
Abstract
The derangement in calcaneal morphology after a fracture can be significant and is often associated with severe soft tissue envelop problems. Medial calcaneal external fixation is useful for early restoration of calcaneal morphology and the corresponding soft tissue envelop. When performed in a stepwise fashion, external fixation can successfully restore normal calcaneal height, length, width, and coronal plane alignment. For severely displaced joint depression and broken tongue–type calcaneus fractures where open treatment is the preferred strategy, early external fixation restores the normal soft tissue tension, allows a stable environment for soft tissue recovery, and facilitates the definitive operation by restoring and maintaining overall calcaneal architecture. We describe the stepwise approach to calcaneal reduction and external fixation and report a case series demonstrating this method is safe and effective for staged management of severely displaced calcaneus fractures.
Introduction
Swelling, blistering, and skin sloughing after calcaneus fractures often preclude early open definitive treatment. Injury to the soft tissue envelop is a direct result of lost calcaneal morphology and presents a significant clinical obstacle. 1,2 Derangement of calcaneal morphology after fracture often results in a shortened, widened calcaneus with varus displacement of the tuberosity and loss of Bohler’s angle. 3 While waiting for soft tissue recovery, the envelop recovers in a contracted manner due to the distorted calcaneal architecture. Delayed surgical restoration of calcaneal height and length results in acute re-tensioning of the contracted soft tissue envelop which is thought to contribute to postoperative wound complications.
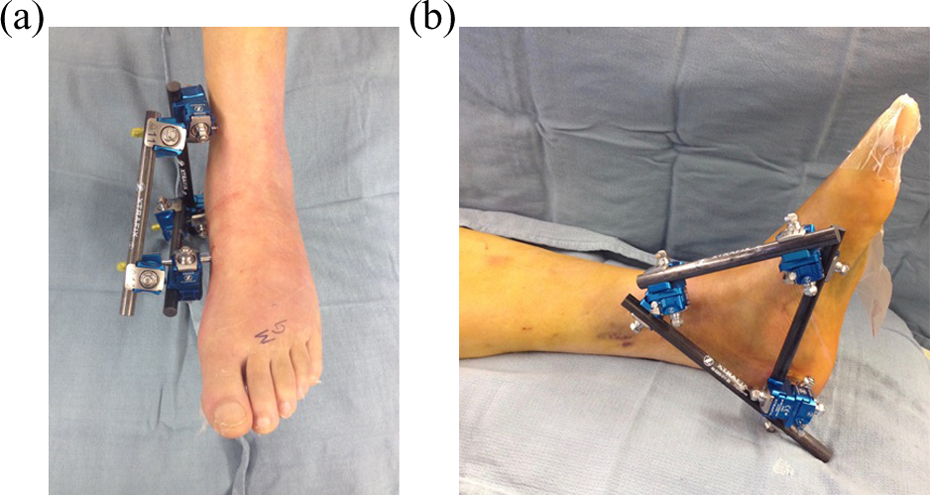
To mitigate this problem, we have adopted a two-stage approach for treating selected severely displaced closed joint depression or broken tongue variant–type calcaneus fractures at our institution. 4 Early external fixation is performed to restore normal calcaneal morphology and that of the corresponding soft tissue envelop (Figure 1(a) and (b)). Once soft tissues are determined appropriately safe, an extensile lateral approach is utilized for anatomic reduction and stable fixation of the articular surfaces. In theory, this approach allows for (1) more rapid resolution of soft tissue injury, (2) early restoration of calcaneal architecture facilitating the definitive operation, and (3) avoidance of potential wound complications associated with re-tensioning of the soft tissue envelop at the time of definitive treatment. 4

(a) A clinical photograph of the foot before external fixation and (b) after demonstrating restoration of normal calcaneal morphology and soft tissue tension.
The purpose of this study is to describe the technique used for medial calcaneal external fixation and present the results of a case series treated with the two-stage protocol.
Surgical technique
Patients presenting with displaced joint depression or broken tongue variant–type calcaneus fractures are selected for two-stage treatment based on soft tissue condition at the time of presentation and severity of displacement on injury radiographs and computed tomography (CT) scan. Radiographs of the uninjured side are used as comparison for accurate determination of calcaneal shortening, widening, varus displacement, and loss of Bohler’s angle.
