of ankle movement, Sochart and Hardinge 12 measured femoral venous velocity using ultrasonography during passive and active ankle movements, including dorsiflexion/plantar flexion and subtalar inversion/eversion, both independently and combined; however, they did not control for movement speed. They reported that active combined movement resulted in the largest increase in femoral venous velocity, with a 38% increase in mean velocity and a 58% increase in peak velocity during movement. In the current study, rapid active ankle dorsiflexion/plantar flexion at 60 cycles/min, slow active ankle dorsiflexion/plantar flexion at 30 cycles/min, and slow combined leg motion at 30 cycles/min, using the LEX, induced flow volume increases of 129%, 38%, and 103%, respectively, at 1 min postexercise, and 63%, 39%, and 53%, respectively, at 30 min postexercise. Although rapid exercise improved venous flow volume compared to slow exercise for a short period after LEX exercise, combined leg motion improved venous flow volume compared to slow ankle dorsiflexion/plantar flexion at the same speed. Therefore, we consider that slow combined leg exercise with LEX is effective for postoperative and bedridden patients.
Calf muscle pump function is related to chronic venous insufficiency. 25 –27 Padberg et al. 26 reported that increases in calf muscle strength and ankle mobility improve venous hemodynamics by improving calf muscle pump function. Those reports are in agreement with our hypothesis that leg exercises, completed with LEX, can improve venous flow.
According to Ohgi et al., 28 soleal vein thrombosis is an origin site of fatal pulmonary thromboembolisms. To prevent venous thrombosis in the soleus muscle, the LEX is designed to produce greater soleus muscle contraction in the knee-flexed position than during active ankle movement without LEX. The gastrocnemius muscles and the soleus muscles work on the plantar flexion of the ankle joints. When the ankle joints are plantarflexed in a knee extension position, the gastrocnemius muscles become agonist muscles, and thus, the soleus muscles may not be sufficiently contracted. Conversely, in knee flexion position, the gastrocnemius muscle, which is a biarticular muscle, is relaxed. However, the soleus muscle is a monoarticular muscle and contracts to a greater extent in knee flexion position, compared to knee extension. When patients are positioned in a bed, their knees are often extended. Therefore, we hypothesize that exercise with the LEX facilitates stronger contraction of the soleus muscle than conventional exercise approaches.
In a previous study, we measured muscle activity during active combined leg exercise at a rate of 30 cycles/min, with and without LEX, in healthy participants using surface electromyography. 19 Higher magnitude muscle activity was observed for the rectus femoris, vastus lateralis, gastrocnemius, and soleus muscles, with LEX than without LEX, based on integrated electromyogram data. Another study compared femoral venous flow in healthy participants for a period of 30 min after 1 min of exercise, at a rate of 30 cycles/min, with and without LEX. 20 After 1 min of exercise with LEX, the venous flow volume and vessel diameter at 30 min was higher than that observed at 30 min, after 1 min of exercise without LEX, in the same leg.
This study has several limitations. The first is the method for evaluating venous flow and thrombosis. We evaluated only the femoral vein using ultrasonography despite the fact that the soleal vein being is crucial for venous flow. Although duplex ultrasonography is the standard technique for measuring venous flow, the critical or clinical meaningful lower limb venous flow necessary for reducing the risk of thromboembolism is unknown. Future investigations of the incidence of thromboembolisms, including pulmonary embolisms, in clinical settings are needed. 7,15,17
The second limitation involves the influence of LEX on the cardiovascular system. We hypothesized that exercise with the LEX would induce increased cardiac output, and skeletal muscle contraction would affect lower extremity peripheral arteries, ensuring proper blood flow in the muscle. Exercise with the LEX improved venous flow in the lower extremities. Cardiac output and vital signs should be monitored during and after LEX exercises to investigate the mechanisms that improve lower extremity venous flow while using LEX.
The third limitation is the frequency of LEX exercise in clinical settings. We describe that the effects of 1 min of LEX exercise persisted for 30 min; however, it is impractical to do LEX exercise every 30 min. Therefore, we intend to establish protocols for clinical studies by referencing prior studies. 29,30 Yamashita et al., 29 reporting on patients in intensive care units, stated that the effect of 5 min of passive ankle dorsiflexion, performed by nurses at 30 cycles/min, persisted for 2 h, increased peak blood flow velocity in the femoral vein to levels that were equivalent to, or more effective than, those produced using the Intermittent pneumatic compression device (IPCD). Fuch et al. 30 reported that combined pharmacological prophylaxis and 30 min use of a passive ankle compression device, three times per day, lowered the incidence of deep vein thrombosis (DVT) compared to pharmacological prophylaxis alone. Our future protocol will consist of four sets of 5 min of combined leg motion with LEX per day. VTE prophylaxis during sleep is also needed; therefore, we intend to investigate the use of IPC during nighttime hours in addition to the use of LEX daytime hours.
The fourth limitation pertains to the age of our volunteers. Study participants were young (mean age 21.6) and healthy. On the other hand, most patients who may use LEX during the postoperative period are bedridden and/or elderly. The data obtained from the study may not apply to those elderly patients who have a higher risk of VTE. Future studies should use LEX with an elderly study cohort.
We anticipate that the LEX will improve ankle mobility in patients, thereby preventing thromboembolism and potentially motivating patients to participate in early rehabilitation. LEX is also a potential educational tool for patients and medical experts and can be used to teach the importance of active ankle movement for thromboembolism prophylaxis. In the future, we intend to study the duration of increased venous flow, after LEX, in order to design a thromboembolism prophylaxis protocol involving LEX. Furthermore, we plan to evaluate the incidence of perioperative thromboembolism in patients undergoing total hip arthroplasty, total knee arthroplasty, and spinal surgery, to evaluate the effect of LEX in preventing thrombosis in real-world clinical settings.
Conclusion
One minute of LEX exercise improved femoral vein flow volume for up to 30 min postexercise. Rapid ankle dorsiflexion/plantar flexion induced a higher flow volume and mean flow velocity than slow exercise. However, at the same speed, combined leg motion, active dorsiflexion/plantar flexion, and subtalar eversion/inversion with the knee and hip motion, induced better effects on flow volume than single ankle exercise.
The LEX is a tool for improving lower extremity venous flow through different modes of exercise in the supine position, and therefore may help prevent lower extremity deep vein thrombosis.
Footnotes
Acknowledgments
The authors would like to thank Mr. Toshiji Mizukoshi, executive adviser at Nemoto, Co., Ltd, and Mr. Tsutomu Mizukoshi, the executive managing director at Nemoto, Co., Ltd, as co-producers of LEX. They would like to thank Prof. Yasuyoshi Wadano, Director of Ibaraki Prefectural University of Health Sciences Hospital, Ms. Kyoko Nishimura, the former head nurse of Unit 530 at the University of Tsukuba Hospital, and Prof. Koichi Iwai, the former vice-president of the Ibaraki Prefectural University of Health Sciences, who assisted in the statistical analysis of the data. They would also like to thank the late Kiyoshi Eguchi, former professor of the University of Tsukuba hospital, for his generous support and warm encouragement.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by “Research Contributing to Medical Safety” of Tsukuba University Hospital, and “A-step; Adaptable and Seamless Technology Transfer Program through Target-driven R&D” from the Japanese Science and Technology Agency.