
Abstract
Background:
Various radiographic measurements that describe humeral head coverage by the acromion and the effect on rotator cuff pathology have been reported. This study aimed to describe and validate a new radiographic measurement, the acromiohumeral centre edge angle (ACEA).
Methods:
We compared the ACEA on computed tomography (CT) and plain X-ray to determine whether X-ray is accurate for measuring this angle. We then compared the results from this control population with 107 patients with acute rotator cuff tears. We compared functional outcomes in rotator cuff tear patients to determine whether the ACEA has any effect on outcome after surgery. An intra- and inter-observer variability analysis was performed and we compared the ACEA to the acromial index (AI) on rotation X-rays.
Results:
The ACEA was comparable on CT and plain X-ray and was most accurate when true anteroposterior glenohumeral X-rays were used (15.94° vs. 15.87° on CT, p = 0.476). The ACEA showed high intra- and inter-observer reproducibility and was unchanged on internal and external rotation X-rays (20.48 vs. 20.47, p = 0.842), whereas the AI was significantly different (0.74 vs. 0.70, p < 0.001). The ACEA was significantly higher in our rotator cuff tear patients than the control population (23.9° vs. 16.6°, p < 0.001), although a higher ACEA was not associated with poorer outcomes.
Conclusion:
The ACEA is a valid measurement for describing humeral head coverage by the acromion and can be accurately measured on plain radiographs with good reproducibility. It is unaffected by shoulder rotation and was significantly higher in patients with acute rotator cuff tears.
Introduction
Bigliani et al. first described different acromion shapes and how this affected rotator cuff pathology. 1 He analysed the shape of the acromion on lateral radiographs and found a higher prevalence of rotator cuff tears in patients with a hooked (type III) acromion than in those with a curved (type II) or flat (type I) acromion. Since then, there have been numerous radiographic measurements described which analyse the acromion and its relationship with the humeral head and glenoid which have various prognostic indicators. Banas et al. described the lateral acromial angle (LAA) as the angle between the glenoid and the undersurface of the acromion. 2 A smaller LAA (i.e. a downsloping acromion) has been reported as being associated with higher rates of rotator cuff tear. 3 Nyffeler et al. introduced the acromial index (AI) which describes the lateral extension of the acromion. 4 Measured on true anteroposterior radiographs, it is a ratio of glenoacromial (GA) to glenohumeral (GH) distance where a higher AI (i.e. a more laterally extending acromion resulting in greater humeral head coverage) is associated with a higher incidence of rotator cuff tears and recurrent tears post-repair. 4 –7 The acromial angle is measured on arch radiographs and is the angle between the anterior and posterior undersurface of the acromion with increased angles associated with higher rates of impingement and rotator cuff tears. 8 The acromial coverage index (acromial distance/humeral distance) is a ratio of the acromial distance to the humeral distance with higher ratios, indicating more coverage of the humeral head, associated with higher rates of rotator cuff tear. 6
This study proposes a new measurement, the acromiohumeral centre edge angle (ACEA), which is the angle created between a line drawn superiorly from the centre of the humeral head parallel to the glenoid and a second line from the centre of the humeral head to the outer edge of the acromion on a true anteroposterior GH X-ray.
We believe that measurement of the ACEA is easier than the AI which requires two measurements and a calculation in order to find the ratio. We also believe that it is less prone to error than the LAA as identification of the undersurface of the acromion can be difficult in patients with different shaped acromions. The aims of this study were to determine whether plain radiographs could be used to accurately measure the ACEA and whether it is reproducible. We aimed to compare the ACEA with other measurements described in the literature, specifically the AI in order to determine whether rotation had any effect on either measurement and thus whether one was more accurate and reliable than the other. We believe that because the AI uses the greater tuberosity in its measurement (GH distance) rotation could have an effect (given the change in position of the tuberosity with humeral rotation) even when a true AP GH X-ray is taken. We aimed to determine whether the ACEA differs in patients with acute rotator cuff tears than the general population and whether it has any effect on outcome following rotator cuff repair. Secondary aims included determining whether the AI and LAA differed between the normal population and patients with rotator cuff tears and whether these measurements had any effect on patient outcome following rotator cuff repair.