The primary indications for staged manipulative external fixation with delayed extensile ORIF of closed calcaneus fractures are based on the injury radiographs and CT scan. These include joint depression or broken tongue types with: (1) articular comminution or anterior process involvement not amenable to percutaneous reduction and either (2) Bohler’s angle <5° (used as a proxy for significant height loss), or (3) fracture dislocation. Additional clinical indications include severe blistering and neurologic deficit associated with medial dislocation or widening.
Patients are placed supine on the operating table with an ipsilateral hip bump and a foam ramp under the operative limb (Figure 2). Injury films and contralateral foot films are displayed for intraoperative comparison. The leg is prepped and draped in from mid-thigh. Figure 3(a) and (b) demonstrates the planned external fixation construct.

The patient is positioned with the operative leg on a foam ramp.
(a) and (b) Clinical photographs of the medial calcaneal external fixator.
The medial midfoot pin is placed first (Figure 4). With the knee flexed and the foot flat, a perfect anterior to posterior (AP) of the midfoot is obtained with C-arm and the start site on the medial cuneiform is localized. It is critical to clearly see the second and third tarsometatarsal joints on this view to avoid placing the pin into these joints. A 3.2-mm drill is used to drill a pilot hole from the medial cortex of the medial cuneiform through the medial and middle cuneiforms and into the body of the lateral cuneiform. A 5- × 170-mm Schanz pin is then placed using a universal T-handle chuck. This pin should engage all three cuneiform bones. The leg is then laid flat on the ramp to facilitate placement of the distal medial tibial pin (Figure 5). The appropriate starting level (1 cm above the incisura) is localized with C-arm and a small incision over the medial face of the tibia is made. A 3.2-mm drill is used to create a bicortical pilot hole parallel to the tibiotalar joint, and a 5- × 170-mm Schanz pin is inserted using a universal T-handle. When drilling the pilot hole, the drill bit is irrigated to minimize heat necrosis.

The tibial Schanz pin is placed bicortically above the incisura and parallel to the plafond.

The medial midfoot pin engages all three cuneiforms.
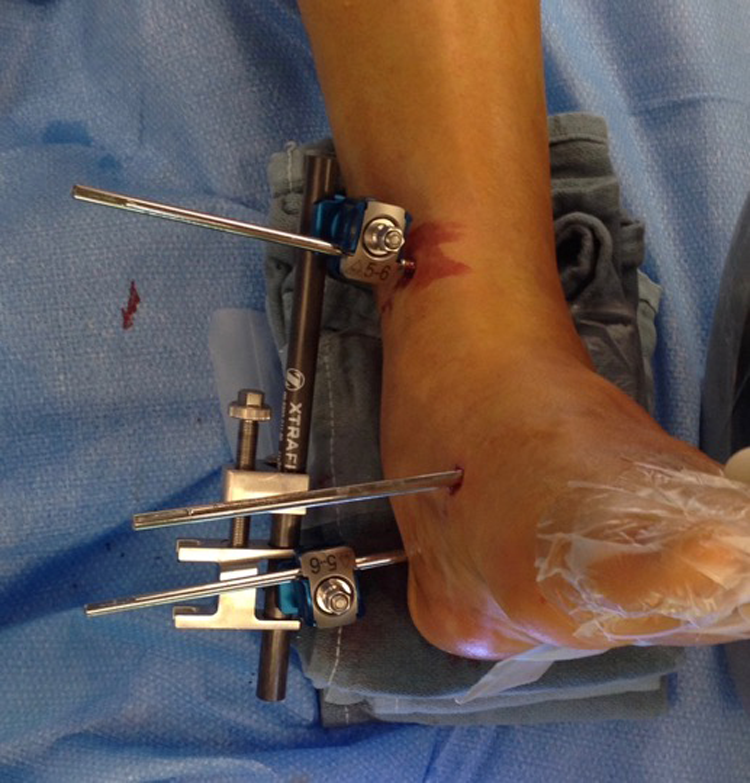
Placement of the medial calcaneal tuberosity pin varies based on fracture morphology. A medial construct obviates the need for a transcalcaneal pin, preserving the lateral skin flap. Ideally, the pin is placed low and posterior in the tuberosity where bone density is best. In the presence of comminution, this may not be possible and the pin is placed in the best available posterior tuberosity bone, always keeping in mind the safe zone for calcaneal pin placement. 5 A lateral view of the calcaneal tuberosity is obtained and the skin is incised in the desired location. Blunt dissection to the medial calcaneal cortex avoids injury to the calcaneal branch of the tibial nerve. A 3.2-mm drill is inserted and the start site confirmed with C-arm prior to drilling. Only the medial cortex is perforated. A 5- × 170-mm Schanz pin is then inserted using the universal T-handle (Figure 6(a) and (b)). Any varus deformity should be accounted for during pin placement such that after reduction, the pin will be perpendicular to the long axis of the calcaneus and parallel to the floor on an axial view (Figure 7(a) and (b)). Appropriate pin depth is confirmed radiographically and clinically. It should be bicortical on the axial view but not palpable beneath the lateral soft tissues.

