
Abstract
Purpose:
The aim of this study was to assess applicability of arthroscopic technique in intramedullary nail fixation of humerus shaft fractures and to compare with conventional nailing in terms of its effects on perioperative and postoperative intra-articular complication rates as well as on clinical and functional outcomes.
Methods:
This prospective randomized controlled clinical trial included 40 patients (12 females and 28 males) indicated for surgery between either undergo arthroscopy-assisted (Arthroscopy-assisted intramedullary nailing [AIMN]; n = 20) or conventional (Intramedullary nailing [IMN]; n = 20) anterograde intramedullary nailing. Two groups were compared in terms of mean number of fluoroscopic shootings until the guide wire was inserted, time for union, length of hospital stay, and complication rates. Shoulder functions were assessed by Constant and American Shoulder and Elbow Surgeons (ASES) score.
Results:
Groups did not significantly differ in terms of age, gender, and mechanism of injury, length of hospital stay, union rate, and mean union time (p > 0.05). Mean ASES and Constant scores were found to be statistically significantly higher in AIMN group than that in IMN group (p = 0.000 and p = 0.002, respectively). Mean number of fluoroscopic shootings until the guide wire was inserted was 2.15 in AIMN group, which was significantly lower compared to 4.2 of IMN group (p = 0.000).
Conclusions:
Arthroscopy-assisted technique may be an applicable and safe method owing to its cosmetic advantages and more satisfactory postoperative shoulder functions subsequent to less injury to deltoid, rotator cuff, and other soft tissue, as compared to conventional anterograde approach.
Introduction
Humerus diaphysis fractures constitute 20% of humerus fractures and 3–5% of all fractures. 1 Conservative approaches (e.g. functional bracing) achieved successful outcomes in nondisplaced or minimally displaced fractures owing to their high union potential. 2,3 Intramedullary nail, plate, and external fixators could be used for fixation in patients indicated for surgery. 1
Intramedullary nail fixation is a reliable fixation method in high-impact long bone fractures, advanced osteoporosis, and pathological fractures. 4 Though anterograde or retrograde approaches are present, decision of either approach depends on the anatomic localization, type of the fracture, and experience of the surgeon. 5
Many research reported technical errors and complications regarding intramedullary nail fixation. 4 Subacromial impingement and consequent injury to shoulder joint could be encountered secondary to placement of the nail superior to subchondral region or its superior migration during or after insertion of the nail. In particular, chronic shoulder pain and functional disability are common complications after damage to cartilage of humeral head and rotator cuff. 5,6
Current management of fractures features minimal invasive approaches after widespread use of arthroscopy and advancement of surgical instruments and techniques. Advantages of arthroscopic interventions include less soft tissue injury, less morbidity that may negatively affect functional outcomes like postoperative scarring, achievement of better reduction by visual inspection of fracture reduction at articular site, fixation of screw or nail penetration within the joint, and good cosmetic outcomes. 7
The purpose of this study was to assess applicability of arthroscopic technique in intramedullary nail fixation of humerus shaft fractures and to compare with conventional nailing in terms of its effects on perioperative and postoperative intra-articular complication rates as well as on clinical and functional outcomes.
Methods
This prospective randomized controlled clinical trial was approved by Local Ethics Committee of our hospital. All subjects gave written informed consent. Patients were operated by the same surgeon. A total of 40 patients (12 females and 28 males) indicated for surgery between January 2013 and December 2015 were randomized to either undergo arthroscopy-assisted (Arthroscopy-assisted intramedullary nailing [AIMN]; n = 20) or conventional (Intramedullary nailing [IMN]; n = 20) anterograde intramedullary nailing. Indications for surgery were inability to achieve an acceptable alignment that were <20° anterior angulation, <30° varus/valgus angulation, and <3 cm shortening and distraction at fracture site. Patients diagnosed with clinically and radiologically documented spiral (AO12-A1), short oblique (AO12-A2), or transverse (AO12-A3) humerus diaphyseal fracture and indicated for the surgery were included in the study (Table 1). Exclusion criteria were patients with open proximal humerus epiphyseal lines, pathological fractures, neurovascular injury, infected fractures, history of previous humerus fracture, grade 3 open fractures, and concomitant rotator cuff tear or preexisting shoulder pathology.
