
Abstract
Purpose:
Histological architecture of normal acetabular labrum regarding free nerve endings (FNEs) and mechanoreceptors (MRs) has been satisfactorily described in the literature. However, the presence of FNEs and MRs in acetabular labrum of hip joint has been analyzed only once in patients with osteoarthritis (OA). Aim of this article is to report histological distribution pattern of FNEs and MRs in acetabular labrum of patients with severe OA, at the same time conducting a comparison with normal acetabular labrum described in the literature.
Methods:
Seven patients with severe hip OA were enrolled in this study. Patient selection was assisted by the utilization of specific clinical scales delineated by the American College of Rheumatology. After successful total hip arthroplasty, tissue samples of acetabular labra of seven patients were histologically processed and stained with the gold standard chloride method, which was subsequently examined under a compound microscope.
Results:
FNEs and MRs constituted the major histological structures. Identified MRs included Pacini corpuscles, Ruffini corpuscles, and Golgi-Mazzoni corpuscles. The presence of FNEs was predominant in the middle part of the acetabular labrum, featuring a remarkable decrease in peripheral parts. In contrast, MRs were detected basically in peripheral parts and less in the middle part.
Conclusions:
Differentiation of the distribution pattern of MRs and FNEs in acetabular labrum of hip joint is remarkable between normal patients and patients with severe OA. The abundance of FNEs in the middle part of the pathologic labrum is mainly responsible for the observed discrimination. A “conversion” of MRs to FNEs may occur during OA progression, modulating therefore this pattern as well as the upcoming clinical manifestations.
Introduction
Acetabular labrum constitutes a cartilaginous ring located in glenohumeral as well as in hip joint. It plays a fundamental role not only in stability but also in the maintenance of articular cartilage. Kim and Azuma 1 were the first to investigate and describe the significant presence of nerve endings, as well as sensory nerve and organs in the acetabular labrum, suggesting a possible involvement in proprioceptive and nociceptive mechanisms.
The connection of free nerve endings (FNEs; neuroreceptors) with the sense of pain transmit is well-known today. On the other side, mechanoreceptors (MRs) are entrusted with the detection and transmit of senses as touch (Merkel’s disks), light touch and vibration (Meissner’s corpuscles), and deep pressure and vibration (Pacini’s corpuscles, Golgi-Mazzoni corpuscles, and Ruffini corpuscles).
Acetabular labrum lesions, such as labral tears, seem to constitute an important risk factor for the appearance of osteoarthritis (OA). The term “osteoarthritis” refers to chronic inflammation of the anatomical joint elements (articular cartilage, synovial bursa, and bones), which is manifested mainly in elderly, with stiffness, pain, and possible edema.
The presence of FNEs and MRs in acetabular labrum of hip joint has been described previously. However, to our knowledge, this distribution pattern of FNEs in combination with MRs has been described only once in patients with OA. 2 One secondary study focused on the presentation of FNEs in acetabular labrum in patients with OA, within a general anatomical and clinical analysis. 3
In this study, we analyze, according to our own clinical and histological evidence, the distribution pattern of MRs and FNEs in acetabular labra of patients with OA. The study’s aim was to report the differences with the normal pattern, suggesting a pathogenetic mechanism underlying these differences as well as the upcoming symptoms of the disease.
Materials and methods
Our study took place in Amalia Fleming Hospital, Athens, Greece. All procedures performed in our study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Seven patients were finally selected, four men and three women, with a mean age of 65–70 years. All of them were initially radiographically diagnosed with grades III and IV hip OA (severe OA), according to the fundamentally established Kellgren–Lawrence (OA) grading system. 4 Radiologically, patients featured multiple to large osteophytes, definite to marked joint space narrowing, and sclerosis, which was severe in grade IV. Radiography showed furthermore possible/definite bone deformity in grade III/IV OA, respectively, as also established in Kellgren–Lawrence scale.