(a) The calcaneal pin location is checked before drilling and (b) should be placed in good posterior tuberosity bone to avoid cutout.

(a) The calcaneal pin is placed perpendicular to the long axis of the tuberosity in anticipation of reducing the varus deformity. (b) After reduction of varus the calcaneal pin is parallel to the floor on the axial heel view.
Restoration of calcaneal height, length, and longitudinal axis is achieved through multiple manipulative maneuvers performed in a stepwise fashion. A bar is first placed between the tibial and calcaneal pins. With a universal T-handle, a valgus moment is applied to the calcaneal pin while connecting it to the bar to reduce varus deformity. This maneuver may magnify lateral translational deformity which will be corrected later. Axial alignment is judged fluoroscopically with the axial heel view and is adjusted by manipulating the calcaneal pin. Distraction along this vector, applied through the use of a compressor–distractor, restores calcaneal height (Figures 8 and 9(a) to (c)). A second bar is applied between the cuneiform and calcaneus pins; distraction along this vector restores length. Clamps are tightened and an axial view is obtained to assess residual lateral translation. If significant translation is present, a universal T-handle is placed on the calcaneal pin leaving a gap between it and the pin-bar clamp wide enough for a smooth lamina spreader or spinal rod distractor to be inserted. The clamp is loosened on the pin and the lamina spreader is opened, effectively medializing the calcaneal tuberosity (Figure 10(a) and (b)). The reduction is fine-tuned on the axial view and the clamp is tightened (Figure 11).
The distractor is used to restore calcaneal height first.