Materials and methods
In order to perform this study, we first analysed 100 trauma computed tomography (CT) scans (200 shoulders) in patients under the age of 50 years from our institute. All trauma CT scans were done for blunt trauma (almost exclusively following motor vehicle accidents). These 200 shoulders served as our control population. We obtained this list of patients from our hospital’s trauma database. Trauma CT’s are performed with patients lying supine on the CT table and typically with their arms by their side in neutral rotation. Those patients who had their CT scans performed with their arms above their heads or across their abdomens were excluded from the analysis. We reviewed patient clinical records and excluded those who had any previous shoulder pathology recorded. Any patient who had sustained a shoulder injury as result of the trauma was also excluded. Furthermore, only those patients under the age of 50 years were included in this control group as they are more likely to be asymptomatic than an older population with regards to their shoulders. We measured the ACEA for all 200 shoulders on coronal plane slices. We formatted all CT images on an axial slice through the scapula using multiplanar reconstruction (MPR), so that the resultant coronal plane slices were perfectly perpendicular to the plane of the glenoid (i.e. a perfect anteroposterior coronal image of the GH joint). To measure the ACEA (see Figure 1), we superimposed a circle over the humeral head in order to find its centre. This circle followed the contour of the articular surface of the humeral head (ignoring the tuberosities). One limb of the angle was drawn superiorly from the centre of the humeral head parallel to the glenoid. The second limb was drawn from the centre of the humeral head to the outer (most lateral) edge of the acromion. The angle created between these two lines was measured as the ACEA.

ACEA: Measuring the ACEA on an AP GH X-ray. A circle is first superimposed over the humeral head which follows its articular surface. The angle is formed with the first limb drawn superiorly from the centre of the circle parallel to the glenoid and the second drawn from the centre of the circle to the lateral most aspect of the acromion. ACEA: acromiohumeral centre edge angle; GH: glenohumeral.
We then remeasured the ACEA for all 200 shoulders on their corresponding plain shoulder radiographs (when available) or the CT scout image. If the patient had a shoulder X-ray, the angle was measured on the AP GH image. If they hadn’t had dedicated shoulder views, then the CT scout image provided an alternative for measuring this angle. Given that both images are two-dimensional (as opposed to the three-dimensional CT scan) and they cannot be manipulated like a CT scan to obtain a perfect AP GH view, they would be considered less accurate for measuring the ACEA. If the X-ray had not been taken perpendicular to the plane of the glenoid (i.e. a true anteroposterior X-ray of the GH joint) and there was a double line, representing the anterior and posterior rims of the glenoid, a line was drawn between the supraglenoid and infraglenoid tubercles to represent the plane of the glenoid (and thus one limb of the ACEA). Only those patients in whom we could measure the ACEA on both CT scan and plane radiographs were included in the analysis, as the purpose of measuring the angle on both was to determine whether plain X-rays could be used to accurately measure the angle and therefore be used as a substitute for CT which would be considered the gold standard.
We also measured the AI and LAA (see Figures 2 and 3) for all 200 shoulders on CT scans and on corresponding plain X-rays and compared the two imaging modalities to ensure that X-ray could also reproduce these measurements accurately.

AI: The AI, measured on a true AP GH X-ray, is a ratio of the GA to GH distance measured perpendicular to a line parallel to the glenoid. AI: acromial index; GH: glenohumeral; GA: glenoacromial.

LAA: The LAA is the angle between the glenoid and the undersurface of the acromion. LAA: lateral acromial angle.
