
Abstract
Purpose:
Arthroscopic treatment of shoulder instability has some advantages (including short surgical time, less morbidity, less postoperative pain, reduced hospitalization time, and decreased risk of complications) compared with open procedures. We performed a prospective study comparing open repair with arthroscopic repair for recurrent anterior shoulder instability. The aim was to clarify the relative effectiveness of open Bankart repair plus inferior capsular shift (OBRICS) and arthroscopic Bankart (AB) repair without augmentations with approximately 5 years of follow-up.
Methods:
We investigated 32 shoulders of 30 patients (24 men and 6 women) undergoing OBRICS (15 shoulders of 17 patients; two patients were bilateral) and AB (15 shoulders of 15 patients). The average follow-up was 5 years and 2.5 months (range: 60–66 months). The clinical evaluation included recurrent instability rate, range of motion, and postoperative rehabilitation. All patients were assessed using the scoring systems of Rowe and the University of California at Los Angeles (UCLA) preoperatively and during the final evaluation.
Results:
Recurrent instability rates were significantly different between the OBRICS (0%) and AB (26.6%) groups (p = 0.022). There were fewer limitations of external rotation (ER), ER at 90° abduction, and horizontal extension for AB than for OBRICS postoperatively (p < 0.05). The mean Rowe and UCLA scores for both methods were not significantly different at final follow-up.
Conclusion:
Our data suggest that OBRICS leads to a lower rate of recurrent instability. However, those with AB had fewer ER and horizontal extension limitations.
Introduction
Traumatic anterior instability of the shoulder is one of most controversial joint diseases because of the available treatment methods. Surgical repair of traumatic anterior instability of the shoulder can be performed using either an open or arthroscopic procedure. Traditional open Bankart repair and capsulorrhaphy for traumatic anterior instability of the shoulder have been considered the gold standard procedures. 1,2 There have been many studies documenting low recurrence rates, ranging from 0% to 11%, after open stabilization. 2 –5 Recent advances in arthroscopic techniques and reports of their use have suggested that arthroscopic repair using suture anchors and rotator interval closure and/or capsular plication may be a viable alternative that more closely parallels the open repair technique. 6,7 The advantage of the arthroscopic procedure is that the subscapularis tendon is not cut and the skin incision is smaller than that used during the open procedure, thus reducing the risk of iatrogenic damage. Therefore, the surgical time is shorter with less morbidity, less postoperative pain, reduced hospitalization time, and a decreased risk of complications. 8 Moreover, some studies reported a minor loss of range of motion (ROM) in patients treated arthroscopically compared with those treated using an open procedure. 3,9 Few studies have prospectively evaluated the clinical results of traumatic anterior shoulder instability treated with either an open or arthroscopic procedure. 10 –14 In addition, prospective studies reported short-term outcomes (less than 2–4 years); no middle or long-term (more than 5 years) outcome studies are currently available.
The purpose of this study was to analyze the outcomes, including recurrence rate, longitudinal ROM, and traumatic anterior shoulder instability clinical score, and to compare these outcomes between the open procedure (Bankart repair plus inferior capsular shift (OBRICS)) and the arthroscopic Bankart (AB) procedure using the suture anchor technique without augmentations in a homogeneous group. These patients were evaluated for 5 years (mean: 5 years and 2.5 months) after both surgeries. In addition, we compared recent, prospective, clinical comparative surgery reports for the same surgical techniques (OBRICS group vs. AB group).
Materials and methods
The study was approved by our Institutional Review Board according to the official guidelines of the Declaration of Helsinki 1996. All participants consented to undergo one of two surgical techniques (OBRICS or AB). For the present study, 30 continuous patients (32 shoulders) with traumatic, recurrent, anterior dislocation, and subluxation of the shoulder from December 2003 to October 2005 were prospectively divided into two groups (either OBRICS or AB repair). Patients older than 16 years of age with anterior glenohumeral instability participated in this study. Inclusion criteria consisted of unidirectional anterior instability manifesting as a subjective symptom of shoulder instability, and physical examination findings consistent with instability (including positive anterior apprehension and relocation signs in the abducted, externally rotated position). Surgical indication for recurrent anterior shoulder instability was based on the clinical findings and history, including symptoms of instability in the abducted, externally rotated shoulder position that limited occupational or sport activities. Although our patients had a history of traumatic dislocation and subluxation, this was not a prerequisite for inclusion in the study. Seventeen shoulders of 15 patients underwent OBRICS and 15 shoulders of 15 patients underwent AB repair without augmentations. Table 1 shows the characteristics of patients in both groups.