Sequential intraoperative fluoroscopy images demonstrate the change calcaneal height (a) before, (b) during, and (c) after use of the distractor.
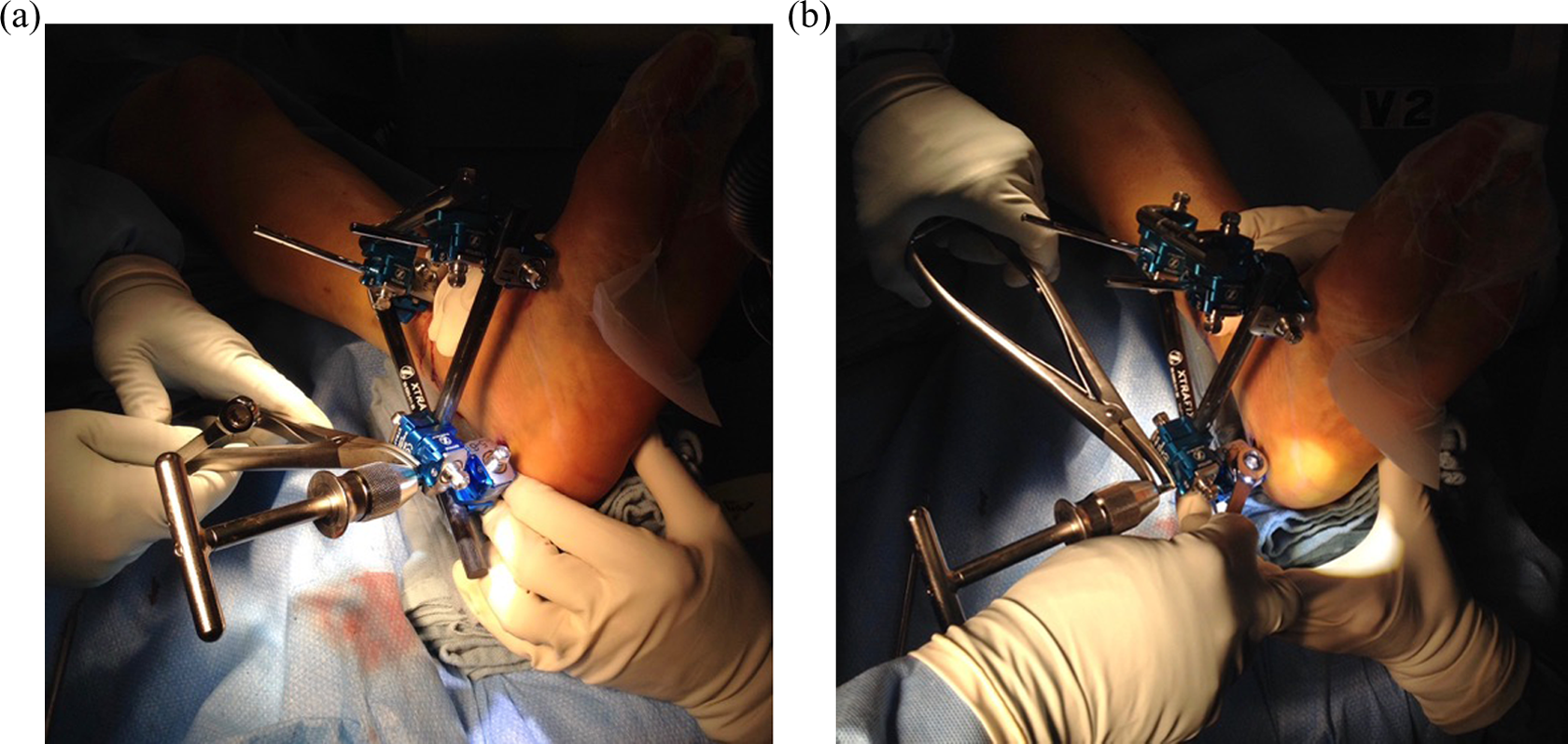
Clinical photographs of the technique used to correct residual lateral translation. (a) The lamina spreader is placed between the clamp and a universal T-handle, and the clamp is loosened on the pin only. (b) The lamina spreader is opened, thereby medializing the calcaneal tuberosity and the clamp is resecured to the pin.

Postoperative axial heel X-ray demonstrates correction of varus and translational deformity, effectively restoring the normal calcaneal width.
Perfect lateral and axial views are obtained with the C-arm and compared to images of the contralateral side. Adjustments to improve reduction are performed as necessary using controlled distraction. Skin incisions are relaxed if needed around the pins and sterile dressings are placed. A well-padded plaster splint is placed and maintained until a skin check is performed. A post-manipulation is repeated only in cases of fracture dislocation. When determined safe by the treating surgeon, an extensile lateral approach is used for anatomic reduction and internal fixation (Figure 12(a) and (b)). Postoperatively all patients remain non-weight bearing for 3 months with ankle and subtalar motion beginning at 2–3 weeks unless extenuating soft tissue concerns preclude it.
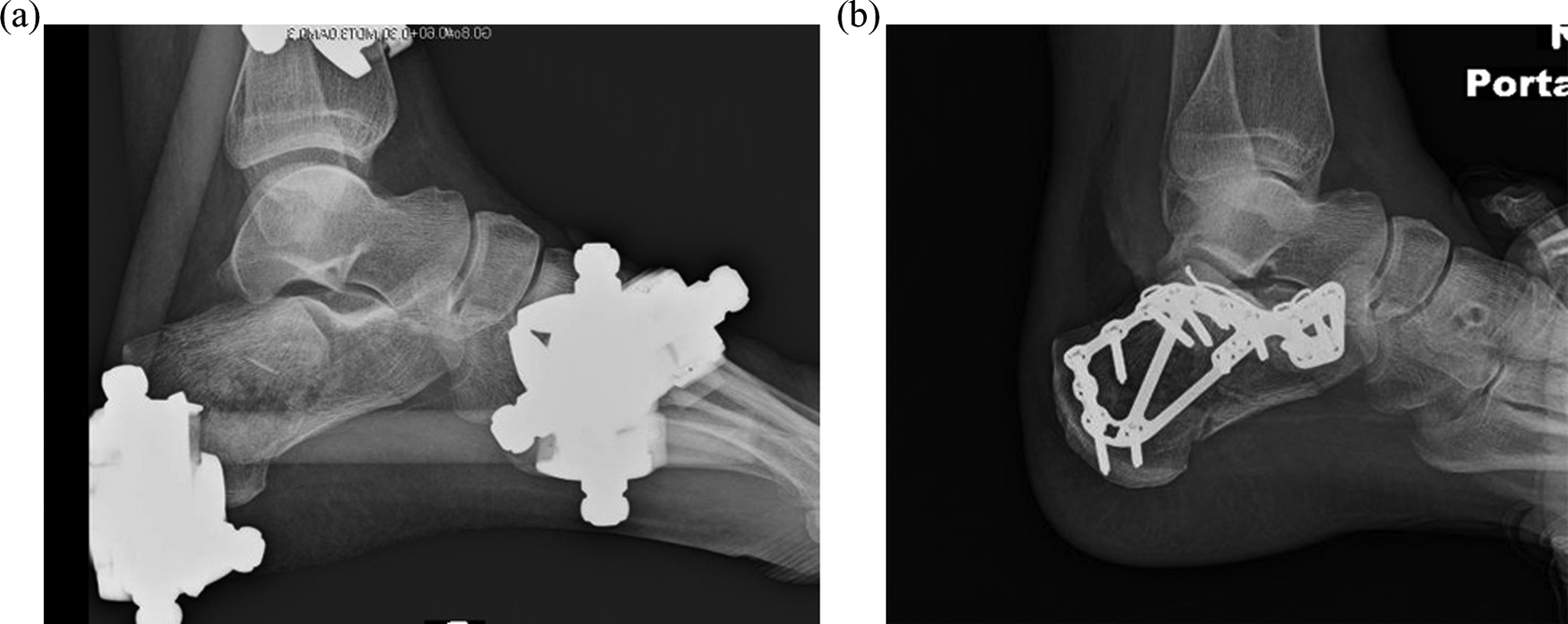
(a) Postoperative X-rays demonstrate restoration of calcaneal morphology after external fixation and (b) anatomic reduction of the articular surfaces after open reduction and internal fixation.
Case series
Methods