We randomly chose 25 patients from the rotator cuff group (see later in this section) who had true AP GH X-rays and the primary author (NS) remeasured the ACEA on a second occasion in order to perform an intra-observer variability analysis. The second author (LA) also measured the ACEA on these same 25 radiographs in order for an inter-observer variability analysis to be performed. The same was performed for the AI and LAA.
Another 25 patients were randomly selected from the rotator cuff group (see later in this section) who had undergone AP GH X-rays with the humerus in internal and external rotation, and the ACEA and AI were measured on both views in order to determine whether rotation has any effect on either measurement.
After confirming that plain X-ray could be used for accurately measuring the ACEA, we then compared this angle between a normal population (our 200 shoulders from the initial assessment served as this group) and a population of patients with acute rotator cuff tears. We obtained a list of all patients who had undergone rotator cuff repair surgery in our hospital during the past 4 years. All surgeries had been performed with ACC funding. ACC is a government organization which provides treatment funding for anyone sustaining an injury in New Zealand. These cuff tears were therefore all acute or traumatic in nature given they had been ACC approved for surgery as opposed to chronic or degenerative cuff tears which are not funded by ACC. When there is uncertainty about a traumatic versus degenerative condition, ACC will often require further imaging, such as a magnetic resonance imaging (MRI), before agreeing to fund treatment, and so a small number of these cuff tears had undergone MRI scans to exclude degenerative tears. The reason we chose to look at just acute cuff tears was twofold. Firstly, one of the aims of the study was to determine whether the ACEA could be used to predict acute cuff tears due to an anatomic variation (i.e. an overhanging acromion) rather than chronic or degenerative cuff tears which are multifactorial and develop over time. Secondly, chronic cuff tears can result in superior migration of the humeral head which could therefore potentially effect measurement of the ACEA and thus our results.
All of these patients had standing plain X-rays of the affected shoulder as part of their workup before surgery. None had superior migration of the humeral head. We reviewed their plane radiographs and measured the ACEA on the AP GH X-ray. This enabled for us to then determine whether there was any difference in ACEA between the two groups. We also measured the AI and LAA and performed the same comparison.
We sent those patients who had undergone rotator cuff repair surgery the Flex-SF function questionnaire and a visual analogue satisfaction (VAS) score at a minimum of 12 months post-surgery in order to determine whether the ACEA (or AI or LAA) had any effect on outcome following surgery.
Approval to conduct this study was granted by our hospital’s research committee.
Statistical analyses
The paired CT and plane X-ray observations from the 200 control patients were compared using Bland–Altman plots and 95% limits of agreement were calculated. Independent comparisons between control patients and rotator cuff patients and between gender groups were undertaken using independent t-tests. Pearson’s correlation coefficients were used to assess the strength of the associations between the three measurements (ACEA, AI and LAA) and between these measurements and age and functional outcomes. The magnitudes of the intra- and inter-observer assessments are summarized as the coefficients of variation ascribed to the relevant source of variation and as intra-class correlations, representing the variation between patients’ measures as a percentage of all variation. A two-tailed p value < 0.05 was taken to indicate statistical significance.
Results
When comparing the ACEA as measured on CT scan with the measurement from plain X-ray (within the control population of 200 shoulders, average age 35 years), we found no clinical difference in the results (see Table 1). Twenty shoulders (out of the 200) in the control group had undergone dedicated shoulder X-rays including a true AP GH X-ray. When we looked specifically at these 20 shoulders and compared the ACEA measured on CT scan (15.87°) with true AP GH X-rays (15.94°), we found the mean difference was significantly less (only 0.069°).
Comparison of CT and plane X-ray measurements.

CT: computed tomography; ACEA: acromiohumeral centre edge angle; AI: acromial index; LAA: lateral acromial angle; SD: standard deviation.
We also found that X-ray could be used to accurately measure the AI and LAA with no significant clinical difference in measurements when compared with CT scan (see Appendix 1 for Bland–Altman plots). Similar to the ACEA, when we compared these measurements on CT and X-ray in the 20 patients who had true AP GH X-rays, we found the differences were significantly less (Table 2).
