
Abstract
Purpose:
The postoperative protocol after arthroscopic rotator cuff repair (ARCR) is still controversial. Some surgeons recommend slower rehabilitation in order to improve the integrity of the repair, while others prefer early range-of-motion (ROM) exercise to avoid postoperative stiffness. The purpose of this study was to determine target ROM (T-ROM) measurements at 3 months after ARCR that are predictive of eventual full recovery without structural failure.
Methods:
The cases consisted of 374 shoulders in 360 patients who underwent primary ARCR and were followed up for at least 2 years. Forward flexion (FF) and side-lying external rotation (ER) were measured preoperatively at 3, 6, 9, 12, and 24 months after surgery, and the patients were divided into six subgroups according to the values for each type of ROM at 3 months (ROM-3M). In each subgroup, the final ROM at 24 months after surgery was compared to determine the T-ROM. The average ROMs with time and re-tear rate were then compared between the under-T-ROM and over-T-ROM groups.
Results:
The only significant difference in FF was between the 120–129° and 110–119° ROM-3M groups. Therefore, the T-ROM for FF was determined to be 120°. Similarly, the T-ROM for ER was determined to be 20°. Each ROM in the over-T-ROM group was significantly better than that in the under-T-ROM group at all assessments. There was no significant difference in the re-tear rate between the groups.
Conclusion:
To acquire sufficient ROM in 2 years without high re-tear rate, a target FF of 120° and ER of 20° should be achieved within 3 months after surgery.
Keywords
Introduction
Arthroscopic rotator cuff repair (ARCR) has undergone considerable advances over the last decade and has achieved excellent results. 1 –3 Although ARCR with double-row fixation has a lower re-tear rate than single-row fixation or transosseous fixation because of the large contact area between the repaired tendon and the footprint, 1 ARCR with single-row fixation has also been reported to allow more rapid recovery and rehabilitation than that achieved by an open procedure. 2 Therefore, both ARCR techniques have shown excellent results in terms of clinical outcome. 3
However, various complications of this procedure have also been reported. 4 –6 Persistent stiffness is recognized as one of the most common complications after ARCR. 4 Although loss of shoulder mobility after ARCR has been widely discussed, the relationship between shoulder mobility in the early stage and final stiffness is poorly understood, and there is ongoing debate regarding post-ARCR treatment protocols. Several authors have reported that excessive range-of-motion (ROM) exercise in the early stage causes structural failure. 7,8 The importance of rehabilitation in the first 3 months after surgery for return to activities of daily living 9 and tissue healing 10 has been stressed. Thus, we believe that appropriate postoperative rehabilitation, especially in the early postoperative stage, is critical to achieving good results. Therefore, we hypothesized that the final outcomes of surgery could be predicted based on ROM during the early postoperative period, and we investigated the utility of this benchmark of ROM at 3 months (ROM-3M).
Methods
Patient selection
From January 2005 through February 2010, 624 consecutive shoulders in 603 patients in whom conservative treatment was unsuccessful underwent arthroscopic primary rotator cuff repair performed by the senior author. The inclusion criteria were primary rotator cuff repair and a final functional evaluation at a minimum of 2 years postoperatively. Other major associated pathology that would require alternative treatment modalities at the time of arthroscopic surgery, such as Bankart lesion repair and augmentation because of massive retracted irreparable tears, was excluded (99 shoulders in 95 patients). Another five shoulders in five patients with isolated subscapularis tendon tears were also excluded. Thus, 520 shoulders in 503 patients met the inclusion criteria. Of these, 146 shoulders in 143 patients were lost to follow-up before a period of 2 years after surgery was reached. Finally, the study included 374 shoulders in 360 patients who were followed up for a mean of 29.6 ± 9.7 (range: 24–80) months with an overall follow-up rate of 71.9% (374 of 520 shoulders; Figure 1). The patients comprised 218 men and 156 women; mean age was 61.8 ± 10.9 (range: 25–88) years at the time of surgery. The surgery was performed in the dominant extremity in 254 patients (67.9%) and in the nondominant extremity in 120 patients (32.1%). Preoperative tear size was assessed during arthroscopic surgery. There were 324 full-thickness tears, comprising 115 small (<1 cm in length), 105 medium (1–3 cm), 99 large (3–5 cm), and 5 massive (> 5 cm) tears, and 50 partial-thickness tears (11 on the articular side, 37 on the bursal side, and 2 that were intratendinous).

Flow chart showing patient enrolment and follow-up.