Patient characteristics.a

OBRICS: open Bankart repair plus inferior capsular shift; AB: arthroscopic Bankart repair; dislo and subulx: dislocation and subluxation.
aData are mean ± standard deviation.
In both groups, patients with at least three dislocations or subluxations were included. Exclusion criteria included the presence of multidirectional shoulder instability, 15 generalized joint hyperlaxity, 16 history of shoulder surgery, and self-induced (habitual) dislocations. Moreover, there were no large anterior bony defects or fractures involving more than 25% of the glenoid index (GI, as measured using 3 dimensional-computed tomography) in this series. 17
Surgical techniques
After examination under anesthesia, the patient was positioned in a beach chair position to undergo the glenohumeral arthroscopic procedure. Standard posterior and anterior portals were created and a thorough diagnostic arthroscopy was performed. An initial diagnostic glenohumeral arthroscopic procedure was performed to assess intra-articular lesions (superior labral anterior and posterior (SLAP) tear, anterior labral injury, capsular tear, and humeral avulsion of the glenohumeral ligament lesions) in all patients. SLAP tears, if present, were not addressed in both groups. After arthroscopic examination, OBRICS or AB repair without augmentation (rotator interval closure, capsule imprecation, capsular shift, coracoid transfer, etc.) was performed. Only one surgeon (YU) performed the surgery.
The OBRICS procedure is a modification of the capsular shift described by Neer and Foster. 18 Our method of repair has been described previously 19 and includes anatomical repair of the surgically mobilized Bankart lesion with open placement of two or three bio-absorbable suture anchors (3.5-mm PanaLok anchor; DePuy Mitek, Raynham, Massachusetts, United States) through the anterior labrum and into the glenoid margin. Using the anterior axillary approach, the subscapularis tendon was divided transversely halfway through an imaginary line. The capsule was created with upper and lower capsular flaps. Bankart repair was performed using bio-absorbable sutures anchoring the bases of the upper and lower capsular flaps to the hole created close to the center of the Bankart lesion. The knot for the Bankart repair was sutured in the extracapsular area (Figure 1(a)). The arm was then held at approximately 20° flexion and 20°–30° external rotation (ER). The inferior capsular flap was pulled up and sutured to the soft tissue just inferior to the anatomical neck with nonabsorbable sutures. The upper capsular flap was then pulled down over the inferior flap and sutured to the soft tissue inferior to the lesser tuberosity. Thus, the anterior buttress was securely created. The subscapularis tendon was reattached to its original position.

Postoperative sutured AL in the OBRICS and AB groups. Anterior view from the posterior portal in the left glenohumeral joint after (a) OBRICS and (b) AB repair. The torn labrum in the OBRICS procedure was sutured extra-articularly (white arrow); in AB, it was sutured intra-articularly (black arrow). OBRICS; open Bankart repair plus inferior capsular shift; AB: arthroscopic Bankart; G: glenoid; AL: anterior labrum; HH: humeral head.
AB repair was performed in the anterosuperior portal as a working portal. A standardized examination of the glenohumeral joint was performed, including probing the anterior capsule–labral complex. In all patients with a Bankart lesion, arthroscopic intracapsular repair was performed (Figure 1(b)). The anterior capsule and labrum were mobilized and repaired with three Panalok absorbable anchors attached to the edge of the healthy glenoid using a drill guide introduced using a 6-mm cannula (DePuy Mitek) through the anterior portal. The repair included capsular shifts from inferior to superior and from lateral to medial. No augmentations, such as arthroscopic rotator interval closure or capsular shrinkage or capsular plication, were performed during the AB repair.
Clinical evaluations
During the final follow-up, recurrence instability (re-dislocation and subluxation) after surgery, anterior apprehension (via the anterior apprehension test), and ROM were assessed. All patients were examined using the rating scale of Rowe et al. 20 and the University of California at Los Angeles (UCLA) scoring system 21 preoperatively, 2 years after surgery, and during the final follow-up (more than 5 years after surgery).
Postoperative care
Rehabilitation was performed using the same schedule in both groups. In both groups, a shoulder sling/immobilizer was used for 4 weeks after surgery, during which time active use of the upper extremity below the elbow was encouraged. At 5–6 weeks after surgery, active and passive shoulder motions were initiated, starting with daily pendulum exercise. During the same period, passive self-assisted and active isometric exercises in elevation and ER were gradually promoted. Strengthening exercises were started at 8–10 weeks after surgery. The goals were to obtain full ROM, adequate strength, ER, and combined abduction and ER at 12 weeks. After that, patients decided on their own rehabilitation goals and made the transition to athletic rehabilitation. Return to pre-injury or vigorous athletic activity was allowed at least 6 months or more after achieving adequate muscle strength.