Comparison of the centre edge angle, AI and LAA as measured on CT scan and true AP GH X-ray.

AI: acromial index; LAA: lateral acromial angle; CT: computed tomography; GH: glenohumeral; ACEA: acromiohumeral centre edge angle.
The results of the intra-observer and inter-observer variability analysis found the ACEA to have high intra- and inter-observer concordance as did the AI and LAA (Table 3 and Table 4).
Summary of intra-observer variation.a

ACEA: acromiohumeral centre edge angle; AI: acromial index; LAA: lateral acromial angle; CV%: coefficient of variation; ICC: intra-class correlation coefficient.
aThe CV% represents the random differences between replicates as a % of the mean: <5% is taken to show very good reliability. The ICCs represent the variability between patients as a % of the total variation among readings. Values close to 100% indicate that variability between duplicates is not a source of any significant variation.
Summary of inter-observer variation.

CV%: coefficient of variation; ICC: intra-class correlation coefficient; ACEA: acromiohumeral centre edge angle; AI: acromial index; LAA: lateral acromial angle.
When we measured the ACEA on internal and external rotation X-rays, we found that rotation had no effect on this angle (20.48 vs. 20.47, p = 0.842). However, when we measured the AI on internal and external rotation X-rays, we found that it changed significantly (0.74 vs. 0.70, p < 0.001). This was due to the change in GH distance (52.63 vs. 55.41, p < 0.001). The GA distance was unchanged on internal and external rotation (38.70 vs. 38.73, p = 0.791). The LAA also remained unchanged on internal and external rotation X-rays (see Table 5).
Comparison of ACEA, AI and LAA on internal and external rotation X-rays.
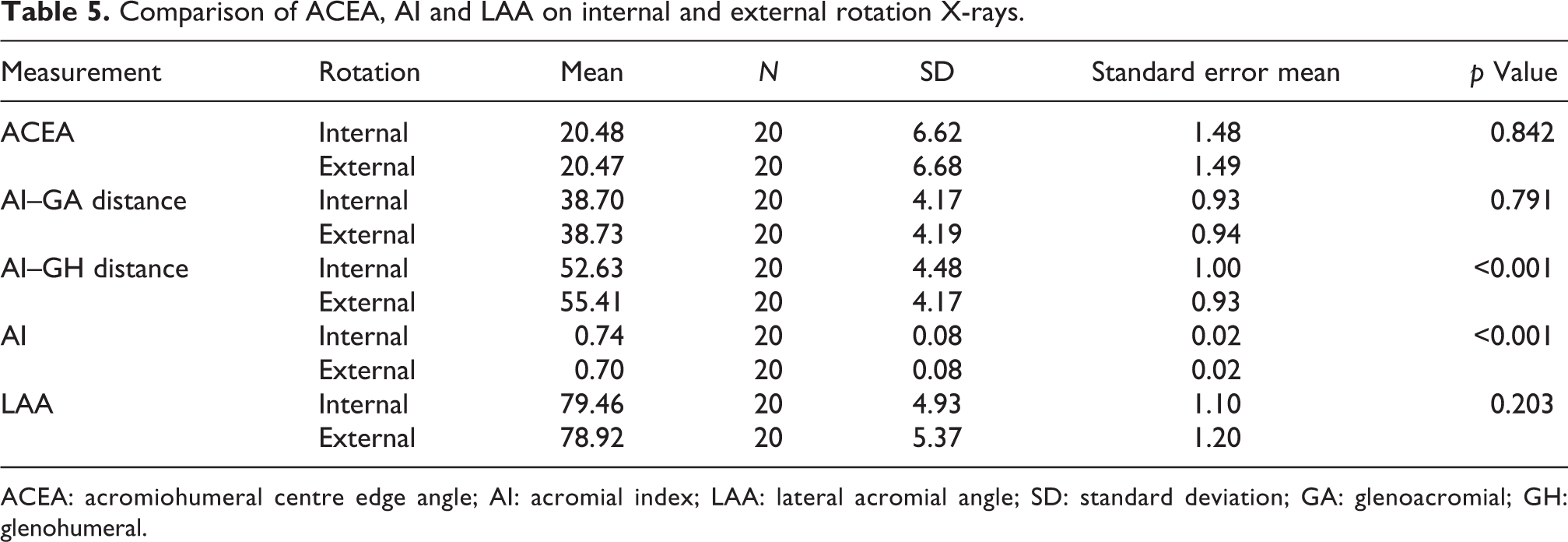
ACEA: acromiohumeral centre edge angle; AI: acromial index; LAA: lateral acromial angle; SD: standard deviation; GA: glenoacromial; GH: glenohumeral.
