
Abstract
Purpose:
The aetiology of hallux valgus (HV) is multifactorial in nature. The first metatarsocuneiform joint obliquity is a well-known factor in the development of the deformity. The purpose of this study is to assess the correlation of different medial cuneiform radiological measures on the severity of HV.
Methods:
Full weight-bearing anteroposterior views of 152 feet with different clinical severity are divided into four groups: without deformity and with mild, moderate and severe deformities. Three medial cuneiform angles were assessed, namely, the first metatarsocuneiform angle (MCA), the first metatarsocuneiform slope angle (MCSA) and the medial cuneiform lateral tilt angle (MCLTA).
Results:
The first MCA average values of groups 1, 2, 3 and 4 were (25.16 ± 5.74°, 27.38 ± 6.14°, 30.27 ± 5.62° and 34.28 ± 6.81°), respectively. Statistical differences were detected between groups (1, 3) and (1, 4) with p values of 0.034 and 0.001, respectively. The average values of the first MCSA of groups 1, 2, 3 and 4 were 19.26 ± 4.97°, 22.54 ± 5.62°, 26.13 ± 6.36° and 32.17 ± 5.85°, respectively. Significant differences were detected between groups (1, 3) and (1, 4) with p values of 0.04 and 0.023, respectively. Average values of the MCLTA of groups 1, 2, 3 and 4 were 80.85 ± 4.49°, 74.56 ± 5.28°, 62.38 ± 6.34° and 58.78 ± 6.25°, respectively. Statistical significances were detected between groups (1, 2), (1, 3) and (1, 4) with p values of 0.026, 0.018 and 0.001, respectively.
Conclusions:
Increasing the medial cuneiform lateral tilt increases the first metatarsocuneiform articulation obliquity demonstrated by the increase in the first MCSA which in term enhances the progression of varus deformity of the first metatarsal bone explained by the increase in the first MCA.
Keywords
Introduction
Hallux valgus (HV) is a very common entity frequently encountered in podiatric and foot surgery. It is mainly characterized by lateral deviation of the big toe, accompanied by soft tissue, bone enlargement at the first metatarsophalangeal joint and varus deformity with internal rotation of the first metatarsal bone. 1 –3 It had been demonstrated that HV incidence in the general population is to be around 8% with a men to women ratio of 1:8.53. 2,3
The aetiology of HV deformity is multifactorial in nature; factors including intrinsic muscle imbalance, genetic conditions, narrow foot wear and flat foot are well known to play an important role in the development of the deformity. 4,5 Although many classifications had been proposed to describe the deformity in detail for preoperative planning purposes, 6,7 Garrow et al. 8 described the Manchester scale relying on the clinical presentation of the foot photograph. He described four clinical pictures of HV as none, mild, moderate and severe deformities.
Many clinical and radiological studies have validated the Manchester scale in categorizing HV deformity. They concluded that Manchester scale can be recommended for both clinical and research purposes with a high inter and intratester reliability. 9 –11
The first metatarsocuneiform joint is essential in the first ray functional biomechanics and thus progression of the deformity. It had been demonstrated in previous studies that hypermobility of the joint is not correlated with the HV deformity. 12,13 Hypermobility of the first metatarsocuneiform joint is a topic which has not been settled yet. A lot of papers have focused on this topic; however, no common agreement regarding the impact of joint hypermobility on the pathology of HV has been accepted by most of the authors. 14
By the introduction of picture archiving and communication systems (PACS) which became widespread and the standard radiological viewing tool in many orthopaedic clinics, radiologists and orthopaedic surgeons became more able to measure angles and distances even in a more precise manner. 15,16
Many studies have correlated the Manchester scale system with variant foot angles in HV deformity, including the intermetatarsal and metatarsophalangeal angles. 12,13 However, it is strange not to find a well-structured study in the literature focusing the impact of the medial cuneiform bone variant measures (lateral tilt, the first metatarsocuneiform slope angle (MCSA) and the first metatarsocuneiform angle (MCA)) on the HV different clinical severity using the Manchester scale.
