
Abstract
Purpose:
Developmental dysplasia of the hip (DDH) presents a considerable surgical challenge in total hip arthroplasty (THA). Although the usefulness of computed tomography (CT)-based navigation in cup alignment has been reported, few reports have evaluated three-dimensional (3-D) cup positioning against the acetabulum specifically in patients with DDH. The purpose of this study was to evaluate the efficacy of a CT-based navigation system for alignment and spatial positioning of the cup in THA for patients with DDH.
Methods:
We reviewed 174 DDH THA cases in which CT-based navigation was used, and 75 cases in which a mechanical guide was used as a control group. Postoperative cup alignment and spatial positioning were evaluated by superimposition of a 3-D cup template onto the actual implanted cup using postoperative CT images, with pelvic coordinates matching the preoperative planning.
Results:
The proportion within the combined target zone (inclination and anteversion) was 97.7% in the navigation group and 61.3% in the non-navigation group. The mean absolute error between the intraoperative record and the postoperative measurement was 1.5° ± 1.3° for inclination and 2.1° ± 1.8° for anteversion in the navigation group. For acetabular cup positioning, the mean discrepancy between the preoperative planning and the postoperative measurements was 1.9 ± 1.6 mm on the transverse axis, 2.8 ± 2.3 mm on the longitudinal axis, and 1.7 ± 1.3 mm on the sagittal axis.
Conclusion:
THA using a CT-based navigation system achieved quite high accuracy of cup alignment angles and spatial cup positioning in primary THA for patients with DDH.
Introduction
Total hip arthroplasty (THA) in patients with osteoarthritis (OA) secondary to developmental dysplasia of the hip (DDH) presents a great surgical challenge because of the acetabular and femoral deformities, superolateral subluxation, and leg length discrepancy. 1,2 Regarding cup implantation for DDH, it is difficult to decide on the appropriate target point for acetabular reaming and cup placement because of the typical deformities present, which include an inadequate acetabular roof, a double acetabular floor, and a variety of osteophytes at the acetabular rim. 1,3 Optimal cup alignment is important in THA for achieving the maximum possible range of motion at the hip, which enables the patient to perform better in activities of daily living postoperatively, and for obtaining successful results. 4,5 Malpositioning of the acetabular cup has been associated with increased rates of dislocation, 6,7 impingement, 8,9 pelvic osteolysis, 10 acetabular migration, 6 leg length discrepancy, and polyethylene wear. 5,6 Moreover, acetabular cup positioning is an important consideration. Despite cup alignment appearing acceptable on anteroposterior views on plain X-ray, we sometimes encounter cases of incorrect cup positioning with destruction of the anterior or posterior wall of the acetabulum, which can be detected by three-dimensional (3-D) evaluation using computed tomography (CT).
Historically, the placement of the acetabular cup during surgery was performed using the freehand technique or a mechanical guide; however, the accuracy of these methods is not reliable. 11,12 Further, it is difficult to know precisely how the patient’s pelvis is oriented when in the lateral decubitus position, and this may also lead to incorrect cup placement when using a mechanical guide or the freehand technique. 13 Using a navigation system, the surgeon can ream the acetabulum and insert the cup more precisely regardless of pelvic orientation with real-time monitoring of cup alignment and location intraoperatively. 4,5 However, relatively few studies have evaluated the benefits of using a navigation system for both alignment of the acetabular cup and cup positioning on 3-D axes in the pelvis of a patient with DDH.
The purpose of this study was to assess the efficacy of CT-based navigation for cementless cup implantation in THA for patients with DDH categorized by the Crowe classification by comparing the placement of the acetabular cup with and without the navigation system and by evaluating the accuracy of the cup alignment angles and spatial cup positioning using CT images.