When comparing the ACEA between the control population and the population of patients with acute rotator cuff tears (107 patients, average age 63 years, see below), we found that patients with rotator cuff tears had significantly higher average ACEAs (23.89° vs. 16.66°, p < 0.01). The results also found that patients within the rotator cuff tear group had significantly higher AIs (0.755 vs. 0.690, p < 0.01) and significantly lower LAAs (76.48° vs 79.71°, p < 0.01) as has previously been reported. Table 6 summarizes these data. Of note, no patient in the rotator cuff tear group had evidence of superior migration of the humeral head with a preserved acromiohumeral distance of at least 8 mm.
Comparison of radiographic measurements between control group and rotator cuff group.

ACEA: acromiohumeral centre edge angle; AI: acromial index; LAA: lateral acromial angle. Those results that reached statistical significance are in bold to highlight these
Hundred fifty patients had undergone rotator cuff repair surgery at our institution in the preceding 4 years. We sent those who were at least 12 months post-surgery the Flex-SF function questionnaire and a visual analogue satisfaction questionnaire. We received responses from 107 patients (mean 29 months post-surgery, range 14–46 months) and found that within these patients, higher ACEAs were not associated with worse outcomes (Flex-SF function scores or satisfaction scores). Similarly, neither were higher AIs nor lower LAAs. Table 7 summarizes these results. Interestingly though, females had significantly higher average ACEAs, higher AIs and lower LAAs than males and there was a trend for worse Flex-SF function scores and lower satisfaction scores in females following surgery, although this did not reach statistical significance (see Table 8). All three X-ray measurements (ACEA, AI and LAA) highly correlated with one another (all p < 0.001).
Summary of the results within the rotator cuff group.
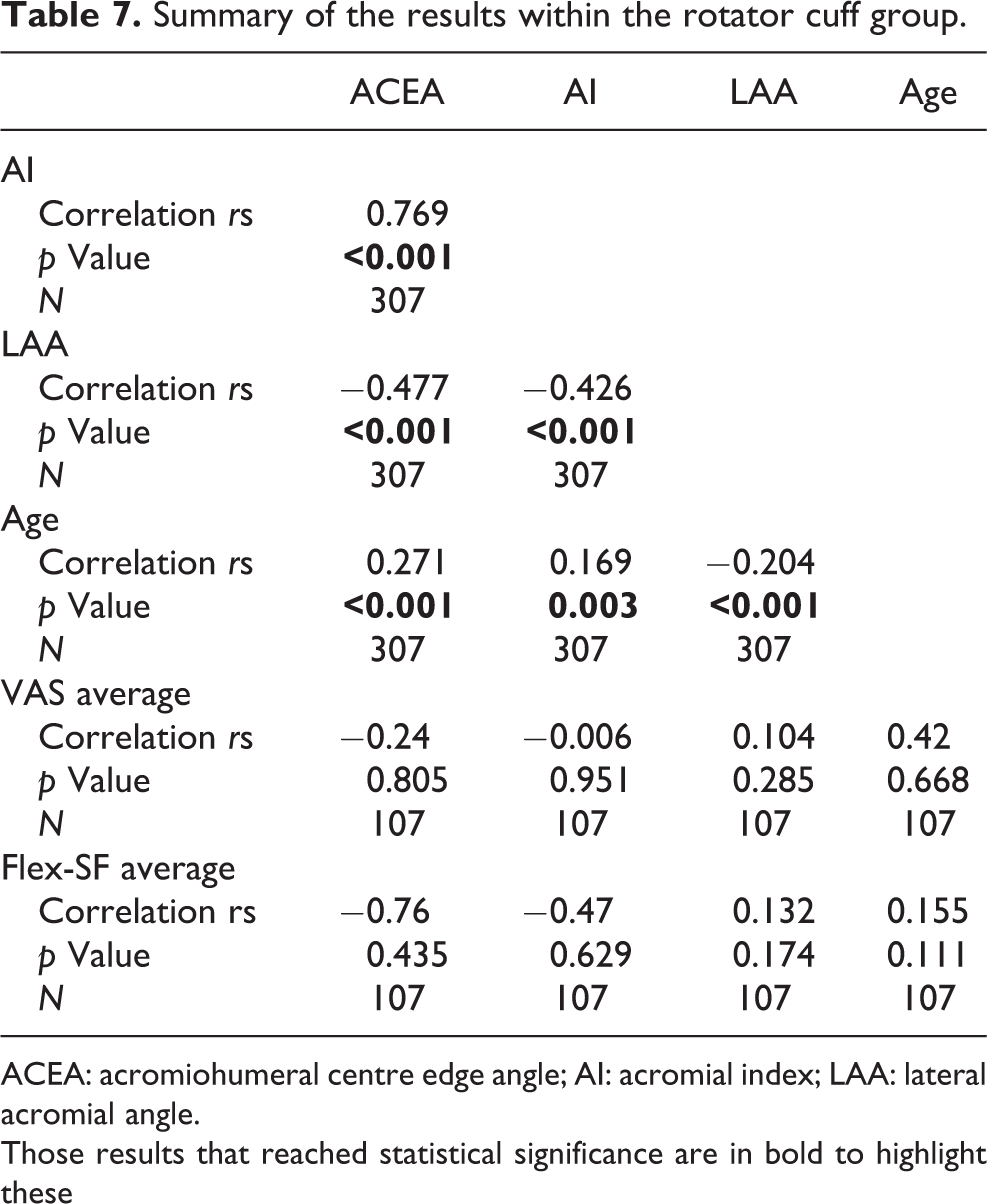
ACEA: acromiohumeral centre edge angle; AI: acromial index; LAA: lateral acromial angle. Those results that reached statistical significance are in bold to highlight these
Comparison of radiographic measurements and outcomes between males and females.

ACEA: acromiohumeral centre edge angle; AI: acromial index; LAA: lateral acromial angle. Those results that reached statistical significance are in bold to highlight these