Except for radiological grading, specific clinical scales were also used for more accurate patient selection. These clinical scales, which contributed to better clinical evaluation, included the six-minute walk test (6MWT), the timed up and go (TUG) as well as the Arthritis Impact Measurement Scales (AIMSs). Test conduction was strictly framed by the rules and advisory guidelines of the American College of Rheumatology. Results of these tests, in combination with the radiographic evaluation, allowed the appropriate selection of the sample.
In this study, patients with low performance were candidates to participate in 6MWT. This performance was appointed by the distance of 250 m. Patients who covered a distance of more than 250 m were automatically excluded from the study. In TUG, 11 s was the exclusion limit. These two tests contributed to the functionality clinical evaluation of hip joint, assisting in the exclusion of patients with moderate to physiological joint functionality.
AIMS was included in clinical scales in order to gain a complete opinion about patient’s symptomatology and its psychological effects. Quality of life was approached by this way. After the completion of questionnaires, zero score was considered as good health status, when the total score 10–60 represented poor health status. As a subjective test, AIMS was initially not equal with 6MWT and TUG evaluated. However, our end results revealed admirable agreement between AIMS and the other used tests.
Final selection of seven patients was conducted according to these data. Radiographic Kellgren–Lawrence grade III/IV and pathological, as referred, clinical scales constituted the main participation terms. After informed written consent of all patients were obtained, they underwent a successful total hip arthroplasty.
Acetabular labrum was removed for each patient (Figure 1), obtaining multiple tissue sample from three parts of the labrum: ventral, middle, and frontodorsal (Figure 2). Labrum specimens were stored at
Removed acetabular labrum after successful total hip arthroplasty.

Acetabular labrum histological specimen parts.
Specifically, obtained tissue sections were decalcified in Borden’s ReaLemon liquid solution (88% formic acid admixed with three parts of freshly squeezed (filtered) lemon juice) for 15 min in dark. Tissues were then removed, separated from the transfused formic acid, and placed in 1% solution of gold chloride, placing the tissues again for 10 min in dark, or until its hue alteration from golden yellow to dark. Gold chloride solution was then transfused and tissues were enriched with the addition of 25% formic acid for 30 min at room temperature in dark. Formic acid solution was transfused, and the processed tissues were then washed and cleaned. 6,7 For histological staining, the tissue sections were washed two times in 70% alcohol and two times in xylene and then cover slipped.
Sections were analyzed under a light microscope (Nikon Optiphot 2, NIKON, Tokyo, Japan) connected to a PC and a camera lucida. High-resolution microscopic images were captured using a color 3CCD Sony DXC-950P (Sony Corporation, Tokyo, Japan) camera and the Scion Image program. Images were corrected with Photoshop CS5.
Results
Histological samples were examined under the optical microscope. Results were qualitatively similar across the seven patients.
FNEs and MRs were searched and identified in all samples. MRs included Pacini corpuscles, Golgi-Mazzoni corpuscles, and Ruffini corpuscles.
FNEs were identified predominantly in the middle part of the acetabular labrum of the seven patients, while their presence in the frontodorsal and ventral parts was unimportant or absent (Figure 3). FNEs were in addition more abundant in the chondral side of the labrum in comparison with the articular part.
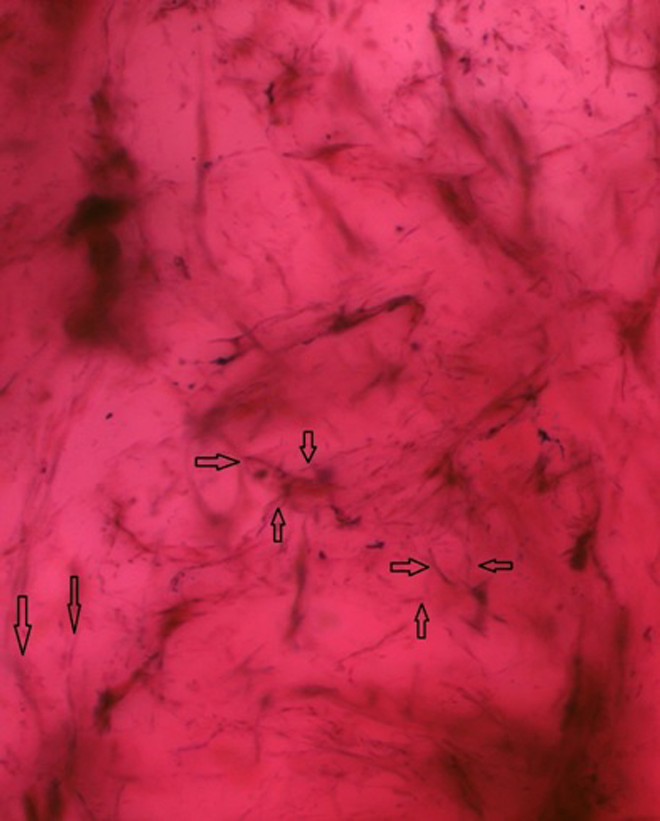
FNEs identified in the middle part of the labrum. 400× magnification. FNE: free nerve ending.
