
Abstract
Introduction:
Radial club hand deformity acquired post haematogenous osteomyelitis of radius bone is a very rare disease. Resulting in functional and cosmetic deficit of upper limb which is similar to congenital cases. For a long-time various surgeons attempted to reconstruct the deformity by bone grafting, plating, Ilizarov, monorail external fixator, callus distraction and so on. Keeping in mind that creating single bone forearm we proposed centralization of ulna on wrist to correct the deformity.
Materials and methods:
In our institute, we conducted a rare study involving small number of patients (n = 5), between February 2013 and November 2106. The study participants comprised four male children and one female child whose average age was 1.8 months. Participant inclusion criteria were no active infection, no distal end of radius (cartilage remnant) and only haematogenous osteomyelitis. Exclusion criteria were congenital radial club hand and active infection.
Result:
Decrease in the angle of radial deviation (radiologically) preoperatively from 54° to 5° and angle of volar flexion from 34° to 4° were measured. Preoperatively no ulnar angulations were observed. Length of ulna remains similar to the opposite side. No neurovascular complication noted and full range of movement regained.
Discussion:
Our case series is unique in terms of massive bone loss, that is, distal metaphysic and epiphysis, so we followed the statement of Ono et al. and did centralization of ulna over carpus and achieved good functional and cosmetic outcome at the cost of loss of motion at the wrist, concluding that treatment is primarily considered as salvage only.
The most common cause of radial club hand deformity in children is congenital that is radial ray deficiency which is estimated to be 1 per 100,000 live birth. But similar deformity can be acquired as a complication of osteomyelitis of radius bone. Radius is a rare site to be affected with haematogenous osteomyelitis, and in Western literature its incidence is only around 3%. 1 In a retrospective study of over 68 years, only nine cases of osteomyelitic radial club hand were found. In developing countries still in poverty and having unhygienic conditions, it is not uncommon to find such deformity. This osteomyelitis results in absorption and lysis of radius, causing a radial defect, that is, a gap defect, resulting in shortening of radius. The defect of shortening of radius varies from small defect to total absence, leaving only the distal metaphysis carrying the carpus. In addition, there is a possibility, but not common, of angulation of ulna and dislocation of distal radioulnar joint. These lead to radial deviation deformity of wrist.
Reconstruction of this deformity is a big challenge to surgeons. These cases if left untreated resulted in severe cosmetic and functional deformity. Many authors issued treatment guidelines for acquired radial club hand. Netrawichien 2 reported good results in two patients treated by cancellous bone graft, plating and ulnar shortening. Ono et al. 1 treated nine patients by interposition bone grafting, centralization, radioulnar transposition and an Ilizarov external fixator, with good results. Sabharwal 3 reported two patients with open fracture of distal radius with atrophic nonunion treated by staged Ilizarov apparatus and obtained good results.
Keeping in mind that centralization of wrist (i.e. ulna) is the basic framework for correction of such deformity, we report a retrospective study of small series (n = 5) of such cases who were treated by this method. In this study, we select only those cases in which the distal metaphyseal remnant is either totally absorbed or very small with only the cartilaginous epiphysis end.
Materials and methods
This is a prospective study conducted between February 2013 and November 2016, involving rare small series of cases with acquired radial club hand due to haematogenous osteomyelitis treated by centralization of ulna. The study participants comprised four male children and one girl child. In three cases, the right upper limb was involved and in two cases the left upper limb. The mean age of the children was 1.8 months (12–18). All children had haematogenous osteomyelitis, but none had active infection when they presented to our institute. No previous reconstruction surgery had been performed. The mean time from the onset of osteomyelitis and reconstructive surgery was 6.9 months. Radiologically the mean angle of radial deviation was 54° (45–80°) and of volar flexion was 34° (20—50°; Figure 1(a) and (b)). Before planning for reconstructive surgery, the presence of active osteomyelitis was ruled out radiologically and by standard clinic tests (complete blood cell count [CBC] errythrocyte sedimentation rate [ESR] c-reactive protine [CRP]). At least 6-month interval between the onset of osteomyelitis and surgery is set as one of the inclusion criteria for participants. Exclusion criteria include congenital radial club hand deformity, active infection and traumatic osteomyelitis. In our study, there is no visible remnant of distal radius (X-ray), but only the cartilaginous end remains (intraoperatively). Preoperatively every patient underwent corrective cast to stretch the skin (Table 1).

