
Abstract
Introduction:
Steroid and local anaesthetic injection to the acromioclavicular joint (ACJ) is a very common diagnostic and therapeutic procedure, which is often performed in the outpatient department. However, it can be difficult to localize this joint because of its small size, presence of osteophytes and variable morphology in the population. We performed a study to determine whether the use of an image intensifier (X-ray guidance), in theatre, improves the accuracy of this injection.
Methods:
This was a prospective study carried out between March 2014 and March 2015. The injections were performed by two senior orthopaedic surgeons. First, we clinically palpated the ACJ and marked the area over this point as A. Then, with the use of a needle and an image intensifier in a single plane, we identified the actual location of the ACJ and marked this point as B. We measured the distance between A and B in millimetres (mm) and determined the accuracy of the injections. Further analysis taking into account the ACJ capsular attachments was also performed.
Results:
In total, 45 patients and 50 injections were included in the study; five patients had repeated injections at different times. We found that only 12 injections (24%) were palpated to be correct with no discrepancies between A and B (95% confidence interval: 14–37%). For the remaining 38 injections (76%), the use of an image intensifier had significantly improved the accuracy of ACJ location (p < 0.05). Taking the capsular attachments of the ACJ into consideration reduced the number of inaccurate injections to 27 (54%).
Conclusion:
We recommend the use of an image intensifier (or ultrasound guidance) to accurately determine the location of the ACJ for steroid and local anaesthetic injections. This prevents an injection into the wrong place, which can lead to wrong diagnosis and/or suboptimal treatment.
Introduction
Acromioclavicular joint (ACJ) osteoarthritis is one of the underlying causes of anterior or superior shoulder pain. It is the most common disorder involving the ACJ. 1 It can be a debilitating condition commonly caused by the degeneration of the fibrocartilaginous disc within the joint. Nevertheless, patients presenting with similar shoulder pain may have other underlying causes at the same time such as impingement or rotator cuff pathology, making the diagnosis challenging. Plain film radiographs can reveal evidence of degeneration within the joints. However, the diagnosis is not solely based on plain film radiographs as similar findings may also exist in asymptomatic individuals. 2 The use of steroid and local anaesthetic injections can be useful in both diagnosis and therapy. They can help to localize the source of the pain and differentiate between ACJ and other shoulder pathology. 3
Due to a smaller joint space and variable morphology, the ACJ is difficult to identify clinically and inject accurately. This is illustrated further in cadaveric studies reporting only a success rate of 67% when injecting into this joint. 4 This can lead to a false negative result and be diagnostically and therapeutically misleading. The ACJ is routinely injected in the outpatient department with many patients reporting no improvement in their symptoms, leading to either further injections elsewhere around the shoulder girdle or expensive investigations. We believe that injection into the ACJ can be difficult without using image guidance. ACJ injections can be done under X-ray or ultrasound guidance. Few studies have demonstrated better accuracy with the use of X-ray or ultrasound guidance. 5 –7
The aim of our study was to determine whether the use of an image intensifier (X-ray guidance), in theatre, improves the accuracy of ACJ injections and to report the magnitude and direction of inaccurate injections. We also determined the accuracy of ACJ injections with a particular reference to its capsular attachments, which has not been reported before.
Methods
This was a prospective study carried out between October 2014 and March 2015 in a large district general hospital (United Kingdom). Following ethical approval (NHS REC), all adult patients with suspected or confirmed ACJ pathology were included in the study. The injections were performed by two senior orthopaedic surgeons using a standardized technique within a theatre setting. The ACJ was identified by tracing the acromion and anterior/posterior clavicle to delineate the ACJ boundaries.
We used 20 mg of Kenalog (triamcinolone) and 2 ml of 0.25% bupivacaine through a 23–25 gauge needle to provide a total injection volume of 3 ml for all patients to ensure standardization. We have found that injecting higher volumes in a small joint, which is further reduced by pathology, is not possible. First, we clinically palpated the ACJ and marked the skin over this point as A (Figure 1(a) and (b)). Then, with the use of a needle and an image intensifier in a single plane, we identified the actual location of the ACJ and marked this point on the skin as B (Figure 2(a) and (b)). We measured the distance between A and B in millimetres (mm) and determined the accuracy of the injections. Further analysis of accuracy was performed taking into consideration the ACJ capsular attachments, which on average extend 2.8 mm on the acromion and 3.5 mm on the clavicle. 8 We made the assumption that the surface anatomy was representative of the bony and capsular landmarks. Furthermore, χ 2 analysis was performed to assess the significance, if any, of introducing image guidance.

ACJ position on clinical palpation (point A). ACJ: acromioclavicular joint.

Radiograph of ACJ position on clinical palpation (point A). ACJ: acromioclavicular joint.
Following the injection, we routinely performed a clinical examination to ascertain the efficacy of the given injection.
Results
In total, 45 patients (24 males and 21 females) and 50 injections were included in the study; 5 patients had repeated injections at different times. The mean age was 51 years (range 40–85).
We found that only 12 injections (24%) were palpated to be correct with no discrepancies between points A and B (95% confidence interval (CI): 14–37%). The remaining 38 injections (76%) were misplaced laterally for 23 injections (46%) and medially for 13 injections (26%). For these 38 injections, the use of an image intensifier had significantly improved the accuracy of ACJ location on χ 2 analysis (p < 0.05). Further stratifications of these 38 injections demonstrated 20 injections (40%) were palpated to be up to 5 mm away, 16 injections (32%) between 6 mm and 10 mm away and 2 injections (4%) more than 10 mm away (Figure 3). By taking the ACJ capsular attachments into consideration, the number of inaccurate injections fell from 38 to 27 (54%). We found that 70% of patients reported pain relief following ACJ injections.