On the other side, MRs were fundamentally in the peripheral parts of the labrum detected: frontodorsal and ventral parts. In 100% of patients, one or more MRs were recognized, either in frontodorsal or in ventral part. Nevertheless, MRs were also identified in the middle part (in 71.4% (five of seven patients) and to a greater extent in comparison with the presence of FNEs in peripheral parts. Six (86%) of the seven patients were identified either Ruffini corpuscles or Golgi-Mazzoni corpuscles in the peripheral parts of the labrum (Figures 4 and 5). Pacini corpuscles were found in all patients and in all parts of the labrum (more in peripheral parts as shown in Figure 6). MRs were also found in a greater quantity in chondral side of labrum. Our data are analytically presented in Tables 1 and 2. Statistical analysis was characterized by approach in one decimal place.

Ruffini corpuscle identified in the ventral part of the labrum. 400× magnification.

Golgi-Mazzoni corpuscle identified in the frontodorsal part of the labrum. 400× magnification.

Pacini corpuscle identified in the middle part of the labrum. 400× magnification.
MRs and FNEs distribution per part of acetabular labrum.
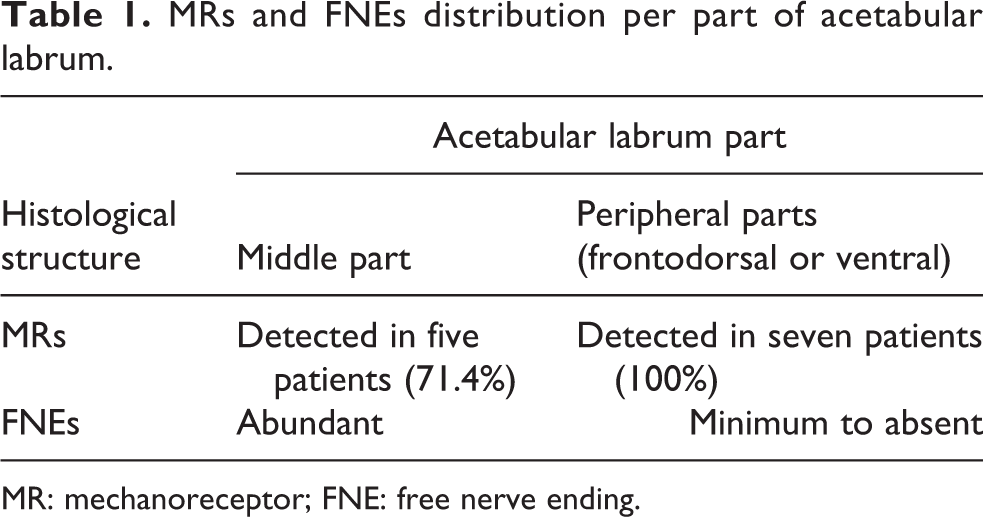
MR: mechanoreceptor; FNE: free nerve ending.
Statistical representation of MRs’ localization per type among the patients.

MR: mechanoreceptor.