(a) Preoperative radiograph (AP view). (b) Preoperative (lateral view).
Details of the patients.
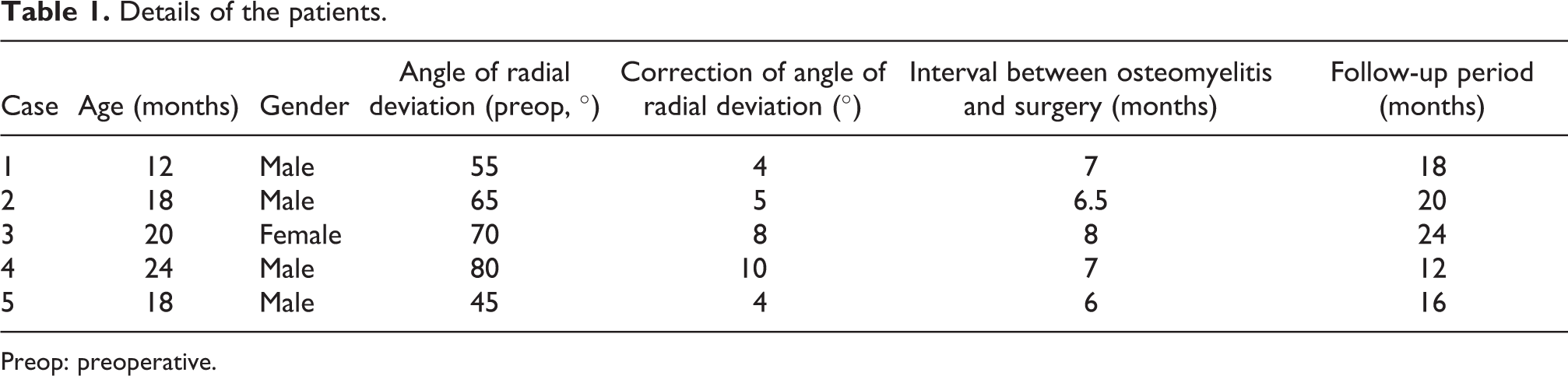
Preop: preoperative.
Surgical procedure
A lazy ‘S’- or ‘C’-shaped dorsal midline incision or a longitudinal ‘Z’ plasty on radial side with transverse incision on ulnar side or a bilobed incision was made, depending on the amount of initial correction made and the amount of redundant skin left on the ulnar side (Figure 2). Once the incision is made and fascia is cut, it is essential to preserve the branches of superficial sensory radial nerve (Figure 3(a)). The extensor tendon was identified, and a thorough dissection was done to release any tight radial structure. The extensor digitorum tendons were identified and retracted to expose wrist capsule and also free extensor carpi ulnaris tendon. The capsule was incised transversely exposing the distal ulna and the rest of the distal radial cartilaginous end. The cartilaginous mass of carpal bones was also identified. The distal radial cartilaginous end was excised to release any tight radial structure. The distal end ulna was freed from its surrounding. A rectangular-shaped slot was made in cartilaginous mass of carpal bones with its dimension matching the distal ulna. The cartilage of distal ulna was shaved, if needed, to fit into the carpal notch without damaging the physeal plate. A k-wire was passed through this slot into the third metacarpal and was pushed retrograde into the ulna medullary canal after fixing the ulna into the notch (Figure 3(b)). The thickness of k-wire was selected in such a manner that it fills the diameter of the metacarpal, as recommended by Goldberg and Meyn. 4 Repeated attempts to pass k-wire into the ulnar medullary canal was avoided, as it can damage the distal ulnar epiphysis. Therefore, not more than two attempts were made to pin the ulna (Figure 3(c)). At the ulnar side, the wrist was stabilized by imbricating or suturing the distal capsule to the periosteum of the distal ulna. Additionally, advancing or reefing the extensor carpi ulnaris tendon loosens as a result of correction. The wrist was kept immobilized in the above elbow plaster cast, with maximum elbow flexion and mid-prone position (Figure 4(a)).

Preoperative planned incision.

(a) Operative incision. (b) Retrograde k-wire from central metacarpal to ulna. (c) After centralization.