Discussion
A good classification system must be both reliable and valid. 9,10 We designed the ACEA as we felt that it would fulfil both of these requirements. The ACEA describes the relationship between the acromion and humeral head. It is analogous to the centre edge angle of the hip where smaller angles can be associated with hip dysplasia. Conversely, in the case of the shoulder, higher ACEAs (i.e. increased amounts of humeral head coverage) are associated with higher rates of rotator cuff tears, as this study has shown. We believed that the ACEA would be easy to measure and thus highly reproducible. Our findings have confirmed this with the ACEA having high intra- and inter-observer concordance when measured on AP GH X-rays, higher even than the AI and LAA. CT scan would be considered the gold standard for measuring the ACEA because CT scans can be formatted and the orientation of slices adjusted using MPR. We were therefore able to measure the ACEA on a perfect AP coronal image of the GH joint on CT. We were also able to scroll through coronal slices to determine the exact lateral most aspect of the acromion. We thus felt that CT would give an exact measurement of this angle. We had hoped to find no difference between the two imaging modalities but deemed a difference of 0.82° clinically acceptable and within an acceptable error of measurement. The majority of the X-ray measurements in the control group was made on the two-dimensional CT scout image (“scanogram”) which does not necessarily give a true AP of the GH joint and could therefore account for this difference. When we compared the ACEA in patients who had undergone CT scan and a true AP GH X-rays, this difference was significantly less (0.069°). We found that this was also the case for the AI and LAA (and, in fact, most authors describe measuring the AI and LAA on AP GH X-rays). We therefore recommend that the ACEA is measured on true AP GH X-rays in order to obtain the most accurate measurement. We found that the ACEA, unlike the AI, is unaffected by shoulder rotation which is one of the key findings of this study as rotation on X-rays is not always consistent, and therefore a measurement that is unaffected by rotation is likely to be the most reliable and accurate.