Materials and methods
This study was approved by the institutional review board at our institution (the approval number: 1627). In accordance with the requirements of a retrospective review, we informed the research contents by posting the documents on the bulletin board in our institution and written consent from each case was not required. We retrospectively reviewed 214 hips in 178 consecutive Japanese patients who underwent cementless primary THA with 3-D templates used for preoperative planning and navigation (CT-based hip navigation system, version 1.0 and 1.1 software, a Cart I system and a FP5000 camera, or a Cart II system and a P6000 camera; Stryker Navigation, Freiburg, Germany) of cup placement during surgery in our department between August 2008 and July 2014 (navigation group). All patients underwent postoperative CT examination. We excluded 10 hips with primary OA, 24 hips with osteonecrosis of the femoral head, and 6 hips with rheumatoid arthritis, leaving 174 hips with DDH available for further analysis in the navigation group. We also retrospectively reviewed 94 hips in 84 consecutive patients who underwent cementless primary THA without the use of a navigation system between January 2006 and July 2008 (non-navigation group). The non-navigation group consisted of 80 hips with DDH, 4 hips with primary OA, 6 hips with osteonecrosis of the femoral head, and 4 hips with rheumatoid arthritis. Five hips that did not undergo postoperative CT were excluded, leaving 75 hips with DDH for the analysis. All DDH cases were categorized using the Crowe classification and underwent implantation of a cementless acetabular cup. 14 A Trident cup (Stryker Navigation) was used in 163 hips, a TriAD cup (Stryker Navigation) in 59 hips, a Tritanium cup (Stryker Navigation) in 15 hips, and a Trilogy cup (Zimmer Biomet, Warsaw, Indiana, USA) in 12 hips.
For preoperative planning of THA with navigation, CT images were taken from the iliac wing to the femoral condyle using a helical CT scanner (Aquilion 16; Toshiba Medical Systems, Tokyo, Japan). Slice thickness of 1 mm and pitch of 2.0 mm were used. The data were transferred to the 3-D template workstation to determine the optimal size, angle, and position of the cup. To determine the pelvic plane, eight reference points on the pelvis (bilateral anterior superior iliac spines, bilateral pubic tubercles, the most distal points of the bilateral ischia, mid pubic symphysis, and sacral midplane) were taken. The pelvis has two major reference planes, namely, the anterior pelvic plane (APP) and the functional pelvic plane (FPP). The APP is defined by both the bilateral anterior superior iliac spines and pubic tubercle and the FPP is the condition of the pelvis being in the supine position on the CT scan table with adjustment of the rotation until the bilateral anterior iliac spines touch the same horizontal plane. We used FPP as a reference plane in our preoperative planning and navigation surgery. 15 The size and position of the cup were determined to acquire maximal contact with the remaining host bone. Murray et al. reported three sets of cup alignment definitions: anatomic, radiographic, and operative inclination and anteversion angles. 16 Basically, the records from the CT-based navigation system were anatomic angles, and we used Murray’s equation to calculate the cup alignment angles for these three sets of cup alignment definitions. We set the acceptable range of cup alignment at 30–45° for radiographic inclination and 5–25° for radiographic anteversion based on standards from previous reports. 17 Our principal targets for acetabular cup alignment were an anatomic inclination of 40° and anatomic anteversion of 20°, which corresponds to a radiographic inclination of 38.3° and anteversion of 12.7°. These cup alignment angles are almost at the center of the target zone. In some cases, we adjusted cup anatomic anteversion from 10° to 30° according to the femoral anteversion or posterior pelvic tilt in the standing position. In the non-navigation group, we used a mechanical guide for reaming and cup placement. The mechanical guide showed an operative inclination angle of 40° and an operative anteversion angle of 20°, which corresponds to a radiographic inclination of 41.8° and a radiographic anteversion of 15.2°.
All operations were performed using a direct lateral approach in the lateral decubitus position. For the navigation surgery, landmark and surface matching techniques were used for registration of the pelvis, and accuracy within 1 mm was considered acceptable. Subsequently, acetabular reaming and cup placement were performed under navigation guidance. The final cup inclination and anteversion angles were recorded as intraoperative cup alignment after implantation of the cup.
A CT scan was performed about 3 weeks after surgery for postoperative evaluation. Using these data, we measured the postoperative cup alignment angles and position. The postoperative cup angles were measured using the same protocol as that used for preoperative planning with the 3-D template system. All the reference points on the preoperative plan were copied manually, and the FPP was adjusted in the same way as for the preoperative planning. Three-dimensional models of the acetabular cup were superimposed on the images of the actual implanted cup, and the cup angles and position were measured automatically (Figure 1). For assessment of the position of the acetabular cup, the cup position was defined by coordinates on the X, Y, and Z axes using the 3-D template system (Figure 2). The X-axis (transverse) connected the bilateral anterior superior iliac spines and the Z-axis (longitudinal) was perpendicular to the X-axis parallel of the FPP. The Y-axis (sagittal) was perpendicular to the Z-axis on the sagittal view. The position of the cup center was indicated using these X, Y, and Z parameters. To evaluate the accuracy of cup alignment using the navigation system, we measured the absolute difference between the intraoperative records and the postoperative measurements. In the non-navigation group, a postoperative analysis of cup alignment measures was also performed using postoperative CT images and the 3-D template system in the same way as in the navigation group.