Discussion
The acetabular labrum of the hip joint is described as a horseshoe-shaped anatomical structure. The labrum adheres bony and cyclically to the acetabular edge, surrounding thus the anterior, superior, and posterior portions of acetabular rim. 8 Its inferior marginal portion is merged with the transverse acetabular ligament. This ligament lies in the base of acetabular fovea, linking the anteroinferior portion (anterior horn) with the posteroinferior portion (posterior horn) of the labrum. 9 All labral portions are connected with the acetabular hyaline cartilage, 10 which articulates with the analogous articular surface on the femoral head. The labral diameters feature great variety according to each portion. The anterior and superior portion of acetabular labrum is wider than the inferior. 10,11 The superior labral portion constitutes particularly the thickest characterized by a diameter of the order of 3 mm. 12 However, many normal anatomical variations in acetabular labrum may be presented. 13
Functionally, the acetabular labrum plays a great biomechanical role primarily in the maintenance of the hip joint stability. This stability can constitute the effect of compensatory labral response to a mechanical distraction force, which may possibly occur in combination with a translation force. 14 Acetabular labrum contributes fundamentally to this stability even in the case of labral tears, featuring great impedance against the transposition of femoral head in a neutral anatomical position. 15 On the other side, it is known that femoral external rotation is also limited by the iliofemoral ligament role of labrum. 16 The stabilizing role of the labrum is therefore framed by the limitative. Except for these, it seems to play an extra protecting role in hip joint, strengthening with unknown mechanisms the production of intra-articular fluid from the synovial membrane. 17
MRs are important histological structures found in muscles, tendons, and capsules. Krause was the first to find and describe MRs. 18 Nevertheless, the first systematic classification of MRs was established by Freeman and Wyke in 1967, distinguishing four different types of MRs: type I includes Ruffini endings and Meissner’s corpuscles, type II includes Pacinian corpuscles, type III includes Golgi-Mazzoni corpuscles, and type IV includes FNEs. 19
Today it is well-known that MRs and FNEs, which represent an autonomic category, are closely related to proprioception and nociception, respectively. They are entrusted with the detection of special stimuli, transmitting them finally to cortex in the form of electrical nerve impulses, with coordination of other neurons. New nerve impulses are created in response to these afferent stimuli, running into efferent nerve fibers. These afferent and efferent nerve fibers constitute two major systems that contribute fundamentally to the synergy of movements, protecting musculoskeletal system also from injuries. 20 The presence and distribution pattern of MRs and FNEs in acetabular labrum have been described many times, with different results (Table 3).
Presence of MRs and FNEs in acetabular labrum of hip joint.

MR: mechanoreceptor; FNE: free nerve ending.
OA constitutes a degenerative disease mainly characterized by joint inefficiency. Major clinical characteristics include furthermore degeneration of articular hyaline cartilage, meniscal lesions as well as loss of stabilizing power of adjacent ligaments. 24 Nonspecific symptoms such as pain and articular stiffness constitute the hallmark of the disease. 25 The epidemiologic profile and risk factors of OA is well-defined today; heavy individual work, 25 obesity 26 , and a specific single-nucleotide polymorphism of GDF5 27 seem to be prevalent risk factors for OA appearance.
According to recent data, acetabular labrum lesions play a significant role in the pathogenesis of OA. Inversion of acetabular labrum may possibly lead to hip OA. 28 On the other side, acetabular lesions are more severe in patients with radiographic hip OA in comparison with healthy patients. 29 Aging and dysplasia of acetabular labrum may be important risk factors for acetabular labrum degeneration. 30 Degeneration of acetabular labrum may concomitantly lead to the appearance of OA.
In this study, acetabular labra of the seven patients with OA were histologically investigated, emphasizing the distribution pattern of MRs and FNEs, in order to exclude safer conclusions about its possible pathogenetic role in OA appearance. To our knowledge, histological investigation of acetabular labrum in patients with OA has been reported only twice. 2,3 However, the investigation in one of the two studies was conducted in a general research of patients with different degenerative diseases, including OA. The presence of FNEs in the acetabular labrum was decribed. 3 Specific information about MRs was reported only in one study. 2 Nevertheless, the differentiation of the distribution pattern of MRs and FNEs in patients with OA and healthy, respectively, was not highlighted in any of the studies.