Distribution of fracture types.

All patients were administered prophylactic cephazolin 1 g Intravenous (IV), 1 h before the surgery. Patients were prepared in beach-chair position under general anesthesia. Fluoroscopy was positioned appropriately. Following necessary sterilization and draping procedures, affected side was marked, including anatomical landmarks and fracture line. In AIMN group, the shoulder joint was visualized through posterior arthroscopic portal following posterior incision made inferomedial to the lateral border of spine of scapula. In order to determine entrance site of the nail, a 2.2-mm Kirschner wire (K-wire) was introduced percutaneously distal to the anterolateral border of the acromion, targeting humeral shaft and intramedullary cavity over the articular cartilage just medial to the greater tubercle posterior to the biceps tendon (Figure 1). About a 2-cm incision was performed at the level of K-wire after arthroscopic and fluoroscopic confirmation. Deltoid fibers were passed by blunt dissection to reach supraspinatus (Figure 2). The joint was accessed by 10-mm incision parallel to the extension of supraspinatus tendon. A cannulated awl was introduced over the K-wire, through which a guide wire was also inserted ensuring passing through the fracture line. After confirmation of the fracture reduction under fluoroscopy, intramedullary humerus nail with appropriate diameter and length was delivered. After ensuring that proximal part of the nail was within the articular cartilage arthroscopically, two screws were delivered into the head of humerus from proximal side. That screw heads did not penetrate articular cartilage was verified by arthroscopy prior to osteosynthesis by two screws exploring radial nerve through a mini incision performed from distal side. An end cup was placed under arthroscopy and supraspinatus was repaired by a single nonabsorbable suture (Figure 3). The operation was completed after suturing of the skin. Patients were applied shoulder–arm sling.

Arthroscopic view of the guide wire.
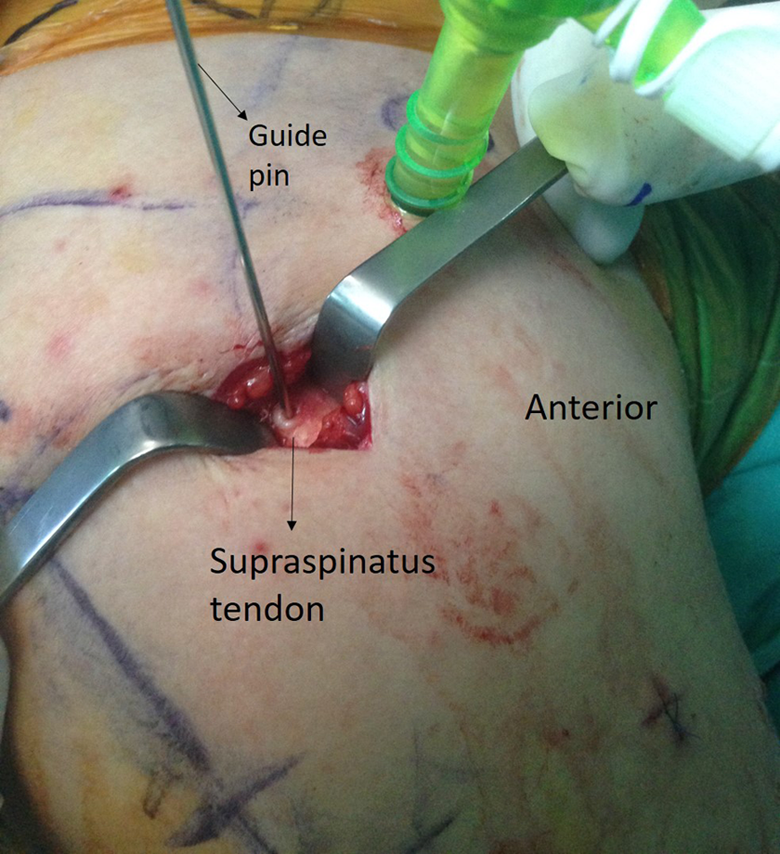
Small incision at the level of K-wire after arthroscopic and fluoroscopic confirmation.

Placement of the end cup under arthroscopy.