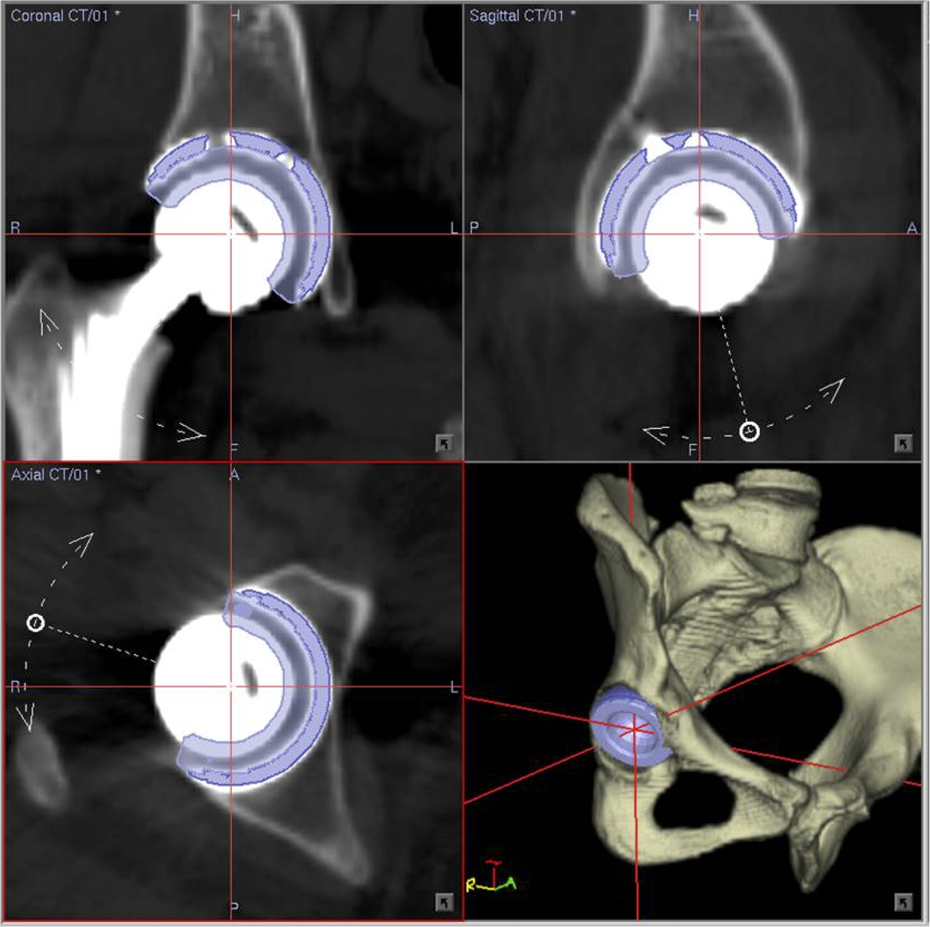
Acetabular component angles and positions were measured by superimposing the templates of the acetabular cup on the image of the actual implanted component.

Cup position (cup center) is indicated in three-dimensional space using the X (transverse), Y (sagittal), and Z (longitudinal) axes.
All statistical analyses were performed using SPSS version 22.0 software (IBM Corp., Armonk, New York). Patient age and body mass index were compared between the navigation and non-navigation groups using the Mann–Whitney U test. The χ 2 was used to compare the inlier rate between the two groups. We tested all continuous parameters for normal distribution using the Kolmogorov–Smirnov test. The Kruskal–Wallis test was used to compare data without a normal distribution. Analysis of variance (ANOVA) was used to compare normally distributed data. The reliability of the cup alignment and the cup position values was assessed by determining the interobserver and intraobserver reproducibility in 30 randomly selected cases. All evaluations for these 30 cases were repeated two times each by two different observers, each of whom was blinded to the results reported by the other, and the intraclass and interclass correlation coefficients were calculated. A p value <0.05 was considered statistically significant.