The aim of this study is to assess the impact of variant medial cuneiform bone angles on the clinical picture of HV deformity using the Manchester scale.
Patients and methods
After getting the approval of the ethical committee numbered (4/8 – 2016), patients with normal feet and with mild, moderate and severe HV deformities were included in the study. Whereas patients with congenital foot anomalies, previous foot surgery, previous tarsal or metatarsal fractures and patients with diabetic feet were excluded.
Weight-bearing true foot anteroposterior (AP) views of 152 patients were obtained and divided into four groups.
Group 1 composed of 40 patients without HV deformity, 8 men and 32 women with an age average of 45 ± 15.86 years (range, 17–63 years). Group 2 composed of 43 patients with mild HV deformity, 6 men and 37 women with an age average of 51 ± 17.62 years (range, 16–72 years). Group 3 composed of 36 patients with moderate HV deformity, 3 men and 33 women with an age average of 49 ± 14.31 years (range, 24–66 years). Group 4 composed of 33 patients with severe HV deformity, 5 men and 28 women with an age average of 53 ± 17.44 years (range, 31–78 years). Demographic details related to all patients involved in this study were demonstrated in Table 1.
Demographic data related to patients involved in the study.

Radiological measurements
AP weight-bearing X-ray for feet was obtained for all patients. All radiograms were taken using the same standard radiographic positioning using the same radiographic machine (Digital Diagnost; Philips Medical Systems – United Kingdom and Extreme PACS# Company – Turkey). All measurements were accomplished using the extreme Cross Enterprise Document Sharing (XDS) digital programme (Extreme PACS© Company).
The first MCA
On a true full weight-bearing AP view of the foot, it is the measured angle between the longitudinal axis of the first metatarsal bone and the longitudinal axis of the medial cuneiform bone (Figure 1).

AP view of a right foot showing the first MCA which is the measured angle between the longitudinal axis of the first metatarsal bone and the longitudinal axis of the medial cuneiform bone. AP: anteroposterior; MCA: metatarsocuneiform angle.
The first MCSA
On a true full weight-bearing AP view of the foot, it is the measured angle between a line drown at the base of the first metatarsal bone and a line perpendicular to the longitudinal axis of the medial cuneiform bone (Figure 2).

AP view showing the first MCSA which is the measured angle between a line drown at the base of the first metatarsal bone and a line perpendicular to the longitudinal axis of the medial cuneiform bone. AP: anteroposterior; MCSA: metatarsocuneiform slope angle.
Medial cuneiform lateral tilt angle
On a true full weight-bearing AP view of the foot, it is the measured angle between the lateral border of the medial cuneiform bone and a line parallel to the anterior surface of the navicular bone (Figure 3).

AP view demonstrating the measurement of the MCLTA which is the measured angle between the lateral border of the medial cuneiform bone and a line parallel to the anterior surface of the navicular bone. AP: anteroposterior; MCLTA: medial cuneiform lateral tilt angle.
For statistical analysis, the unpaired t-test was used to compare between the variant results of the four groups, where the p value was set to be significant at <0.05.
Results
The average values of the first MCA in patients without HV deformity group 1, mild HV group 2, moderate HV group 3 and severe HV group 4 were 25.16 ± 5.74°, 27.38 ± 6.14°, 30.27 ± 5.62° and 34.28 ± 6.81°, respectively. There was no statistical significance detected between the first MCA values of groups 1 and 2; however, significant statistical differences were detected between groups (1, 3) and (1, 4) with p values of 0.034 and 0.001, respectively.
The average values of the first MCSA of groups 1, 2, 3 and 4 were 19.26 ± 4.97°, 22.54 ± 5.62°, 26.13 ± 6.36° and 32.17 ± 5.85°, respectively. There was no statistical significance detected between first MCSA values of groups 1 and 2; however, significant statistical differences were detected between groups (1, 3) and (1, 4) with p values of 0.04 and 0.023, respectively.