There are multiple other measurements which also describe this relationship between the humeral head and acromion of which the AI and LAA are most widely reported. The AI requires two measurements and a calculation in order to obtain a result, perhaps making it more prone to error. We postulated that the AI (GA to GH ratio) could be affected by shoulder rotation given the change in position of the greater tuberosity (and thus the GH distance) with differing positions of humeral rotation even when a true AP X-ray of the GH joint is taken. Our findings have confirmed this and shown that although the AI had high intra- and inter-observer concordance when measured on true AP GH X-rays with the humeral head in neutral rotation, it was significantly different in the same patient when AP GH X-rays were taken in internal and external rotation. It is also known that rotator cuff pathology can cause erosion of the greater tuberosity which would therefore affect the GH distance and thus the AI. Despite this, the average AI in our rotator cuff tear group (0.755) was comparable with that reported in other studies (0.75 by Balke, 0.73 by Nyffeler, 0.72 by Torrens, 0.67 by Kim, 0.71 by Melean and 0.687 by Ames). 3,4,6,11 –13 Similarly, the average LAA in our rotator cuff tear group (76.48°) was similar to that reported by Balke (77°). 3
The average ACEA in our rotator cuff tear group of patients was significantly higher than our control group indicating a greater amount of humeral head coverage. A greater amount of humeral head coverage could plausibly result in higher rates of rotator cuff impingement and tears due to a compression effect as has been previously described in the literature.
The results showed that within the rotator cuff group differing ACEAs, AIs and LAAs had no effect on outcome (Flex-SF function scores or VAS scores). This contrasts other studies in the literature. For example, a study by Ames et al. showed lower satisfaction outcomes in patients with higher AIs post-rotator cuff repair. 11 Similarly, Zumstein et al. have shown higher AIs are associated with higher rates of retear after surgery. 7 A possible explanation for these contrasting findings is that within our hospital, an acromioplasty is always performed concurrently during rotator cuff repair. The morphology of the acromion is a factor that can be surgically modified through an acromioplasty, whereby the undersurface is excised to create more space and thus reduce impingement and potentially the incidence of recurrent tear. This study’s results could potentially be different if performing an acromioplasty at the time of surgery was not the normal practice.
We did not look specifically at rotator cuff tear size (although on review tears involved supraspinatus and all patients underwent a standard arthroscopic acromioplasty and mini-open repair) which is a limitation of the study. The ACEA is used to predict the incidence of acute rotator cuff tear (presumably due to anatomic variation and having a large overhanging acromion) as opposed to chronic or degenerative tears which are more multifactorial in nature. Thus, no patient in our rotator cuff tear group had evidence of superior migration of the humeral head on standing AP GH radiographs (which likely takes time to develop and is therefore more indicative of a chronic tear). This should be taken into consideration when interpreting the results. We can conclude that patients with a higher ACEA have a higher incidence of acute rotator cuff tear but cannot comment on the development of more chronic tears.