Results
The patient demographics in the navigation and non-navigation groups are shown in Table 1. There was no statistically significant difference in age (p = 0.087) or body mass index (p = 0.108) between the two groups. The radiographic inclination and anteversion values in the two groups are shown in Table 2, and scatterplots of the angles are shown for each group in Figures 3 and 4. The average radiographic inclination and anteversion angles for all cases in the non-navigation group were 37.5° (range 15.0–55.7°) and 18.2° (range −4.2° to 37.7°), respectively, whereas those in the navigation group were 36.9° (range 27.2–44.8°) and 12.0° (range 3.4–17.4°). The numbers of cases within the combined target angle in total, Crowe I, and Crowe II were significantly higher in the navigation group than in the non-navigation group (p < 0.001, p < 0.001, and p = 0.01, respectively). Although there was no statistically significant difference between in the number of cases classified as Crowe III or IV, the inlier rate in the navigation group (92.9%) was markedly high than that in the non-navigation group (60%). With regard to the accuracy of cup placement when using the navigation system, the absolute values of the differences between the intraoperative navigation records and the postoperative measurements are shown in Table 3. The mean discrepancies in cup inclination and anteversion were within 2.0° and around 2.0°, respectively, for all Crowe classifications. The results for 3-D acetabular component positioning in THA using the navigation system are summarized in Table 4. The mean discrepancy between preoperative planning and postoperative measurement was 1.9 (range 0–7) mm on the X-axis, 2.8 (range 0–13) mm on the Y-axis, and 1.7 (range 0–6) mm on the Z-axis in all patients. The average discrepancies in all three axes for all Crowe classifications were within 3.0 mm and were not significantly different; the p value was 0.328 for the X-axis (Kruskal–Wallis test), 0.757 for the Y-axis (ANOVA), and 0.304 for the Z-axis (ANOVA). No complications related to the navigation procedures were encountered.