Surgical procedure
All procedures were performed with the patient under general anesthesia in the beach chair position. A posterior portal and an anterior portal were established for initial assessment and treatment of the glenohumeral joint. The arthroscope was then redirected into the subacromial space. An anterolateral portal and a posterolateral portal were also established. In all cases, subacromial decompression was carried out. We performed double-row fixation for a full-thickness tear and single-row fixation for a partial-thickness tear. For the double-row fixation procedures, after the medial row of metal suture anchors loaded with no. 2 permanent sutures was inserted, the suture was passed through the medial portion of the rotator cuff in a mattress fashion. Next, lateral row suture anchors were inserted at the lateral ridge of the greater tuberosity, and the sutures for the lateral row were placed through the lateral margin of the cuff. Knot tying for the lateral row was performed first and then for the medial row. For the single-row fixation procedures, suture anchors were inserted at the lateral ridge of the greater tuberosity, and the suture was passed through the lateral edge of the cuff in a simple fashion, followed by knot tying.
Postoperative protocol
The shoulders were immobilized for 3 weeks using a sling immobilizer (for small to medium full-thickness tears and for partial-thickness tears) and an immobilizer with an abduction pillow (about 20° of abduction, for large to massive tears). In all cases, isometric cuff exercise and relaxation of muscles around the shoulder girdle were initiated on the day after surgery. After 3 weeks, passive exercise was initiated, avoiding provocation of pain. Six weeks after surgery, the patients started strengthening exercises of the rotator cuff and were permitted to practice light sports activities by 3 months postoperatively. After 6 months, full return to sports and heavy labor were allowed.
Patient assessment
A standard history was taken and a physical examination was performed in all patients. Magnetic resonance imaging (MRI) scans were acquired on the affected side in all cases to confirm a defect in the tendinous portion of the rotator cuff. The size and pattern of the tear were determined on diagnostic arthroscopy.
All patients were assessed by a single examiner for ROM, including forward flexion (FF) and side-lying external rotation (ER), at 3, 6, 9, 12, and 24 months postoperatively. The patients were divided into six subgroups for each plane on the basis of the values obtained at 3 months after surgery as follows: FF1 (<109°), FF2 (110–119°), FF3 (120–129°), FF4 (130–139°), FF5 (140–149°), and FF6 (>150°) and ER1 (<9°), ER2 (10–19°), ER3 (20–29°), ER4 (30–39°), ER5 (40–49°), and ER6 (>50°). The final ROM analyses at 24 months after surgery were compared with the ROM-3M of each subgroup in order to determine the target ROM (T-ROM). The patients were then divided into groups on the basis of ROM-3M (under-T-ROM (FF− and ER−) and over-T-ROM (FF+ and ER+)), and sex, mean age, preoperative tear size, presence of diabetes, and possession of worker’s compensation insurance were compared between the groups. The average ROM values in each group were also compared over time. In the over-T-ROM (FF+ and ER+) and under-T-ROM (FF− and ER−) groups, the final ROMs were compared between preoperative stiff cases (FF < 120° and ER < 20°) and the other cases (FF ≥ 120° and ER ≥ 20°). Furthermore, MRI was performed 1 year after surgery, and findings were classified according to the system proposed by Sugaya et al. 11 Types IV and V were considered to be re-tears. The re-tear rates were compared between the under-T-ROM and over-T-ROM groups.
Statistical methods
The final ROM achieved was compared between the subgroups (FF 1–6 and ER 1–6) using the Steel–Dwass test. Student’s t test was used to compare the ROM in the under-T-ROM groups with that in the over-T-ROM groups over time. Mann–Whitney U test was used for comparisons of patient age and final ROM between preoperative stiff cases and other cases in the over-T-ROM and under-T-ROM groups. The χ2 test was used for comparison of sex, preoperative tear size, presence of diabetes, possession of worker’s compensation insurance, and re-tear rates between the groups. A p value of <0.05 was considered to be statistically significant for all tests.
Results
Determination of the T-ROM
Thirty-seven shoulders were classified as FF1, 25 as FF2, 39 as FF3, 41 as FF4, 42 as FF5, and 190 as FF6 (Table 1, a). The final ROM was 158 ± 16° for FF1, 161 ± 11° for FF2, 166 ± 11° for FF3, 168 ± 6° for FF4, 168 ± 7° for FF5, and 171 ± 5° for FF6. The only adjacent groups with significantly different values were FF2 and FF3 (p = 0.016; Figure 2). Therefore, the T-ROM of FF was determined to be 120°.
Subgroup distributions.