In IMN group, skin and subcutaneous tissue was passed through about a 5-cm incision performed anterolateral to the acromion to reach deltoid fibers, which were split to access subacromial bursa. This was resected to find biceps tendon. Supraspinatus tendon were cut longitudinally posterior to the biceps tendon and the joint was exposed. Following procedures were the same as the other group, except that these were performed via fluoroscopy assistance rather than in an arthroscopy-assisted manner.
Patients underwent postoperative day 1 true anterior–posterior (AP) and Y-view X-rays. They were instructed passive elbow and shoulder exercises. First control visits were performed on postoperative day 15 in an outpatient setting. Sutures were removed and wounds were evaluated. Patients were asked for monthly visits until detection of union and followed for 12 months after the surgery. Union was defined as the radiological detection of callus bridging at three cortices in two-dimensional X-rays and clinical finding of painless rotational movements (Figure 4).
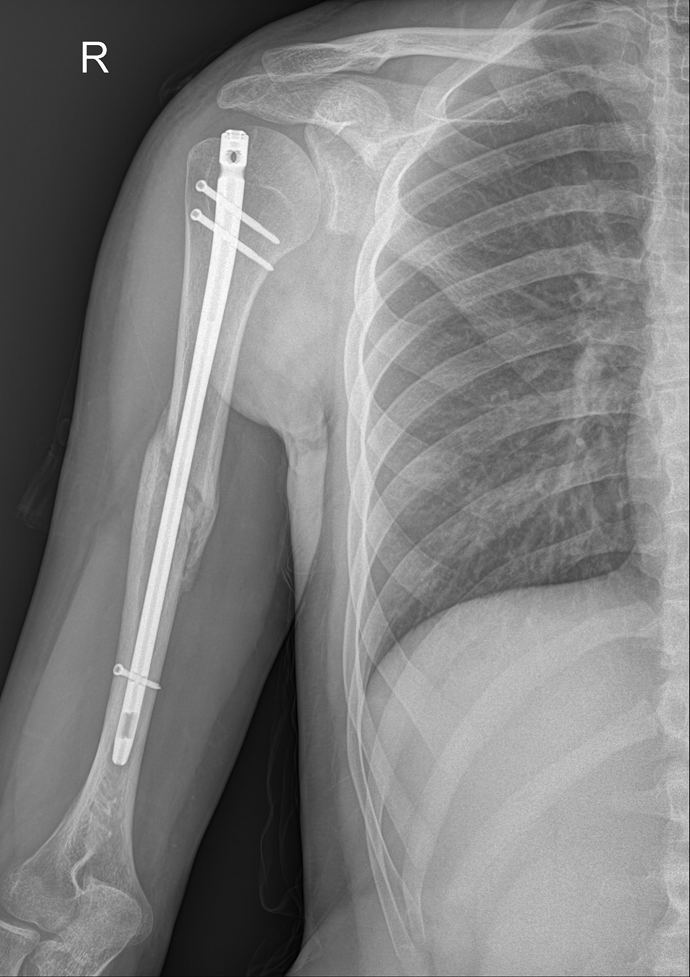
Postoperative AP view at third month. AP: anterior–posterior.
Randomized groups were compared in terms of number of fluoroscopic shootings, time for union, length of hospital stay, and complication rates. Shoulder functions were assessed by Constant and American Shoulder and Elbow Surgeons (ASES) scores. Since their variability depending on the fracture type and reduction difficulty might be misleading, duration of surgery and number of total fluoroscopy shootings were not included into the assessment criteria.
Patient demographics, intraoperative parameters, and postoperative clinical and radiological outcomes were evaluated and compared between these two groups.
Statistical analysis
For descriptive statistics of data, the mean, standard deviation, minimum, and maximum values were used. The distributions of variables were measured using the Kolmogorov–Smirnov test. In the analysis of quantitative data, the Mann–Whitney U test was used. SPSS 22.0 software was used for all analyses. Values of p < 0.05 were considered significant.
Results
Mean age of the subjects was 45 (range: 18–72) and 44 (range: 20–67) in AIMN and IMN groups, respectively. Each group consisted of 12 males (60%) and 8 females (40%).Traffic accident (70%), falling from height (10%), sports injury (7.5%), hit by heavy object (5%), and blow injury (2.5%) were mechanisms of injury in our patient population.