Patient demographics.

aValues are expressed as the mean with the range in parentheses.
Cup orientation according to preoperative Crowe classification.
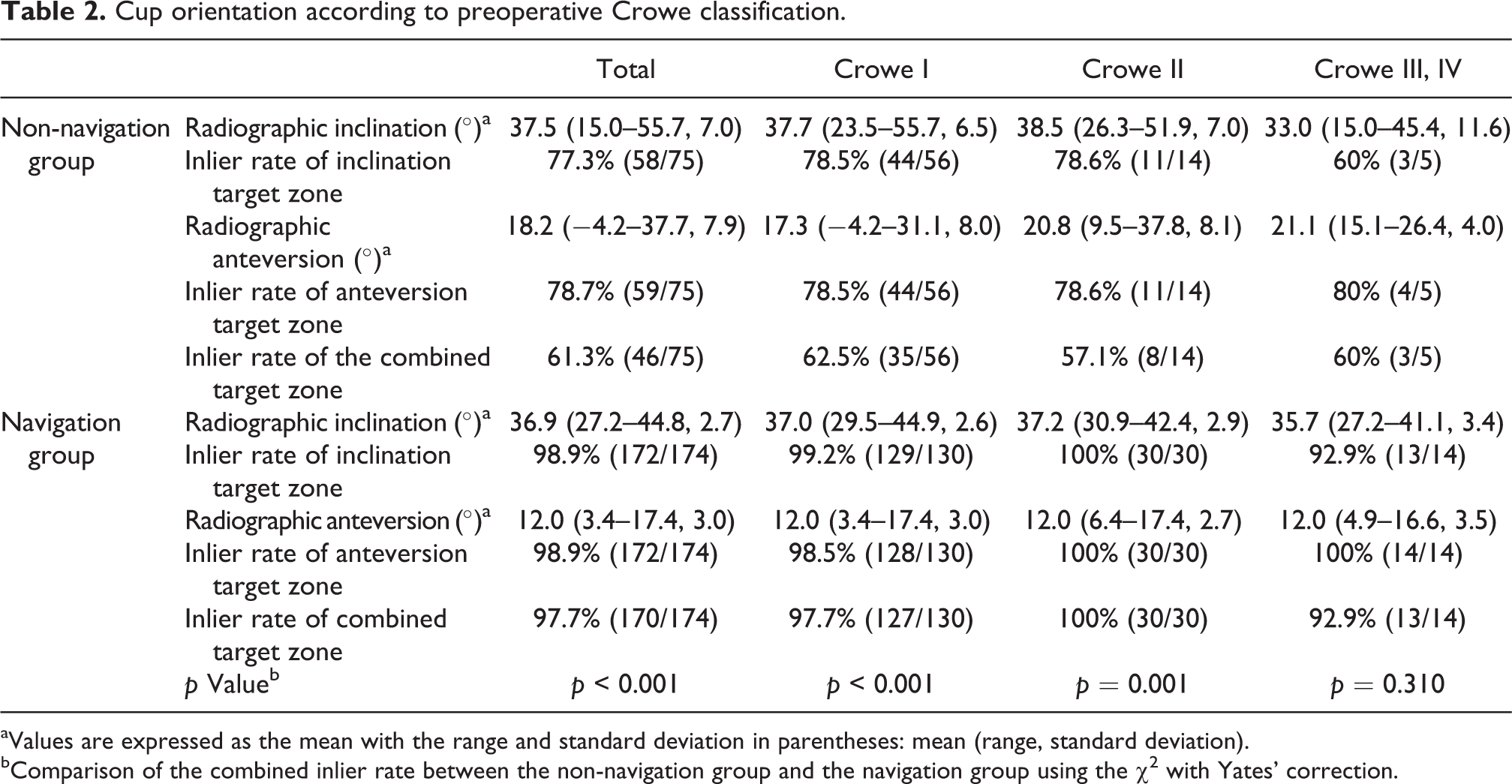
aValues are expressed as the mean with the range and standard deviation in parentheses: mean (range, standard deviation).
bComparison of the combined inlier rate between the non-navigation group and the navigation group using the χ 2 with Yates’ correction.
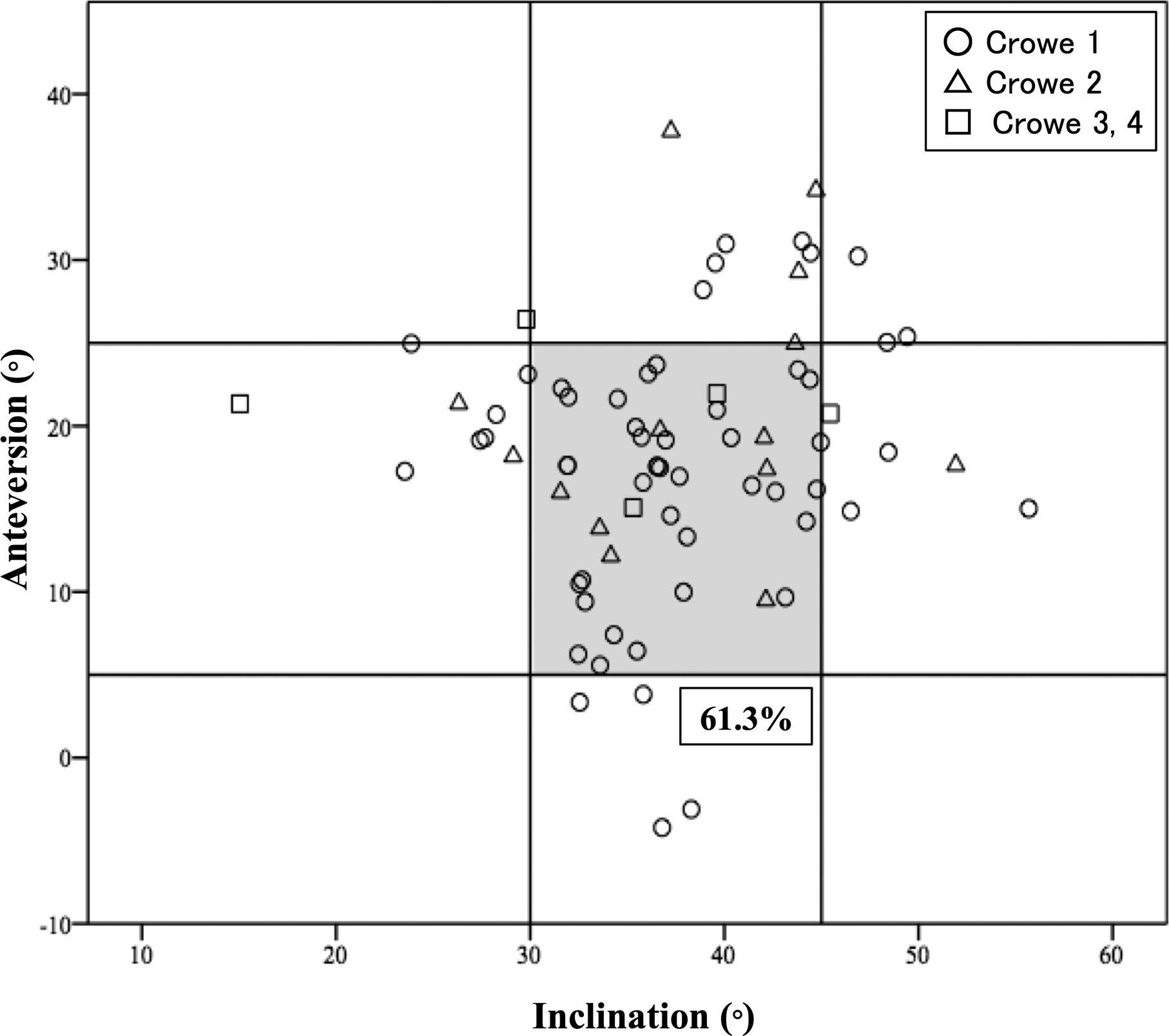
Scatterplot of cup alignment in the non-navigation group. The transverse axis shows the cup inclination angle and the vertical axis shows the cup anteversion angle. All cup alignment angles are indicated by radiographic definition. The gray panel area represents the target zone (30–45° of inclination and 5–25° of anteversion). The inlier rate for combined target angles is 61.3%.

Scatterplot of radiographic cup inclination and anteversion angles in the navigation group showing that 97.7% are within the combined target zone.
Discrepancies in cup angles between intraoperative records and postoperative measurements in the navigation group.a

aAll values are expressed as the mean with the range and standard deviation in parentheses: mean (range, standard deviation).
Cup position values in the navigation group.a

aAll values are expressed as the mean with the range and standard deviation in parentheses: mean (range, standard deviation).
The intraclass and interclass correlation coefficients for all CT measurements, including cup alignments and cup positions on the three axes, were in almost perfect agreement (0.84–0.98, Table 5).
Reliability of implant alignment.

ICC: intraclass correlation.
Discussion
Optimal cup implantation is critical for a satisfactory outcome in THA. However, there are several factors that lead to incorrect cup placement. DDH is considered a complicated condition, especially when severe subluxation is present, as in Crowe types III and IV, because of bony anatomical abnormalities. In the present study, detailed evaluation of CT images demonstrated the benefit of using a navigation system in THA for patients with DDH, regardless of its severity, with regard to not only cup alignment but also spatial cup positioning.