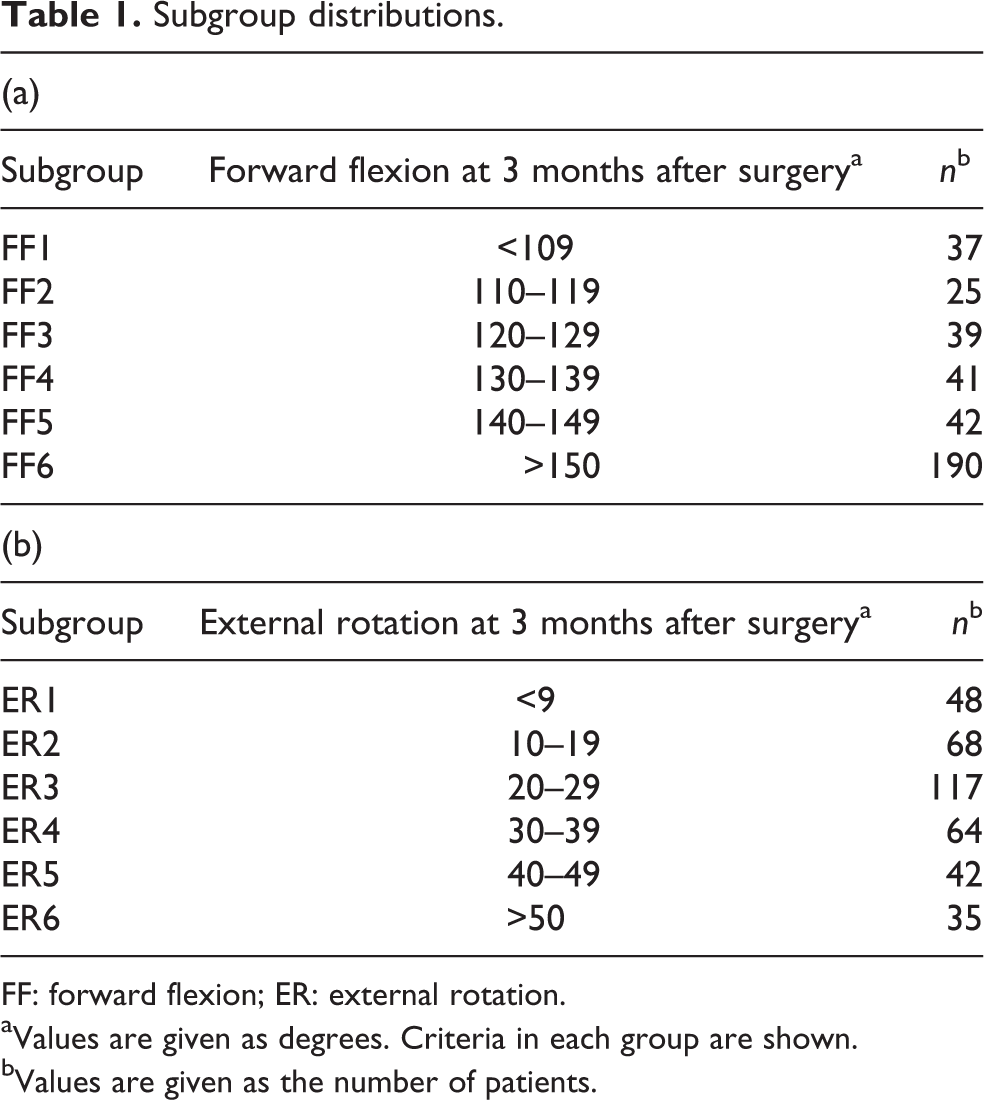
FF: forward flexion; ER: external rotation.
aValues are given as degrees. Criteria in each group are shown.
bValues are given as the number of patients.