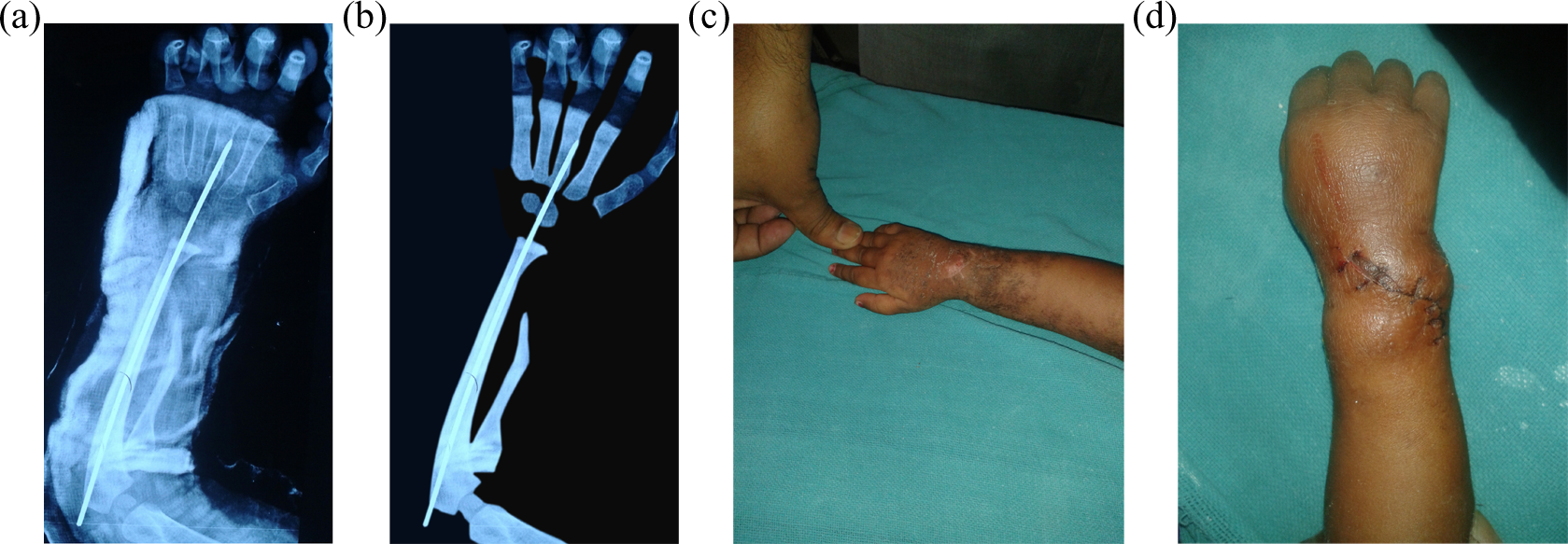
(a) Two days after centralization of wrist (with pop). (b) X-ray two week postoperatively. (c) Clinically correction two week postoperatively. (d) Four-week post-operative.
Post-operatively, the limb was elevated and observed for any swelling, discolouration of the fingers and stretch pain. Assisted movement was done by the mother of the child. Suture were removed on 10th day of surgery and the cast was changed (Figure 4(b)). The k-wire was left in situ. Plaster cast was changed at monthly intervals for up to 3 months, after that below elbow polypropylene splint with radial support was provided for another 3 months, after which this splint was removed in daytime and used only at night. During this period of splinting, the parents were advised to passively mobilize all the finger joints and elbow and promote the child to use the hand in daily activities so as to develop prehension with the corrected wrist position.
Follow-up evaluation was done monthly for 3 months, then after 3 monthly intervals (Figure 5). The average follow-up period was 1.6 years (range 12–24 months). At final follow-up, the range of motion of fingers and elbow was recorded. Radial deviation (i.e. angle between third metacarpal and distal end of ulna) in anterior-posterior (AP) and lateral views were recorded radiographically; and also the change in the length of ulna, if any, was recorded.

At 3 months.
Result
In our study, five cases (n = 5) of acquired radial club hand, excluding congenital cases, in childhood period of average age 18 months, were treated by gradual soft tissue stretching using corrective cast, followed by centralization of ulna. The average radial deviation of wrist at presentation was 54° (45–80°) as measured on radiograph (i.e. angle between third metacarpal and distal end of ulna), while the average volar flexion was 34° (20°–50°). At the last follow-up, the angle of radial deviation corrected to the average 5° (4°–10°0) and volar flexion average to 4° (3°–5°). Thus, the average correction attained during the study was 49° of radial deviation and 30° of volar flexion.