Statistical analysis
Data were analyzed using SPSS for Windows 7 (version 19.0; SPSS Inc., Chicago, Illinois, United States). The independent t-test was performed to assess the difference in preoperative and longitudinal postoperative ROM measurements and clinical shoulder scores (Rowe and UCLA scores). The χ 2 test was performed to evaluate the difference in postoperative instability for bilateral surgery techniques.
Results
Surgical findings
During surgery, an SLAP lesion (including types II and III) was found in five (15.6%) shoulders (OBRICS: 2; AB: 3). A posterolateral notch (the Hill–Sachs defect) was found in 31 (96.9%) of 32 shoulders (OBRICS:16; AB: 15). A classic Bankart lesion (10 shoulders (OBRICS: 4 shoulders; AB: 6 shoulders); 31.3%) or bony Bankart lesion (17 shoulders (OBRICS: 8 shoulders; AB: 9 shoulders); 53.1%) was observed in 27 of 32 shoulders (84.4%). No Bankart lesion was present in only one shoulder in the OBRICS group. In addition, the GI without bony Bankart lesions (erosion type of the glenoid) in the OBRICS and AB groups was 12.3 ± 5.5% and 13.2 ± 5.8%, respectively. 22 Therefore, there were no significant differences in surgical findings in both groups (Table 2).
Surgical findings.a
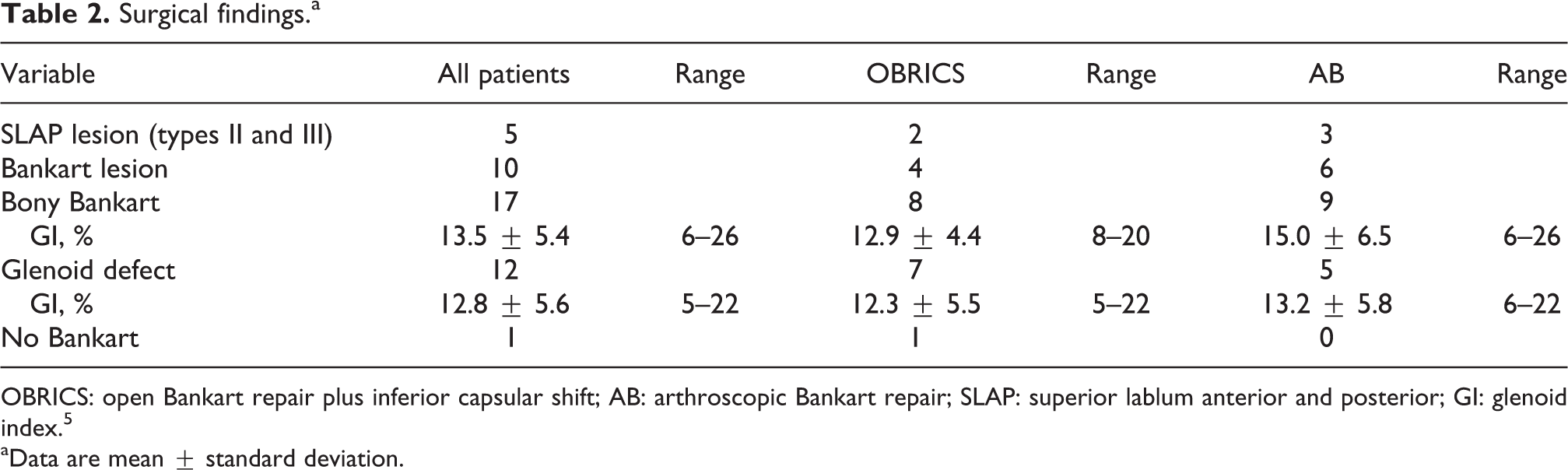
OBRICS: open Bankart repair plus inferior capsular shift; AB: arthroscopic Bankart repair; SLAP: superior lablum anterior and posterior; GI: glenoid index. 5
aData are mean ± standard deviation.