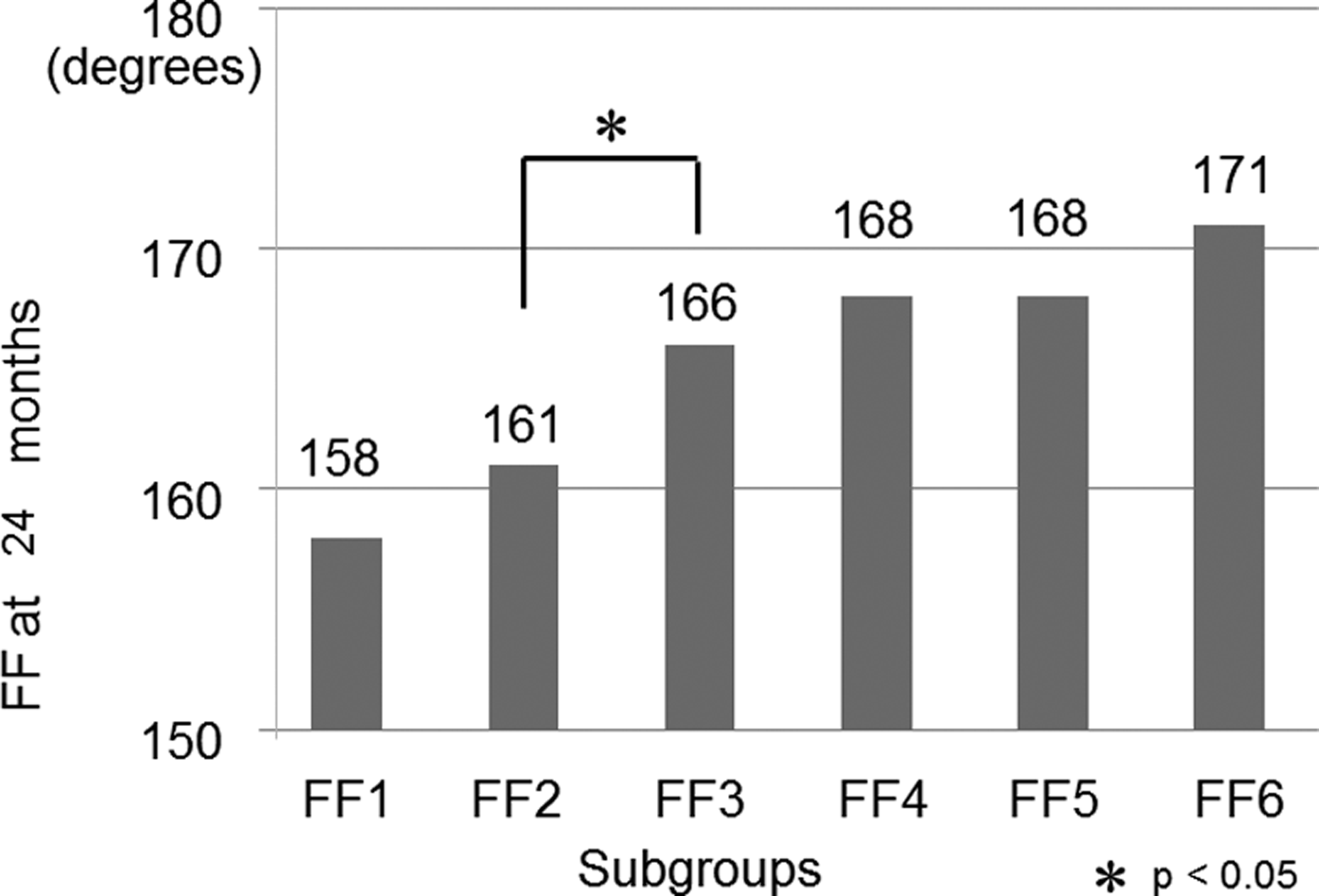
Final FF values at 24 months after surgery by subgroup according to FF values at 3 months after surgery. The only adjacent groups with significantly different values were groups FF2 and FF3. FF: forward flexion.
Forty-eight shoulders were classified as ER1, 68 as ER2, 117 as ER3, 64 as ER4, 42 as ER5, and 35 as ER6 (Table 1, b). The final ROM was 33.5 ± 16.8° for ER1, 43.3 ± 15.5° for ER2, 52.6 ± 11.9° for ER3, 54.6 ± 9.9° for ER4, 58.3 ± 10.8° for ER5, and 59.3 ± 8.8° for ER6. Significant differences were seen between the ER1 and ER2 groups (p = 0.003) and between the ER2 and ER3 groups (p = 0.000; Figure 3). Although significant differences were detected between the two adjacent groups, it should be appreciated that many outliers were included in the ER1 group at 3 months compared with ER2. Therefore, the T-ROM for ER was determined to be 20°.

Final side-lying ER values at 24 months after surgery by subgroup according to ER values at 3 months after surgery. Significant differences were seen between groups ER1 and ER2 and groups ER2 and ER3. ER: external rotation.
Demographic data and comparison of ROM improvement between the under-T-ROM and over-T-ROM groups
There were 62 shoulders in the FF− group (<119°) and 312 shoulders in the FF+ group (≥120°). Mean patient age was significantly higher in the FF− group than in the FF+ group (p = 0.001). However, there was no significant difference with regard to sex, preoperative tear size, presence of diabetes, or possession of worker’s compensation insurance (Table 2). ROM in the FF+ group was significantly better than that in the FF− group during the postoperative course (Figure 4).