Our results showed that females had higher average ACEAs and AIs and lower LAAs than males. It has been reported elsewhere in the literature that females have higher AIs and acromial coverage indices, although we could find nowhere that reported higher rates of rotator cuff tears among females. 6 The trend for a worse functional outcome and lower satisfaction scores among females could be explained by this finding; however, this contradicts the overall finding of the study where higher ACEAs were not associated with a worse outcome.
We chose to use the Flex-SF score as a measure of function. The Flex-SF is a self-reported measure of shoulder function. Patients respond to an initial routing item that classifies them as having low, medium or high shoulder function. They then respond only to the testlet that best targets their level of function. A raw testlet score is obtained and then correlated to a Flex-SF score using a concordance table. The Flex-SF score has been shown to be highly reliable and exhibits excellent validity. 14
All three X-ray measurements (the ACEA, AI and LAA) highly correlated with one another (all p < 0.001). This would be expected given that all three measurements essentially describe the amount of humeral head coverage by the acromion, just using different anatomical landmarks for making these measurements. This provides further evidence for the ACEA angle being a reliable measure for humeral head coverage by the acromion.
Multiple studies have investigated the relationship between humeral head coverage by the acromion and rotator cuff pathology. Nyffeler et al. described an association between the lateral extension of the acromion (the AI) and rotator cuff tears where a larger AI was associated with an increased incidence of rotator cuff tear. 4 They therefore proposed a biomechanical theory in rotator cuff tear etiology where a larger lateral extension of the acromion creates a more vertical ascending force component of the middle deltoid. 4 Consequently, the pressure between the humeral head and the acromion rises which may lead to subacromial impingement and rotator cuff tear. Miyazaki et al. suggested that the AI may be a predictor of rotator cuff tears in some populations (e.g., Brazilians) but not others (e.g., Japanese). 5 Torrens et al. reported that patients in Spain with rotator cuff tears had significantly larger AIs compared with those without cuff pathology. 6 Torrens et al. also found a difference between genders with females having higher acromial coverage. 6 Hanciau et al. found a statistically significant association between the AI and the LAA and subacromial impingement. 15 Balke et al. found that patients with rotator cuff tears had significantly lower LAAs and higher AIs than a control group without shoulder pathology. 3
In contrast, Baechler and Kim found that the percentage of humeral head not covered superiorly and laterally by the acromion may be a factor in the pathogenesis of rotator cuff tears due to hinging of the humeral head on the anterolateral edge of the acromion during early shoulder abduction causing impingement of supraspinatus between these two structures. 16 Similarly, Melean et al. found no positive correlation between a larger AI and the incidence of recurrent rotator cuff tears. 13
Ames et al. investigated the AI in patients who had undergone arthroscopic rotator cuff repair and found no significant difference in the AI when compared to patients with intact cuffs. 11 However, when analysed as a continuous variable, a larger AI was associated with an increased number of tendons torn and anchors used for repair. 11 Furthermore, when the AI was dichotomized (>0.682 and <0.682), a significant difference was seen in QuickDASH and SF-12 PCS scores with a trend towards diminished patient satisfaction in the larger AI group. 11
Conclusion
This study has described a new radiographic measurement pertaining to the shoulder. The ACEA can be accurately measured on plane radiographs and is highly reproducible (with even higher intra- and inter-observer concordance than the AI and LAA). We found that the ACEA is unaffected by shoulder rotation whereas the AI is. The ACEA was higher in patients with acute rotator cuff tears than our control population, although a higher angle was not associated with a poorer outcome following rotator cuff repair surgery possibly due to concurrent acromioplasty. Females tended to have higher angles than males and a trend towards poorer outcomes following surgery. This study also found that patients with rotator cuff tears had higher AIs and lower LAAs than the control population, which has been reported elsewhere in the literature, although this did not impact on outcome following surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.