In our study, the presence of FNEs was almost universal within the acetabular labrum of the seven patients, indexing with the gold standard chloride staining. The middle part of acetabular labrum demonstrated great abundance of FNEs, containing more than every other part. These data are in full agreement with the results of one study, 3 where FNEs were identified in abundance at the acetabular labrum base, featuring its decrease in the periphery. This distribution pattern is partially differentiated in the other study, 2 where FNEs are reported to be predominantly located in anterosuperior and posterosuperior labrum zones. The different acetabular labrum anatomical division is responsible for this apparent differentiation. Anatomical middle part in our study is in full correspondence with the greater portion (more than 50%) of anterosuperior and posterosuperior zones in the other division, when ventral and frontodorsal parts are related to the one portion of anterosuperior zone, including anteroinferior zone, and the one portion of posterosuperior zone, including posteroinferior zone, respectively. These different divisions influenced histological samples obtained and, subsequently, the final results. In our study, FNEs were identified in a smaller percentage in ventral and frontodorsal (peripheral parts) labrum, demonstrating a similarity in the results of the other study, where they were clearly pathologically reduced in anteroinferior and posteroinferior zones.
The distribution pattern of MRs was described only in one study. 2 The quality of identified MRs is in general similar to our study. Pacini, Golgi-Mazzoni and Ruffini corpuscles were described. However, the presence of Krause corpuscles in two specimens (in a statistical sample of 20) was also referred, which is in contrast to our results. This additional finding, which was not identified in our study, could be attributed to the small statistical sample.
MRs were, as FNEs, located predominantly in anterosuperior and posterosuperior acetabular labrum zones (100% of specimens), and in only small percentage (20–40% of specimens) in anteroinferior and posteroinferior zones. This comes in partial contrast to our results. MRs were mainly identified in peripheral labrum parts (frontodorsal and ventral parts) (100% of patients). Their presence in the middle part was nevertheless not unimportant (71.4% of patients). Differences in selected patients’ age, anatomical labrum division samples obtained, and statistical samples may be responsible for the differentiation in the reported results.
Results of our study are generally in agreement with the results of the other similar study. 2 This agreement is finally strengthened by the similar predominant location of MRs and FNEs in chondral part of the acetabular labrum. However, the different distribution pattern of MRs and FNEs between patients with end stage OA and healthy was not highlighted.
The presence of MRs in acetabular labrum of hip joint is reported by the majority of authors (Table 3). The number of MRs is drastically relatively reduced, in comparison with the number of FNEs, in acetabular labrum of patients with OA.
The etiopathogenesis of alteration in this distribution pattern is unknown. It is known that acetabular labrum contributes fundamentally to hip stability by its suctioning function in neutral hip anatomic position. 31 In this position, the middle part of the labrum is primarily loaded, leading to a remarkable mechanical wear. This biomechanical conclusion may rationalize the presence of abundant FNEs in the middle part of acetabular labrum.
Knowledge of the mechanisms of this distribution pattern alteration would help us better understand the pathogenetic mechanisms, which lead to acetabular labrum lesions and, furthermore, to OA. Based on these data, we suggest that during the subclinical progression and, finally, to the clinical appearance of OA, a conversion of MRs to FNEs may occur. This alteration would therefore be explained; finally, when OA appears clinically, this conversion leads to an increased number of FNEs, and, as a result, to a decreased number of MRs. Basic limitation of our study may be the small number of patients enrolled.
Conclusion
Histological architecture of acetabular labrum features an admirable difference between healthy individuals and patients with radiological grades III and IV hip OA. A possible conversion of MRs to FNEs may be the cause, resulting in disease progression and appearance of classical clinical manifestations. Nevertheless, further studies are required in order to accept or reject this hypothesis. Knowledge of the exact role of acetabular labrum in the pathogenesis of OA will be fundamental for clinicians, enabling better clinical evaluation and selection of appropriate treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.