Preoperative patient clinical and demographic data classified according to target FF.
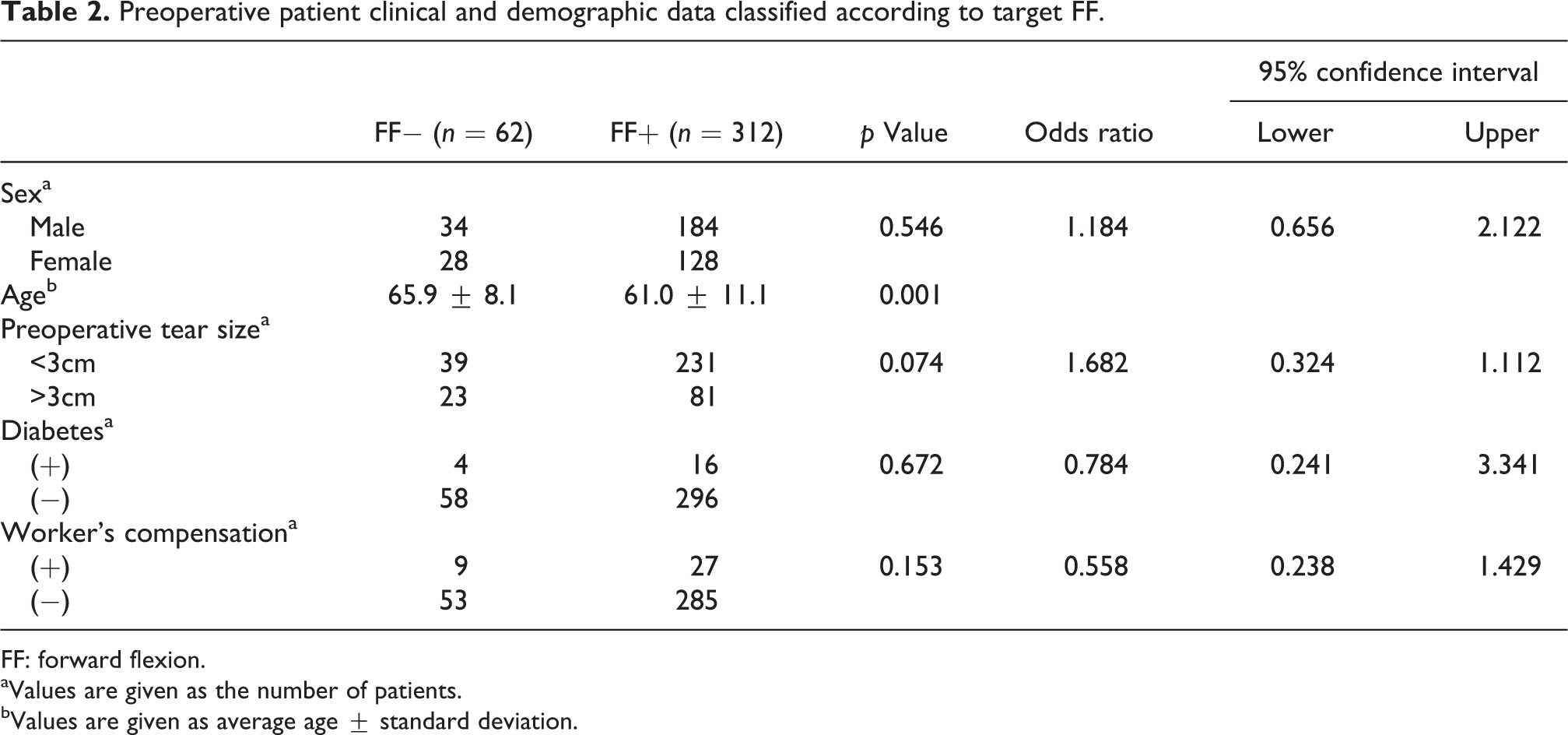
FF: forward flexion.
aValues are given as the number of patients.
bValues are given as average age ± standard deviation.