Groups did not significantly differ in terms of age, gender, and mechanism of injury (p > 0.05). While mean length of hospital stay was 2.15 days (range: 2–3 days) in AIMN group, it was found as 2.7 days (range: 2–7 days) in IMN group, which did not show any statistical difference between groups (p > 0.05).
In AIMN group, union rate was 95% with a mean duration of union as 126.3 days (range: 90–180 days). A patient with nonunion underwent open reduction with plate plus grafting. In IMN group, union rate was 90%, where mean union time was found as 126.6 days (range: 90–180 days). One of the patients with nonunion in this group had history of chronic smoking. No statistical difference was detected between groups in terms of both union rate and mean union time (p > 0.05). A total of three patients with nonunion were not included into further analyses.
Mean ASES and Constant scores of AIMN group were 88.8 (range: 83.3–94.9) and 88.2 (range: 83–93), respectively, whereas that of IMN group were detected as 83.1 (range: 76.6–91.6) and 86 (range: 83–89), respectively. Both of these functional scores were found to be statistically significantly higher in AIMN group than that in IMN group (p = 0.000 and p = 0.002, respectively; Table 2).
Demographic data and results in both groups.

Mean number of fluoroscopic shootings until the guide wire was inserted was 2.15 (range: 1–3) in AIMN group, which was significantly lower compared to 4.2 (range: 2–7) of IMN group (p = 0.000).
One patient (5%) in AIMN group developed radial nerve palsy after the surgery. Since radial nerve was explored during distal locking at the surgery, this complication was regarded as traction-induced neuropathy and followed. At the end of month 3, radial nerve functions were restored.
In another patient of AIMN group, superficial soft tissue infection was detected on postoperative day 15 outpatient visit at the site where distal locking of the nail was performed, which was managed by oral antibiotic therapy. No patient had nails or proximal screws to penetrate into articular surface in AIMN group. Two patients (10%) in IMN group had superficial soft tissue infection, one of which was detected at early postoperative day and the patient was discharged after 7 days of in-hospital antibiotherapy. Other case was identified at postoperative day 15 outpatient visit, which was treated with oral antibiotics.
In IMN group, impingement secondary to placement of end cup at joint level was developed in two patients and penetration of proximal screws into the joint cartilage at the head of humerus was seen in one patient. In these patients, implants were removed as early as possible once the union was achieved.
Discussion
Minimal invasive techniques stand out among current management of fractures rather than conventional open procedures. Utilization of arthroscopy in the treatment of fractures has several advantages such as less perioperative and postoperative morbidity, less soft tissue injury, less bleeding, decreased rates of postoperative scarring and infection, detection and consequent treatment of accompanying intra-articular injuries by direct observation of the joint, and consideration of reduction for intra-articular fractures. 8
While literature search showed studies regarding arthroscopic removal of intramedullary nails of humerus, no study has been published about the use of arthroscopy in the intramedullary fixation of shaft fractures. These studies reported arthroscopy-assisted implant removal to be a safe and less invasive method. 9 Furthermore, a complete arthroscopic intramedullary nail fixation was performed in the surgical treatment of proximal humerus fractures, which resulted in successful outcomes regarding shoulder functions owing to optimal site of nail insertion and less injury to rotator cuff and deltoid muscle. 8
One of the common problems in the anterograde nail fixation of humerus fractures is its unfavorable impact on shoulder functions subsequent to injury to deltoid muscles, rotator cuff, and articular cartilage. We planned to evaluate the effects of arthroscopy on surgical outcomes during intramedullary fixation of humerus shaft fractures.
Duration of union was not relatively comparable between two groups, which was detected as 126 days in each group. A study by Singisetti and Ambedkar reported mean union time to be 120 days in IMN group. 10 Rates of union in both AIMN (95%) and IMN (90%) groups were consistent with the published literature. 1,4,11 Union rates may depend on many factors, including type of the fracture, patient-specific factors, status of smoking, age, gender, bone quality, severity of trauma, and loss of fracture hematoma secondary to open reduction. 12
In terms of length of hospital stay, while minimal length of stay (2 days) was the same in both groups, one patient in IMN group received in-hospital antibiotics of 7 days due to superficial soft tissue infection, which increased mean length of stay in the latter group. Although statistically not significant, lower length of hospital stay in AIMN group may be explained by less invasive and soft tissue-friendly nature of the performed technique.