Actual position of ACJ confirmed with image guidance (point B). ACJ: acromioclavicular joint.

Radiograph of actual position of ACJ confirmed with image guidance (point B). ACJ: acromioclavicular joint.
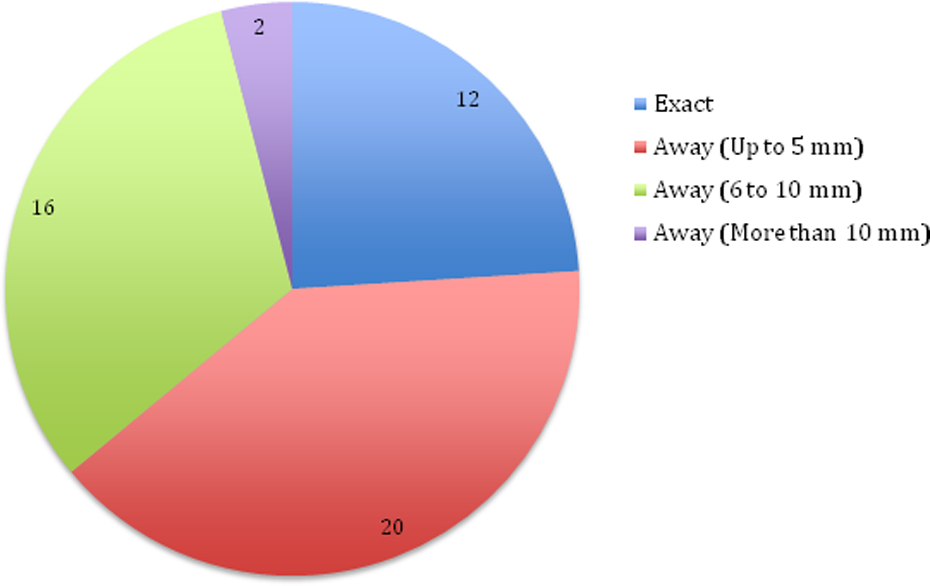
Difference in needle position between points A and B.
Discussion
ACJ osteoarthritis is a common source of shoulder pain and due to a higher prevalence of rotator cuff pathology, it is often neglected by clinicians. 9 The difficulty in establishing a diagnosis can be resolved through directly injecting a local anaesthetic into the AC joint. 3,6,9 In addition to cadaveric studies reporting rates of accurate placement of intra-articular ACJ injections in 67% of cases, in vivo studies have demonstrated lower success rates from 40% to 57%. 4,10 Therefore for diagnostic and therapeutic reasons, image guidance has been recommended to ensure accurate needle placement. 10
Fluoroscopy and ultrasound are used in clinical practice to perform ACJ injections. 6,9 Each modality has its advantages and disadvantages. Both have been shown to be more reliable than clinical palpation alone in terms of accurate placement of ACJ injections. 5 –7 Fluoroscopy is an easy modality to use but requires expensive equipment and theatre space and exposes the patient and surgeon to ionizing radiation. 7 The equipment required to perform ultrasound-guided ACJ injections is smaller, easier to manoeuvre, and does not require ionizing radiation. 6,11 However, orthopaedic surgeons will need to undergo training for using an ultrasound before they perform this procedure proficiently. If the surgeon is not trained to use the ultrasound and if theatre space is not available for fluoroscopy, then an ultrasound-guided injection performed by a radiologist should be considered.
Our study investigated the difference in terms of accurate placement of a needle in the ACJ performed through clinical palpation versus fluoroscopy. We found that in only 24% of cases, the needle was accurately placed into the ACJ using clinical palpation and this figure increased to 46% if the capsular attachments were taken into consideration. Previous studies have defined the ACJ between the boundaries of the acromion and clavicle and we have adopted the same definition. However, the capsule attaches a few millimetres away from each boundary and some experts have argued that technically an injection outside the bony boundary but within the capsule is intra-articular. Our main findings were based on bony landmarks but for completeness, we have shown that even if the zone of capsular attachments is considered blind, injections remain significantly inaccurate, and we would still recommend that all injections be placed within the joint properly and be performed under image guidance to ensure reproducibility. Inaccurate injections can lead to misinterpretation of symptoms, become painful for patients through multiple redirections of the needle to find the ACJ, and produce false negative results and subsequently suboptimal treatment. Post injection, 70% of patients reported pain relief but this would have been lower if the needle was not readjusted in the majority of cases (76%).
The importance of fluoroscopy in improving the accuracy of ACJ injection has been demonstrated in the literature. 5,7 Our study adds weight to the current evidence base and confirms that clinical palpation alone is an inaccurate and unreliable method of finding the ACJ. Therefore, we support the use of image guidance whether that be fluoroscopy or ultrasound when injecting the ACJ. Ultrasound has the value of being more practical, safer and cost effective as the patient is not subjected to theatre time or ionizing radiation but requires a learning curve to become appropriately trained.
The principal limitation of our study was to assume that skin surface markings were directly representative of the ACJ but to do it any other way, in patients, would not be possible.
Conclusion
Disorders of the ACJ are often underestimated and can be difficult to differentiate from other shoulder pathology. ACJ-specific tests have been of limited diagnostic value and plain film radiographs lack specificity to solely make the diagnosis. Steroid and local anaesthetic injections to the ACJ are a very common and useful diagnostic and therapeutic procedure. However, they have unsatisfactory levels of accuracy when using clinical palpation alone, leading to high error rates. We have demonstrated that up to 76% of ACJ injections may miss the joint if performed by palpation alone, and, even if the capsular attachments are considered, the figure of 54% remains unacceptably high. Therefore, we recommend the routine use of image guidance to accurately determine the location of the ACJ for all injections. This prevents an injection into the wrong place, which can lead to wrong diagnosis and/or suboptimal treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.