Recurrence of instability
Recurrent instability rates were significantly different between the OBRICS (0%) and AB groups (four patients, 27%; p = 0.042). All cases of recurrent instability were contact sports (a snowboarder, judo player, and basketball player) in the AB group. Case 1 involved a 28-year-old male snowboarder. He complained of experiencing only one subluxation 12 months after surgery; the GI with bony Bankart lesion was 21%. Case 2 involved a 19-year-old male collegiate-level judo performer. He experienced a re-dislocation during judo practice 18 months after surgery and developed a repetitive anterior dislocation; the GI without bony Bankart lesion (erosion type) was 17%. Case 3 involved an 18-year-old male collegiate-level judo performer. He experienced a re-dislocation during judo practice 18 months after surgery and developed a repetitive anterior subluxation; the GI with erosion type was 8%. Case 4 involved a 16-year-old basketball player. He fell while running and experienced one subluxation 38 months after surgery. The GI with erosion type was 20% for case 4 (Table 3).
Recurrent instability with arthroscopic bankart repair.

ULCA: University of California at Los Angeles; Rec.: recurrence; One: only one time; D: dislocation; S: subluxation; GI: glenoid index. 5
Postoperative ROM
Figure 2 shows the longitudinal postoperative ROM for mean loss of shoulder motion (unaffected minus affected shoulder motion). Significant differences only occurred at 3 months after surgery between the OBRICS (15.5° ± 6.5°) and AB (10.4° ± 6.0°) groups in forward flexion (p < 0.05; Figure 2(a)). Therefore, in the AB group, ER limitations in the anatomical position, ER at 90° abduction, and horizontal extension in the AB group were fewer than in the OBRICS group during all postoperative periods (p < 0.05; Figure 2(b), (d), and (g)). However, no significant difference in the mean loss of motion was found between the OBRICS and AB groups for extension, internal rotation (IR) in the anatomical position, or IR at 90° abduction during all postoperative periods (Figure 2(c), (e), and (f)).

Comparison of postoperative mean loss of shoulder motion (unaffected minus affected shoulder motion) between the OBRICS and AB groups. (a) Significant differences were only found 3 months after surgery between both groups in forward flexion. (b), (d), and (g) Limitations of ER, ER at 90° abduction, and horizontal extension in the AB group were smaller than those of the OBRICS group during all postoperative periods (p < 0.05). (c), (e), and (f) However, no significant difference in the mean loss of motion was found between the OBRICS and AB groups in extension, IR in the anatomical position, and IR at 90° abduction during all postoperative periods. ER: external rotation, IR: internal rotation; OBRICS; open Bankart repair plus inferior capsular shift; AB: arthroscopic Bankart. *p < 0.05 and **p < 0.01.
Rowe and UCLA scores
Table 5 shows the preoperative and postoperative Rowe and UCLA rating scores for the OBRICS and AB groups. The mean preoperative Rowe scores for the OBRICS and AB groups were 38.4 ± 11.6 points and 38.9 ± 10.1 points, respectively; the mean postoperative scores were 92.8 ± 9.2 points and 88.3 ± 18.2 points during the final follow-up, respectively. During the final follow-up, 14 patients (82.4%) had good or excellent results and 3 (17.6%) patients had fair results in the OBRICS group. Eleven (73.4%) patients had good or excellent results, 2 (13.3%) had fair results, and 2 (13.3%) had poor results in the AB group. The average Rowe and UCLA scores improved significantly after surgery in both groups (p < 0.05). However, there was no statistically significant difference between the OBRICS and AB groups at final follow-up (Table 4).
Rowe and UCLA scores.

OBRICS: open Bankart repair plus inferior capsular shift; AB: arthroscopic Bankart repair; ULCA: University of California at Los Angeles.
aPre-op versus final follow-up, value with statistical significance, and data are mean ± standard deviation.
Comparisons between open Bankart repair plus capsular shift and arthroscopic Bankart repair for traumatic anterior instability of the shoulder.

O/A: open versus arthroscopic surgery; ER: external rotation; RIC: rotator interval closer; NS: not significant; ROM: range of motion.
Complications
Temporary hyperesthesia of the skin incision occurred postoperatively in one male patient in the OBRICS group; the patient recovered 8 months after surgery. Transient paresthesia of the involved upper extremity was noted in one male patient in the AB group. There were no major neurovascular complications or infections in either group.
Discussion
This study involves a mid-term prospective comparison of open repair with arthroscopic repair for recurrent anterior shoulder instability. Furthermore, both procedures were performed by a specialized surgeon (a senior surgeon that had performed more than 20 surgeries). Previously, most prospective studies have involved 2–4 years of follow-up. 11,12,23 Therefore, in our study, more than 5 years of follow-up (average 62.5 months) after both surgeries was performed. An analysis of demographic data showed that the both groups had many homogeneous characteristics (Table 1).