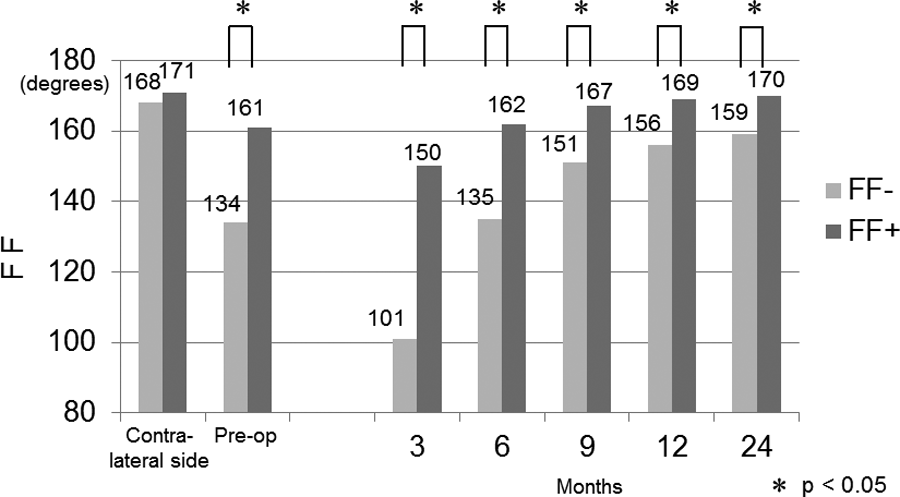
Comparison of FF progress from 3 to 24 months after surgery. Patients were divided into two groups: less than the target range of motion (T-ROM) (FF−) and more than the T-ROM (FF+). ROMs in the FF+ group were significantly better than those in the FF− group during the course. FF: forward flexion; T-ROM: target ROM; ROM: range of motion.
There were 116 shoulders in the ER− group (<19°) and 258 shoulders in the ER+ group (≥20°). Mean age was significantly higher in the ER− group than in the ER+ group (p = 0.024). There was also a significant difference in the sex distribution between the groups (p = 0.016, odds ratio 1.718, 95% confidence interval 1.076–2.740). However, there were no significant differences with regard to preoperative tear size, presence of diabetes, or possessing worker’s compensation insurance (Table 3). ROM in the ER− group was significantly inferior to that in the ER+ group throughout the study period (Figure 5).
Preoperative patient clinical and demographic data classified according to target ER.

ER: external rotation.
aValues are given as the number of patients.
bValues are given as average age ± standard deviation.
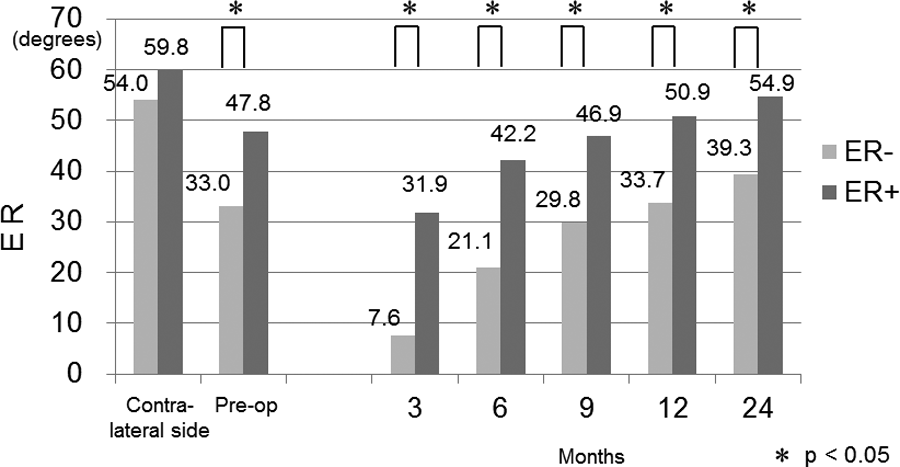
Comparison of ER progress from 3 to 24 months after surgery. Patients were divided into two groups: less than the T-ROM (ER−) and more than the T-ROM (ER+). ROMs in the ER− group were significantly inferior to those in the ER+ group throughout the study period. ER: external rotation; T-ROM: target ROM; ROM: range of motion.
Comparison of final ROM with regard to preoperative ROM between the under-T-ROM and over-T-ROM groups
Of the 40 shoulders with a preoperative FF < 119°, 22 (55.0%) were FF− and 18 (45.0%) were FF+. Of the 334 shoulders with a preoperative FF ≥ 120°, 40 (12.0%) were FF− and 294 (88.0%) were FF+ (p = 0.000, odds ratio 8.983, 95% confidence interval 4.165–19.316; Table 4). Of the 32 shoulders with a preoperative ER < 19°, 23 (71.9%) were ER− and 9 (28.1%) were ER+. Of the 342 shoulders with a preoperative ER ≥ 20°, 93 (27.2%) were ER− and 249 (72.8%) were ER+ (p = 0.000, odds ratio 6.842, 95% confidence interval 2.904–17.336; Table 5).