Our study revealed that cup placement in THA had quite high accuracy in patients with DDH when a navigation system was used. In the navigation group, the inlier rate for the target angle was 98.9% for inclination, 98.9% for anteversion, and 97.7% for the combined angles. These rates were significantly higher than those in the non-navigation group. Moreover, in the navigation group, the discrepancy in cup angles between the intraoperative navigation record and the postoperative measurement was 1.2–1.6° for inclination and 1.7–2.2° for anteversion, independent of Crowe classifications; this discrepancy was not statistically significant. Several previous studies have investigated the accuracy of cup alignment in THA using a CT-based navigation system. In one study, Kalteis et al. prospectively evaluated 30 cases of THA for primary OA using a CT-navigation system and reported that 25 of the 30 cups (83%) were positioned within the safe zone, and the absolute error of the cup angles between the intraoperative records and the postoperative measurements was 3.0° (standard deviation 2.6°; range 0–9°) for inclination and 3.3° (standard deviation 2.3°; range 0–9°) for anteversion. 18 In a prospective randomized study reported by Gurgel et al., the mean deviation from the desired cup angles was 3.0° in inclination and 5.5° in anteversion, and 90% of the cases were inside the safe zone. 19 In both these studies, the main indication for THA was primary OA. Iwana et al. reported higher accuracy when using CT-based navigation THA; the difference in cup angles between the postoperative measurements and the intraoperative records was 1.8 ± 1.6° in inclination and 1.2 ± 1.1° in anteversion. 20 Most (96.3%) of the cases in the study reported by Iwana et al. had OA secondary to DDH. The results of that study are similar to those of the present study, indicating that CT-based navigation could achieve quite high accuracy in cup alignment, even in patients with DDH.