The average values of the medial cuneiform lateral tilt angle (MCLTA) of groups 1, 2, 3 and 4 were 80.85 ± 4.49°, 74.56 ± 5.28°, 62.38 ± 6.34° and 58.78 ± 6.25°, respectively. Statistical significance was detected between groups (1, 2), (1, 3) and (1, 4) with p values of 0.026, 0.018 and 0.001, respectively (Table 2).
Variant medial cuneiform angle measurements in patients with different clinical pictures of hallux valgus.

HV: hallux valgus; MCA: metatarsocuneiform angle; MCSA: metatarsocuneiform slope angle; MCLTA: medial cuneiform lateral tilt angle.
Discussion
The main pathology of HV has been investigated by many researchers around the metatarsophalangeal joint. 17,18 However, many recent studies emphasized that the origin of the deformity is a direct consequence of a pathology related to the proximal elements of the first row. 19,20
Tarsometatarsal joint movement is very essential in the sagittal plane mechanics of the medial column of the foot. This motion has been estimated to constitute 41–57% of the medial column, whereas this motion is much smaller in other tarsal articulation like talar-navicular and medial cuneiform-navicular joints. 21,22
Articular morphology and obliquity of the first metatarsocuneiform articulation has been described by different studies to be associated with HV. Three distinct patterns of the articular surface of the proximal aspect of the first metatarsal bone have been demonstrated by previous studies and concluded that, of these types, increasing the amount of articular facets at the base of the metatarsal bones protects against the development of HV. 23,24 Brage et al., 25 in a radiological study, submitted the first metatarsocuneiform and the first intermetatarsal angles to three sets of radiographs with different angles and examined by three different examiners, where he found that there were no significant differences in measurements between examiners and suggested that the first metatarsocuneiform and first intermetatarsal angles can be measured reliably.
The medial inclination of the first metatarsocuneiform joint has been described to be difficult to be defined and measured on X-ray. 12 In this study, the slope of the first MCA was measured in true AP full weight-bearing views of feet with different clinical severity of HV deformity by measuring the angle between a line drown at the base of the first metatarsal bone and a line perpendicular to the longitudinal axis of the medial cuneiform bone.
Although there was no significant statistical difference detected between the first MCSA values of the foot without the deformity and with the mild form of the deformity, however, significant difference was detected between the normal feet MCSA values and the feet with moderate and severe deformities. This finding supports the conclusion of previous anatomical and radiological studies indicating that increasing the obliquity of the proximal first metatarsal bone articulation increases the risk of the severity of HV. 12,25
As the HV deformity develops, the first metatarsal bone moves to the varus position. Varus progression of the first metatarsal bone is believed to occur at the proximal first metatarsocuneiform joint and this varus progression is demonstrated by the increase in the intermetatarsal angle. Varus progression is associated with the severity of the disease. 26 –28 This is convenient with the resultant values of the first MCA and the statistical significance detected between feet without the deformity and those with moderate and severe form of the disease.
However, the highlight of our study lies on the correlation of the severity of the deformity with the medial cuneiform tilt.
Although the first MCA degree increase is dependent on the varus deformity progression of the first metatarsal bone, however, lateral medial cuneiform tilt is also an important factor in aggravating the varus angle. It had been noticed that the increase of the lateral medial cuneiform tilt is correlated closely with the increase of the first metatarsocuneiform articulation obliquity, thus influencing the varus progression of the first metatarsal bone (Figure 4).