All patients treated for an AO/OTA 83 calcaneus fracture at our institution between September 2007 and October 2012 were identified using a prospectively collected trauma database. 6 Patients managed with the defined two-stage protocol by a single surgeon were identified for this study. Fractures treated with this protocol were joint depression or broken tongue variants with anterior process or articular comminution not amenable to percutaneous reduction as judged by the treating surgeon with marked calcaneal morphologic derangement (Bohler’s angle <5°, fracture dislocation), or had severe blistering. Minimum follow-up was 12 months or until fracture union. Open fractures and patients with ipsilateral lower extremity fractures were excluded from this cohort. Bohler’s angle before and after closed manipulation and external fixation was compared to analyze efficacy of the initial reduction. Postoperative complications were recorded. Deep surgical site infection was defined according to the Centers for Disease Control criteria. 7
Results
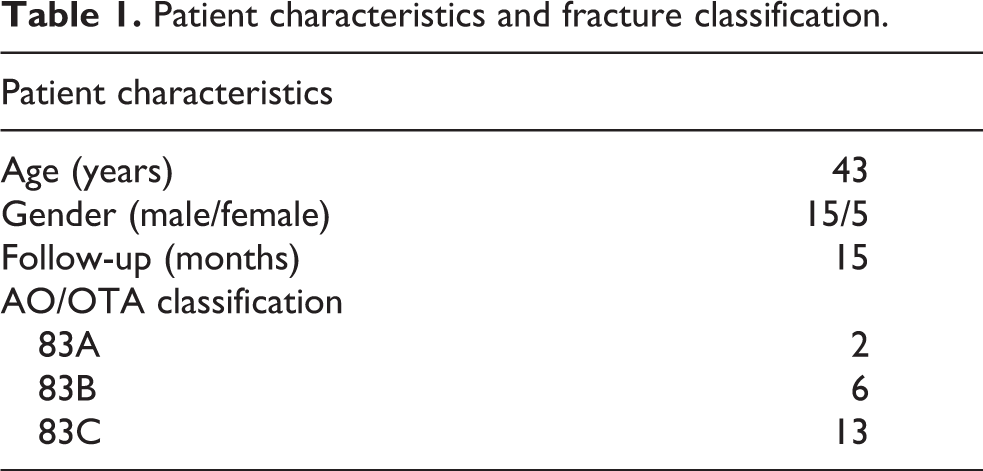
Of 750 calcaneus fractures treated during this time period 21 fractures in 20 patients met inclusion criteria for this study (Table 1). Mean follow-up was 15 months (range 6–40 months). The primary indications used for staged treatment are reported in Table 2. Thirty-three percent of patients met multiple indications for the staged management protocol. Bohler’s angle improved from a mean of 2° (range: −25° to 22°) to 22° (range: 3–46°) (p < 0.001) following external fixation. Mean time from injury to external fixation was 2.8 days and mean time from external fixation to definitive treatment was 11 days. No deep surgical site infections occurred. Three patients developed complications requiring treatment (Table 3).