The length of ulna post-operatively remains equal to the opposite limb and signifies that no injury occurred to the distal ulnar epiphysis during the operative intervention. In our study participants, no ulnar bowing was noted preoperatively. The range of movement at elbow was slightly reduced due to intramedullary pin at olecranon site, but at the last follow-up the elbow movement returned to the preoperative range. There were no finger stiffness and the movement returned to the preoperative range.
Till the last follow-up, there was no recurrence of deformity, neurovascular complication and infection, but in one case there was superficial infection was reported at the pin site, which was treated by oral antibiotics. Two cases complained of skin irritation due to the k-wire at the elbow.
Statistics analysis was not possible due to the small number of cases. Results were evaluated using the deformity criteria of Bayne and Klug, 5 where recurrence of up to 30° was considered acceptable. In our study, all five cases showed good and satisfactory results.
Discussion
Radial club hand deformity acquired after haematogenous osteomyelitis is not common as congenital club hand; and from the beginning till date, surgical correction remains a challenge for orthopaedic surgeons, especially in terms of restoring good cosmetic and functional hand.
In the literature, various treatment modalities are reported for acquired radial club-hand deformity with radial defect, such as cancellous bone grafting and plating, combined with ulnar shortening, interposition bone grafting and centralization and creation of one-bone forearm. 1,2 Recently, bone transport using Ilizarov and callus distraction with monorail fixator are also used in treating forearm bone defect. 6 –11
Our study comprised five cases (n = 5) of acquired radial club hand with massive loss of bone in radius. In all the cases, the distal end of radius that is metaphysic and epiphysis were absorbed in disease process, only cartilaginous flange remained, thereby we adopted centralization of ulna and creation of one-bone forearm for our cases. Other treatment options like callus distraction with a mono-lateral external fixator 12 or Ilizarov ring fixator was not possible because distal pin site was not present in our cases. At a mean follow-up of 1.6 years, all the patients had stable wrist, improved appearance and good functional movement at elbow and fingers.
Malki et al. 13 reported a case of infected nonunion of the radius with extensive bone loss, which was treated by a modified Hey-Groves procedure. At 3-year follow-up, the patient had a cosmetically acceptable one-bone forearm with a stable wrist and a good grip but no forearm rotation.
The acquired radial club hand is totally different from congenital club hand, in that the acquired radial club hand did not have any associated skeletal and soft tissue defect like abnormally placed median nerve, hypoplastic thumb, absent or short radius, bowing of ulna, stiff fingers, and so on. In acquired radial club hand, the only defect is in its radius, that is, a portion of the distal radius is lost. Ulna has its normal growth potential.
In his review of nine cases, Ono et al. 1 recommended that cases with defect in the distal part of radius, with metaphysis and diaphysis affected, then it is essential to perform centralization of the carpus over the distal ulna. He also recommended that cases with intact distal metaphysic and small diaphysis should be treated by bone grafting, and cases with large radial defect having only distal epiphysis should be treated by radioulnar transposition. Here we are unlucky because our series had a massive loss of bone including distal growth plate and very thin cartilaginous flange remained. So we use centralization as a definitive procedure.
Different authors used various techniques to overcome soft tissue contracture like Ilizarov or monorail fixator as a first stage followed by centralization at a second stage; but in our study, we used corrective cast as an initial procedure followed by centralization as the definitive treatment. The disadvantages of using either ring fixator or monorail are long treatment time, pin site problem and chance of median nerve palsy, but over-distraction may cause damage to the neurovascular structure particularly in patients with scarring due to osteomyelitis and who had a failed operation previously.
The aim of treatment in most of the patients with acquired radial club hand is to improve cosmetic and the function; and in our cases, treatment was primarily considered as salvage only. Small number of such cases are treated using different methods, otherwise it would be difficult to conclude as to which treatment method is ideal for such cases.
Conclusion
We conclude that using centralization of carpus over the ulna has showed good result in correcting the deformity and producing wrist stability at the cost of movement loss. There was no detrimental effect on the growth of the distal ulnar epiphysis. The finding of the study need further follow-up, as a short follow-up period for evaluating such rare cases is not appropriate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.