Assessment of number of fluoroscopic shooting did not include total number of shootings, which may vary on the type of fracture and difficulty of reduction. For this reason, fluoroscopic shooting count was calculated till the time guide wire was introduced before fracture reduction. This parameter was significantly less in AIMN group. After arthroscopic evaluation of the joint and determination of entry site of the nail visually in AP and lateral views, first fluoroscopic imaging was performed to confirm alignment of intramedullary canal and being parallel to the shaft of humerus. In IMN group, the number of fluoroscopic shootings is increased by the determination of entry site of nail in both planes after incision and arthrotomy and confirmation of orientation axis. This led us to suggest that arthroscopy-assisted surgery may decrease total number of fluoroscopic shootings and quantity of exposed radiation dose.
Analyses of Constant and ASES functional shoulder scores showed that patients in AIMN group had higher functional and clinical scores, where we attribute arthroscopy assistance with less deltoid injury, opening and repair of rotator cuff only in extent of the diameter of the nail, determination of optimal nail entry site, and facilitation of surgical planning of injury to associated intra-articular structures.
Postoperative complications related to screw entry site or placement of proximal screws (e.g. impingement or screw penetration) were found to be significantly more common in IMN group. Joint protrusion of proximal locking screws was reported to be 8%. 4 A retrospective study by Rommens et al. revealed 9 of 111 patients had screw penetration, 6 of which were symptomatic. Among those symptomatic cases, two screws were at AP plane and four screws were at medial–lateral plane, all of which were removed. 4 In our study, screw penetration at medial–lateral plane was detected in a patient in IMN group and it was removed after 6 weeks. An effective bidirectional image could not be obtained during fluoroscopic confirmation of proximal screws due to the fracture in shaft of the humerus. Therefore, we believe that arthroscopy-assisted surgery may be associated with lower rate of such complications owing to global vision of head of the humerus.
Choice of optimal nail entry site shows variations across many studies. 8,11,13 –15 Main problem in anterograde nailing is the necessity of the nail to be introduced over joint cartilage and rotator cuff during its insertion along intramedullary axis. Various entry sites were described targeting medullary canal from a point near lateral to the insertion of the cuff or from tip of articular cartilage of humeral head. 8,13,14 Park et al. described the nail entry site as a point that is close to the insertion site of supraspinatus, posterior to the point where the long head of the biceps exits from the humeral joint capsule. 15 We preferred entry site over joint cartilage medial to the insertion of the cuff, which we think to be related with less injury to rotator cuff and provide better centralization with intramedullary canal.
Placement of the nail or end cup on the joint cartilage was reported be 7% in a study. 4 Impingement was shown to be associated with erroneous initial placement of the nail as well as the failure of proximal locking screws. 9,16 Proximal protrusion of the nail, described as telescopic effect, may lead to impingement syndrome. 17 This was not observed in any patient in AIMN group, whereas two patients (10%) in IMN group had impingement as detected by postoperative X-rays. Spherical surface of the humeral head may be misleading under fluoroscopy. In particular, following placement of the nail, placement of end cup carefully ensuring that it is also within subchondral zone can prevent nail migration and impingement.
Limitations
Limitations of the technique include necessity of an experienced surgeon in shoulder arthroscopy and a larger operating room allowing for containment of both fluoroscopic and arthroscopic equipment simultaneously. Exclusion of the duration of surgery from assessment and small number of the subjects are listed as the limitations of our study.
Conclusions
In our described surgical technique for the management of humerus shaft fracture, we performed anterograde intramedullary nailing in an arthroscopy-assisted fashion. With this prospective controlled trial, we believe that arthroscopy-assisted minimal invasive technique is an applicable and safe method owing to its cosmetic advantages and more satisfactory postoperative shoulder functions subsequent to less injury to deltoid, rotator cuff, and other soft tissue, as compared to conventional anterograde approach.
Footnotes
Authors’ note
All patients gave the informed consent to this study. This study conforms to the declaration of Helsinki and was authorized by the ethical committee of the authors’ institution.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.