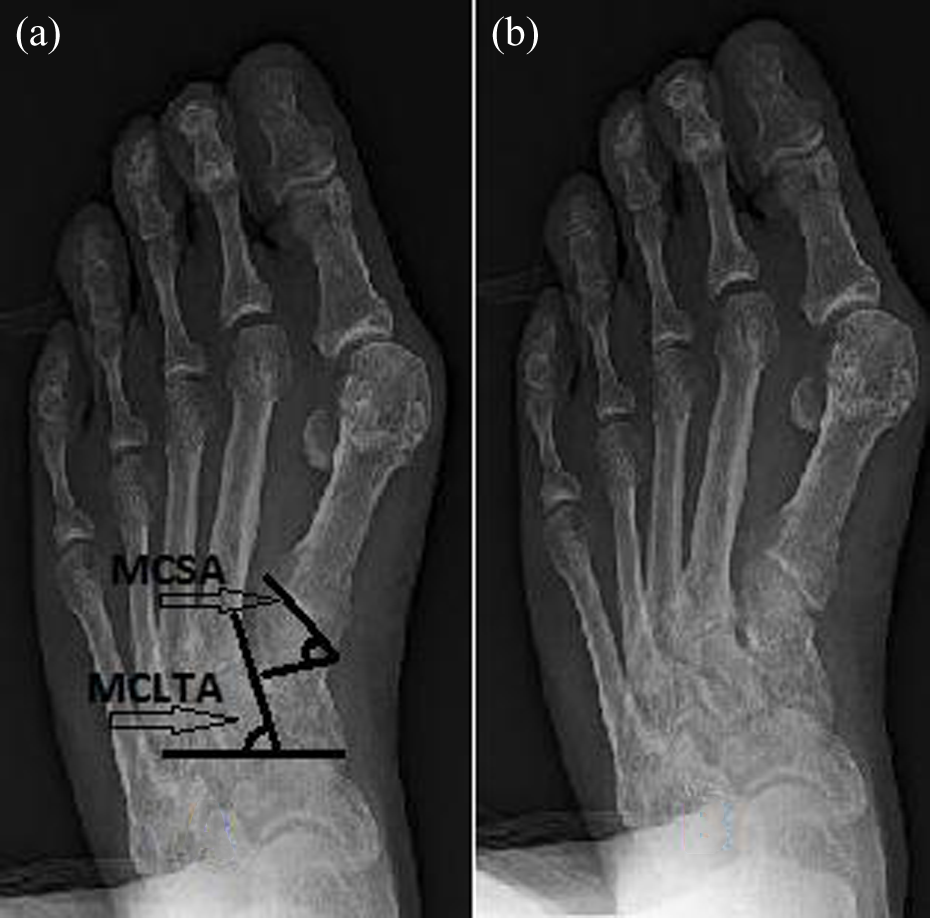
AP view of a severe form of hallux valgus of a 63 years old male. (a) Measuring the MCSA and MCLTA demonstrating the close relation between the two angles and the varus progression of the first metatarsal bone. (b) Excessive varus of the first metatarsal bone is associated with a large first MCSA and lateral medial cuneiform tilt angle. AP: anteroposterior; MCSA: metatarsocuneiform slope angle.
These findings support the role of the proximal elements in the development of the pathomechanics of the hallux deformity. However, to the best of our knowledge, there is no prior literature measuring the lateral medial cuneiform tilt and it’s correlation with the varus progression of the deformity. We believe that increased lateral tilt of the medial cuneiform bone is a high risk for developing HV deformity since it increases the obliquity of the first MCA which in term correlated directly with the varus deformity progression of the disease.
However, this study like other radiological studies has some limitations, the number of patients included in this study was small and simple X-ray views were used. A multicentral study with a larger patients sample can be planned in the future using computerized tomography to study the impact of the medial cuneiform bone variant measures in three-dimensional pattern on the HV deformity.
Conclusion
The first MCA, the first MCSA and the MCLTA are closely associated with the progression of the HV deformity. We believe that increasing the medial cuneiform lateral tilt increases the first metatarsocuneiform articulation obliquity demonstrated by the increase in the first MCSA which in term enhances the progression of the varus deformity of the first metatarsal bone explained by the increase in the first MCA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.