In most of the previous reports on THA, “cup position” has meant “cup alignment,” that is, inclination and anteversion of the cup. However, few studies have used 3-D parameters to assess the actual “position” of the acetabular cup, which indicates the positional relationship between the cup and the acetabulum. The reproducibility of the positioning of the acetabular cup is a very important factor when adjusting for leg length discrepancy and global offset, including cup and femoral lateralization, especially in patients with DDH, who have complicated anatomical deformities and subluxation. Moreover, preserving the anterior and posterior walls of the acetabulum is crucial for stable fixation of the cementless cup and is beneficial for reconstruction of the acetabulum in revision surgery. 21 The present study shows that CT-based navigation achieved high precision in spatial cup positioning; the mean discrepancy between preoperative planning and postoperative measurements in all patients was 1.9 ± 1.6 mm for the transverse axis, 1.7 ± 1.3 mm for the sagittal axis, and 2.8 ± 2.3 mm for the longitudinal axis, with no statistically significant differences according to the Crowe classification. Although the number of hips included in our study was small, the mean discrepancy was within 3.0 mm, even in cases with greater subluxation (Crowe types III and IV). Only one previous report has assessed spatial cup positioning in THA using CT-based navigation and reported mean absolute errors in cup positioning of 1.9 ± 1.5 mm, 1.4 ± 1.2 mm, and 1.9 ± 1.3 mm on the transverse, sagittal, and longitudinal axes, respectively. 20 In that report, most of the patients had OA secondary to DDH, but the detailed classification of DDH was not mentioned. Compared with that study, our results indicate slightly inaccurate positioning on the longitudinal axis. Cup positioning on the transverse and sagittal axes is strongly influenced by anatomical factors, but that on the longitudinal axis can be affected by the surgical situation and intraoperative decisions made by the surgeon regarding cup height. Although some surgeons prefer to implant the cup first and perform the final adjustment when implanting the stem, we normally adjust the cup position according to the depth of the stem or the soft tissue tension, especially in patients with DDH, who have subluxation and anatomical alterations in both the acetabulum and the femur. Thus, intraoperative adjustment of the cup height might lead to error with respect to the preoperative planning.
The use of CT-based navigation raises concerns about radiation exposure. Using an imageless navigation system would avoid radiation exposure, but its accuracy may be less than that of CT-based navigation because the outcome of imageless navigation is strongly affected by the landmark pointing technique used and the soft tissue thickness. 22 Moreover, using the APP as the reference plane cannot accommodate changing of pelvic tilt in every case. 23 CT measurement has been the gold standard for precise 3-D evaluation of the cup with adjustment of the pelvic reference. 24 We consider that CT-based navigation is the most accurate and useful supporting tool for THA to date. Preoperative and postoperative CT evaluation is essential for obtaining precise anatomical and implant information, which is particularly advantageous in patients with DDH, in whom the anatomy of the acetabulum is distorted.
There are several limitations to our study. First is its retrospective design. From January 2006 onward, we routinely performed CT examination before and after surgery; however, no cases in the navigation group and only 5 of 80 cases in the non-navigation group were excluded because of a lack of CT data. Therefore, we believe that case selection bias in this study would have been minimal. Second, the sample size was small, particularly in the non-navigation group. We have been using a CT-based navigation system since 2008, so all patients in the non-navigation group underwent surgery before 2008. In addition, both pre- and postoperative CT data were essential to perform a detailed assessment in this study. Therefore, patients could only be entered into the non-navigation group if they had undergone surgery between 2006 and 2008. Third, the target angle of the cup was different between the navigation group and the non-navigation group (38.3° of radiographic inclination and 12.7° of radiographic anteversion in the navigation group and 41.8° and 15.2°, respectively, in the non-navigation group). In this study, we used the concept of a safe zone to evaluate the cup alignment and both target angles were roughly center of the safe zone; thus, we believe the influence of these slight differences in target angles was small.
Conclusion
This study demonstrated that a CT-based navigation system achieved quite high accuracy of cup alignment angles and spatial cup positioning in primary THA for patients with DDH, with no significant differences according to the Crowe classification.
Footnotes
Acknowledgment
The authors thank Dr Hiroshi Egawa for his contribution to this study as one of the supervisors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.