Ratio of FF− and FF+ according to preoperative ROM.

FF: forward flexion; ROM: range of motion.
aValues are given as the number of patients.
bValues are given as the number of patients (percentage).
Ratio of ER− and ER+ according to preoperative ROM.

ER: external rotation; ROM: range of motion.
aValues are given as the number of patients.
bValues are given as the number of patients (percentage).
In contrast, in the FF− group, the mean final FF in the 22 shoulders with a preoperative FF < 119° was 156 ± 15° and that in the 40 shoulders with a preoperative FF ≥ 120° was 161 ± 14° (p = 0.109). In the FF+ group, the mean final FF in the 18 shoulders with a preoperative FF < 119° was 169 ± 4° and that in the 294 shoulders with a preoperative FF ≥ 120° was 170 ± 7° (p = 0.239). In the ER− group, the mean final ER in the 23 shoulders with a preoperative ER < 19° was 36.7 ± 18.9° and that of the 93 shoulders with a preoperative ER ≥ 20° was 39.9 ± 16.3° (p = 0.493). In the ER+ group, the mean final ER of the 9 shoulders with a preoperative ER < 19° was 53.3 ± 10.0° and that of the 249 shoulders with a preoperative ER ≥ 20° was 55.0 ± 11.2° (p = 0.692). There were no significant differences in any of these cases.
Comparison of re-tear rate between under-T-ROM and over-T-ROM shoulders
A total of 326 shoulders underwent MRI at 1 year after surgery (50 cases in the FF− group, 276 in the FF+ group, 102 in the ER− group, and 224 in the ER+ group). Using the system devised by Sugaya et al., 11 177 shoulders were classified as type I, 96 as type II, 25 as type III, 15 as type IV, and 13 as type V. Considering types IV and V as re-tears, 28 shoulders (8.6%) were cases of re-tear, 7 (14%) of which were FF− and 21 (7.6%) were FF+ (p = 0.138, odds ratio 0.506, 95% confidence interval 0.193–1.500); 12 (11.8%) of these cases were ER− and 16 (7.1%) were ER+ (p = 0.167, odds ratio 0.577, 95% confidence interval 0.245–1.397; Table 6).
Re-tear of rotator cuff in each group at 1 year after surgery.

MRI: magnetic resonance imaging; FF: forward flexion; ER: external rotation.
aValues are given as the number of patients.
bValues are given as the number of patients (percentage).
Discussion
Persistent stiffness is one of the most frequent complications after ARCR. The risk factors for this have been reported to be diabetes, 12 preoperative stiffness, tear size, 13 adhesive capsulitis, single-row repair, age < 50 years, and possession of worker’s compensation insurance. 5 Regardless of the risk factors, postoperative rehabilitation is important in order to avoid postoperative stiffness. Namdari et al. reported that patients with limited motion at 3 months after rotator cuff repair had significantly more pain and lower outcome scores than those without limitation of motion, although not all these patients underwent arthroscopic surgery. 14 On histological analysis, Sonnabend et al. reported that the Sharpey’s fibers attaching bone to tendon were not present in any considerable amount before 12 weeks after surgery in a primate model. 15 These studies suggest that early postoperative care, especially within the first 3 months after surgery, might be important both for preventing unfavorable clinical outcomes and for achieving better structural integrity.
However, the rehabilitation protocol in the early stage after surgery is still controversial. 16 –21 Arndt et al. randomized 100 patients who underwent arthroscopic repair of a non-retracted supraspinatus tear to either immediate passive motion or strict immobilization for 6 weeks. They reported significantly better functional results, including for passive ER, passive anterior elevation, and constant score, in patients with immediate passive motion than in those with immobilization during a mean follow-up period of 15 months. The integrity of the repaired tendons seemed to be slightly better with immobilization, but there was no statistically significant difference in this regard between the groups. 16 However, in a similar study, Keener et al. divided 124 patients who underwent arthroscopic repair of full-thickness rotator cuff tears measuring <30 mm into two groups, one participating in a traditional rehabilitation program with early ROM exercise and the other undergoing 6 weeks of immobilization with delayed ROM exercise. They reported that active elevation and ER were better in the traditional rehabilitation group at 3 months but that functional scores, active motion, and shoulder strength were not significantly different between the two groups at later time points. 17 Other authors have reported that immobilization is necessary immediately after surgery and that postoperative physiotherapy after the immobilization period should be performed gently and without forceful passive ROM exercise. 11,18
During the early stage, aggressive motion may increase the possibility of anatomic failure at the site of repair in the cuff. 7,8 Lee et al. compared patients who underwent an aggressive rehabilitation protocol (manual therapy and unlimited self-passive stretching exercise) with those who underwent a limited rehabilitation protocol (limited continuous passive motion and limited self-passive exercise) after ARCR. They reported that the re-tear rate was 23.3% in the aggressive rehabilitation group and 8.8% in the limited rehabilitation group and recommended gentle rehabilitation in the early stage after ARCR from the viewpoint of tendon healing. 8 Consequently, it is thought that the aggressive rehabilitation protocol in their study represents excessive exercise. Therefore, it might be important to set a T-ROM at 3 months after surgery that does not cause structural failure. In the present study, achievement of the T-ROM at 3 months is not a risk factor for re-tear, so is not considered an excessive target of rehabilitation.