Previous reports indicate that the loss of ROM after arthroscopic surgery versus that after open surgery is controversial. 11,12 Some meta-analysis studies reported a minor loss of ROM for patients treated arthroscopically compared with those treated with an open procedure. These results indicate that arthroscopic repair has a significantly better recovery rate for ER at 90° abduction and ER in the anatomical position. 24,25 However, some reports showed no significant difference in loss of ROM. 3,11,14,26 We considered that these differences affected capsular augmentations (such as rotator interval closer and capsular shift) during arthroscopic surgery and/or ER angles of capsulorrhaphy for OBRICS. Therefore, we compared the results of a previous capsular augmentation study and those of our study (Table 5). If the ER angle at capsulorrhaphy during OBRICS was sutured at 45°, then there was no difference in the limitation of ER. However, when the ER angle at capsulorrhaphy was sutured at 20°–30°, as in our study, the limitation of ER was larger. 27,28 Thus, with the open procedure, ER ROM may become more restricted with larger ER angles. Moreover, these enhanced ER limitations in the open surgery group were likely responsible for the lower recurrence instability rate and the appearance of a between-group difference in the same measure (Table 5).
Risk factors reported for recurrent instability following AB repair include an age younger than 20 years of age at the time of the initial dislocation, being an athlete in a contact sport, and shoulder hyperlaxity. 1,5,29 Three of nine contact sport athletes who underwent AB in our study had recurrent instability (including two judo performers and one snowboarder; 30%). Moreover, 5 of the 15 patients who underwent AB were younger than 20 years of age at the time of initial dislocation; three of them experienced recurrent instability (60%). Thus, our recurrent instability rates following AB were high in the presence of these two risk factors, which was consistent with previous reports. However, one basketball player experienced recurrent subluxation during competition at 3 years and 2 months after the initial surgery. This athlete was observed to have relatively severe glenoid erosion (GI = 20%). Yamamoto et al. 30 conceptualized the relationship between the glenoid erosion and the posterolateral notch using the glenoid track; they reported that in cases when even slight glenoid erosion exceeded the glenoid track, it could cause Hill–Sachs lesions outside the track and create recurrent instability. Therefore, we advise practitioners to first consider the extent of glenoid erosion and position of any Hill–Sachs lesions and identify cases where the former exceeds the glenoid track. Then, in addition to labrum repair, they should consider the options of anterior glenoid reconstruction by means of coracoid transfer (i.e. the Bristow and Latarjet procedures) 31 or iliac bone grafting 32 as well as humeral head reconstruction using the remplissage procedure 33 or by transplantation. 34
The number of complications that patients experience could be used in evaluating the safety of a method. Freedman et al. 3 reported that there were no significant differences between open and arthroscopic stabilization with regard to infection, hardware failure, motion loss requiring surgery, or nerve injury outcomes. No statistical differences were found among these outcomes between the two methods, suggesting that arthroscopic repair and OBRICS are similar in safety.
Several promising arthroscopic techniques have been developed for the treatment of anterior shoulder instability. However, open stabilization appears to remain the global standard for treatment of anterior stabilization, especially for patients at high risk after arthroscopic repair (stretched inferior glenohumeral ligament and glenoid compression fracture), 1 revision procedures, and for treating athletes who participate in contact sports. 2 Coracoid process transfers like the Bristow and Latarjet procedures are recommended for patients at high risk for recurrent instability and lead to favorable outcomes in the short term. 31 Practitioners should still be cautious regarding the long-term outcomes, because these require performing nonanatomical reconstruction procedures on young patients. Regardless of which procedure is performed, the treatment should follow the guidelines advocated by Rowe: anatomic dissection at the time of surgery, identification and repair of the lesions responsible for the instability, returning tissues to their anatomic locations, and early postoperative ROM. By following these guidelines, the results of anterior instability of the shoulder treatment could be optimized. We believe that the stabilization method for post-traumatic anterior shoulder instability still depends on the surgeon’s experience and patient’s preference.
Our study had some limitations. First, the sample size was small for generating significant results. Second, a longer follow-up (more than 10 years) is needed in future prospective randomized studies.
Conclusion
Our data suggest that OBRICS (0%) leads to a lower rate of recurrent instability than AB (26.6%) without segmentations over the course of 5 years (mean: 5 years and 2.5 months) follow-up. The UCLA and Rowe scores were not significantly different between the OBRICS and AB surgeries at final follow-up. However, the AB group had fewer ER limitations after surgery.
Footnotes
Acknowledgment
We thank Kazutoshi Hamada, MD, PhD, for comments on this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.