Patient characteristics and fracture classification.
Primary indications for staged treatment.

Complications requiring treatment.

Discussion
Staged treatment of closed calcaneus fractures with external fixation was originally published by Baumgaertel. 4 The authors describe a technique to restore calcaneal height and reduce varus deformity through a two-pin external fixator and argue that early deformity correction through external fixation reduces wound-related complications. Since its original description, little has been written on the technique and its results. Conversely, the benefits of staged treatment with external fixation have been well described for other periarticular injuries and its use has become standard of care in many settings. 8 –11 We have adopted the concepts introduced by Baumgaertel and modified the technique to allow for multiplanar deformity correction and more rigid external fixation for both open and closed calcaneus fractures. 4 This case series demonstrates medial calcaneal external fixation is safe and effective in restoring calcaneal morphology for closed calcaneus fractures.
Optimal management of calcaneus fractures remains controversial as reported outcomes and complications after surgical treatment vary widely, but studies support surgical management in specific patient populations. 12 –17 Benefits include improved clinical outcomes, reduced subtalar arthritis, and decreased need for complex secondary surgeries compared to nonoperative management. 18,19 When surgery is recommended, the two goals of treatment are (1) restoration of calcaneal morphology and (2) anatomic reduction of the involved articular surfaces. Restoring calcaneal morphology mitigates late problems associated with calcaneal malunion including anterior tibiotalar impingement, subfibular impingement, gait abnormality, and adjacent joint degeneration. 20 –22 Surgical reduction of the articular surface has been demonstrated to reduce rates of subtalar arthritis compared to nonoperative management. 18 Baumgaertel and several other studies have demonstrated early external fixation as an effective mode for restoring calcaneal morphology, consistent with our experience.4, 23,24 Magnan et al. argued that restoration of normal calcaneal architecture is more important than articular reduction and can be accomplished with external fixation alone. 23 Two studies report good outcomes and a favorable complication rate in small cohort undergoing staged treatment with external fixation followed by percutaneous or limited open reduction and fixation of the articular surface. 24,25
While external fixation is reliable for restoring calcaneal height, length, and axial alignment, it cannot be used to anatomically restore Bohler’s angle. This is reflected in the mean post-external fixation Bohler’s angle of 22°. The statistically significant improvement from 2° to 22° results from restoration of calcaneal length. The residual depressed posterior facet fragments cannot be addressed through ligamentotaxis, thus Bohler’s angle remains less than anatomic after manipulative external fixation. Bohler’s angle is fully corrected by open anatomic reduction of the posterior facet fragments at the time of definitive fixation. Alternatively, when the posterior facet is a single large depressed fragment, a surgeon may choose to reduce and fix the depressed articular segments percutaneously at the time of external fixation or through a limited open approach. As in Baumgaertel’s series, we prefer to address articular displacement through an extensile lateral approach for fractures undergoing staged management as these fractures tend to be highly comminuted with substantial articular displacement. Consistent with other studies, we find early external fixation greatly facilitates definitive reconstruction by maintaining normal calcaneal architecture as the soft tissue recovers.
Surgical treatment is fraught with wound-related complications, driving the movement toward minimally invasive and percutaneous operations. 26 While useful for many calcaneal fracture patterns, these techniques have limited utility in achieving accurate articular reduction of highly comminuted and displaced fracture patterns. 27 Studies in support of staged management with external fixation theorize that wound-related complications after definitive surgery are minimized by restoring normal soft tissue tension early to mitigate a high-tension wound closure. 4,23 –25 Our experience adds support to this theory as no deep surgical site infections or wound complications requiring treatment occurred in the cohort. One complication directly related to external fixation, a pin site infection occurred. This was successfully managed with oral antibiotics and had no detrimental effects on the patient’s outcome.
The results of this case series are limited based on study design. Given the small sample size and a lack of control group, we are unable to conclude whether staged management statistically reduces rates of wound-related complications as compared to delayed single-stage treatment. Selection bias is present as all indications for staged treatment were relative and lacked standardization. All operations were performed by a single senior foot and ankle traumatologist, thus the results of the series are not generalizable.
Conclusion
Medial external fixation for staged treatment of closed displaced joint depression and broken tongue variant–type calcaneus fractures is safe and effective for restoration of calcaneal morphology. It facilitates the definitive operation and may decrease rates of wound complications. Our technique builds on that described by Baumgaertel and is useful for managing open and closed calcaneus fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.