The results of this study suggest that if T-ROMs (120° for FF and 20° for ER) are reached 3 months after surgery, sufficient ROM will be acquired in 2 years. Moreover, because ROM in the under-T-ROM groups (FF− and ER−) was inferior to that in the over-T-ROM groups (FF+ and ER+) throughout the follow-up period, achievement of T-ROMs at 3 months after surgery may be essential for acquiring better ROMs 2 years postoperatively. However, even if rehabilitation was performed using a similar protocol, there were cases that would be classified as under-T-ROM at 3 months after surgery because of physical and mental idiosyncrasies, such as lack of mobility of the thorax and/or thoracic vertebra. Nevertheless, even in such cases, forceful rehabilitation should be restricted from the point of view of avoiding structural failure, because the bone–tendon junction would not be histologically mature even at 12 weeks after surgery. 15 In this study, the re-tear rate was higher in under-T-ROM cases than in over-T-ROM cases, albeit not significantly so. It is possible that the under-T-ROM cases underwent relatively forceful rehabilitation until 1 year after surgery. In such cases, an earlier MRI should be carried out in order to assess the integrity of the cuff, and forceful exercise is not recommended. Instead, measures such as increasing the frequency of rehabilitation sessions and, if needed, pain control by subacromial corticosteroid injection 22 might be needed.
In this study, preoperative tear size, presence of diabetes, and possession of worker’s compensation insurance were not risk factors for inadequate ROM-3M, and patient sex was only partially related to ROM-3M. Conversely, it is considered that the final ROM values in patients with preoperative stiffness will be lower than those in others. We found that the rate at which shoulders with a preoperative FF < 119° were classified as FF− was significantly higher than that for shoulders that had a preoperative FF ≥ 120°. Similarly, the percentage of shoulders with a preoperative ER < 19° that were classified as ER– was significantly higher than that for shoulders with a preoperative ER ≥ 20°. However, in this study, there were no significant differences in the final ROM values between shoulders with preoperative stiffness and the other shoulders in either of the over-T-ROM groups (FF+ and ER+). Therefore, even in shoulders with preoperative stiffness, provided that the T-ROM is achieved at 3 months after surgery, the final ROM can eventually be equivalent to that in shoulders with no preoperative stiffness. Similarly, even in cases with no preoperative stiffness, if the T-ROM cannot be reached, a good final ROM is difficult to achieve. Thus, even in shoulders with preoperative stiffness, it is important to achieve the T-ROM at 3 months after surgery. However, as with under-T-ROM cases after 3 months, it might be necessary to make an effort during rehabilitation to reach T-ROM within the first 3 months after surgery, such as providing more frequent rehabilitation sessions and subacromial corticosteroid injections.
There are several limitations to this study. First, a subjective measuring method was used to assess ROM but was performed by a single examiner. Second, almost 28% of the patients were lost to follow-up. MRI was not performed in all cases for various reasons, such as patient refusal. It is generally thought that patients who progress well are more likely to refuse postoperative MRI and then be lost to follow-up. This may have introduced a degree of bias into our study. Third, MRI was performed 1 year after surgery, so the incidence rate of re-tear within 3 months after surgery is unknown. Finally, according to the patient demographic data, the mean patient age in the under-T-ROM groups (FF− and ER−) was significantly higher than that in the over-T-ROM groups (FF+ and ER+), and a significant difference in sex distribution was also seen between the ER− and ER+ groups. This may have been another source of bias in this study.
Conclusions
To acquire sufficient ROM in 2 years, T-ROMs (120° for FF and 20° for ER) should be reached 3 months after surgery. Each ROM in the under-T-ROM groups was inferior to that in the over-T-ROM groups throughout the follow-up period. In this study, achievement of T-ROM at 3 months was not identified as a risk factor for structural failure.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.