
Abstract
Background:
In conjunction with reverse total shoulder arthroplasty (RSA), latissimus dorsi and teres major (LD-TM) transfer has been advocated in the setting of combined loss of elevation and external rotation. The purpose of this systematic review is to summarize the clinical outcomes following RSA with LD-TM transfer.
Methods:
A search of PubMed, EMBASE, CINAHL, Medline, and Cochrane databases was performed between January 1, 1990 and March 1, 2016 and included articles related to outcomes following RSA with LD-TM transfer. Primary outcomes of interest were constant score, shoulder range of motion, and patient satisfaction. Secondary outcomes of interest included subjective shoulder value, simple shoulder test, activities of daily living requiring external rotation, and visual analog pain score. Additional outcomes evaluated included complications and reoperations. Frequency-weighted values of outcome data were utilized.
Results:
Five level IV studies involving 98 shoulders met the inclusion criteria. The mean age of the cohort was 69.1 ± 5.19 years (range 47–85). RSA with LD-TM transfer was performed for rotator cuff arthropathy (94%) or proximal humerus fracture (6%). The average follow-up was 44.5 ± 10.38 months (range 12–105 months). The constant score improved from 28 to 65 (p < 0.0005). Active external rotation improved from −7.4° to 22.9° (p < 0.0005). There was a 22.4% overall complication rate, including dislocation (5.1%), infection (5.1%), and transient nerve palsy (3.4%).
Conclusion:
Patients undergoing RSA with LD-TM transfer in the setting of loss of external rotation demonstrate reliable clinical improvements in shoulder function with complication rates which are comparable to RSA alone.
Keywords
Introduction
First described in 1893 by E. J. Pean, 1 utilization of the reverse total shoulder arthroplasty (RSA) has continued to expand and is indicated for the treatment of rotator cuff arthropathy (RCA), 2 –8 pseudoparalysis of the glenohumeral joint, 9,10 and proximal humerus fractures (PHFs) in elderly, low-demand patients. 11 RSA functions by stabilizing the humeral component around the glenosphere, turning the superior translational force of the deltoid into a functional rotational force. 12 The addition of a latissimus dorsi (LDT) transfer to RSA has been described for patients in the setting of pseudoparalysis with combined loss of active elevation and external rotation (CLEER) due to massive posterior rotator cuff insufficiency. 13 Up to 10% of patients with RCA also have CLEER. 14
The technique for teres major transfer was first described in 1934 by Joseph Batiatto L’Episcopo for children with obstetric palsy. 15 The modified L’Episcopo procedure includes the transfer of both the teres major and latissimus tendons to insert on the lateral humerus, thus aiding in external rotation. 16 The transfer of either the latissimus alone or the latissimus dorsi and teres major (LD-TM) together has been described in combination with RSA for patients with massive posterior cuff arthropathy or PHF malunion with a clinical deficit in combined elevation and external rotation. 14,17 –22
While functional outcomes following RSA are well documented, 20,21,23 there are a limited number of studies evaluating the functional outcomes and associated complications following RSA with LD-TM transfer for patients with CLEER. 13,14,17 –19,22,24,25 The purpose of this systematic review is to characterize the functional outcomes and complication rate following RSA with LD-TM transfer.
Methods
Search strategy
We performed a systematic review of the literature to identify all articles published on RSA with LDT using PubMed, EMBASE, CINAHL, Medline, and Cochrane databases between January 1, 1990 and March 1, 2016, according to the PRISMA guidelines. 26 Search terms included “reverse total shoulder arthroplasty/replacement”, “reverse shoulder arthroplasty/replacement”, “latissimus dorsi transfer”, “tendon transfer”, “posterosuperior”, and “rotator cuff insufficiency.”
Study eligibility
The initial search yielded 109 articles with relevance based on title (Figure 1). All included studies describe the surgical technique for an RSA with LDT alone or in conjunction with teres major tendon transfer for patients with posterosuperior RCA or PHF malunion with clinical deficits in elevation and external rotation. The abstracts generated by the search were individually assessed for relevance by the senior author (KGK). Articles were included which (1) reported at least one outcome of interest, (2) involved at least five patients with minimum follow-up of 12 months, (3) utilized only modern RSA prostheses, and (4) were published only in the English language. Primary outcomes of interest were constant score, shoulder range of motion (forward flexion and external rotation), and patient satisfaction. Secondary outcomes of interest included subjective shoulder value (SSV), simple shoulder test (SST), activities of daily living requiring external rotation (ADLER), visual analog pain score (VAS), University of California-Los Angeles (UCLA) shoulder score, American shoulder and elbow score (ASES), or single assessment numeric evaluation (SANE) scores. Additional outcomes evaluated included complications and reoperations. Exclusion criteria were applied to the following conditions: (1) patients with revision RSA or delayed LDT after prior RSA, 27,28 (2) description of surgical technique without extensive discussion of results, 26,29 (3) biomechanical studies without clinical outcomes, 30,31 (4) case reports, 32 and (5) any of the earlier studies published with a repeated patient cohort. 13,17,18 Full manuscripts of remaining individual studies were then thoroughly reviewed by the authors. Any disagreements or discrepancies in study selection were moderated by consensus.

Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Data pooling across studies and data analysis
Demographic data, surgical variables, primary outcome measures, and secondary outcome measures (SSV, SST, ADLER, VAS, UCLA, ASES, and SANE scores) from comparable studies were pooled for all patients. Outcome measures were compiled and compared to preoperative values.
Statistical analysis
Statistical means with 95% confidence intervals and/or standard deviation were calculated for the continuous variables. Categorical data were expressed as frequencies or percentages. Analyses were performed using SAS version 9.3 (SAS Institute Inc., Cary, North Carolina, USA). Fisher test and χ 2 with p value of 0.05 were deemed statistically significant.
Results
Study selection
The initial search yielded 109 studies, which were screened for inclusion criteria. Fifteen eligible full-text articles were reviewed. Ten articles were subsequently excluded based on the inclusion/exclusion criteria, leaving five level IV studies for analysis. None of the studies received external funding, and no clear sources of bias were identified (Figure 1).
Demographics and clinical variables
Overall 97 patients with 98 shoulders underwent RSA with LD-TM transfer; the vast majority for RCA (94%) and the remainder for PHF malunion (6%) with CLEER. The average age was 69 ± 5.2 (47–85) years old, 33% of patients were male, and the average follow-up was 44 ± 10 months (12–105; Table 1).
Baseline characteristics.

RC: retrospective cohort; RCA: rotator cuff arthropathy; PHF: proximal humerus fracture; NR: not reported.
Preoperative clinical exam findings demonstrated external rotation lag, as described by Hertel et al., 33 in all patients along with the inability to actively elevate and externally rotate the arm. Within the studies that reported MRI characterization of the rotator cuff, 78%, 98%, and 100% of shoulders had Goutallier 34 grade 3–4 fatty infiltration of the supraspinatus, infraspinatus, and teres minor muscles, respectively (Table 1).
Only three studies characterized prior surgeries performed. Of the 61 patients included in the studies which characterized prior surgeries, 23 (38%) had undergone prior rotator cuff repair, 6 (10%) subacromial decompression, 5 (8%) open reduction internal fixation for PHF, 3 (5%) humeral osteotomy, 2 (3%) acromioplasty, 1 (1.6%) humeral head hemiarthroplasty, and 1 (1.6%) labral repair.
Outcome measures
At an average follow-up of 44 ± 10.4 (12–105 range) months, the total constant score improved from 28 ± 11 preoperatively to 65 ± 12 (p < 0.0005) at the time of follow-up. Active forward elevation improved from 72° to 138° (p < 0.0005) and external rotation with the arm at the side improved from −7.4° to 22.9° (p < 0.0005; Table 2).
Primary outcomes.
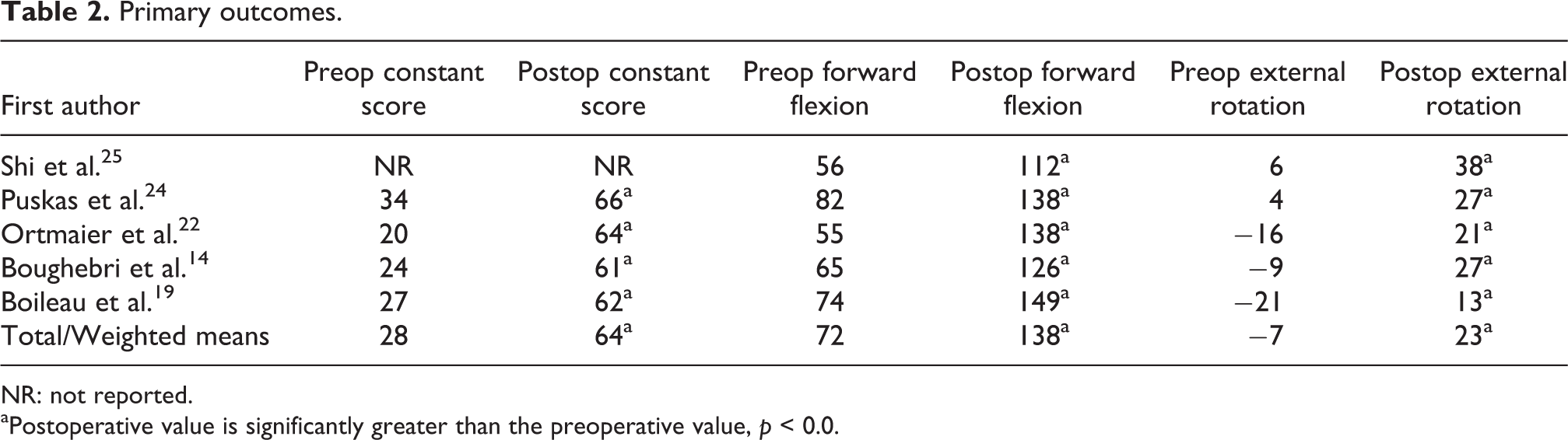
NR: not reported.
aPostoperative value is significantly greater than the preoperative value, p < 0.0.
SSV (n = 49) was featured in two studies and improved from 30 to 74 (p < 0.0005) 19,24 and SST (n = 28) improved from 2.1 to 7.7 (p < 0.0005; Table 3). 14,22 Ninety percent (n = 77) of patients reported being satisfied or very satisfied with the procedure at final follow-up. There was a 22.4% overall clinical complication rate to include dislocation (5.1%), infection (5.1%), and transient nerve palsy (3.4%), as well as to include radial (one patient) and axillary (two patients) nerves (Table 4). Radiographic notching was present in 41% of cases (n = 30). 14,24,25
Secondary outcomes.

SSV: subjective shoulder value; SST: simple shoulder test; ADLER: activities of daily living requiring external rotation; VAS: visual analog pain score; UCLA: University of California-Los Angeles; SANE: single assessment numeric evaluation; ASES: American shoulder and elbow score; —: no value reported in study.
aStatistical significance between pre and postoperative values with p < 0.05.
Complications.

LD-TM: latissimus dorsi and teres major; ORIF: Open reduction internal fixation.
Discussion
Our systematic review demonstrates consistently improved clinical outcomes in patients treated with RSA and LD-TM transfer for CLEER. There were three key findings in our report. First, constant scores improved significantly postoperatively. Second, range of motion, namely active external rotation gained, demonstrated consistent, clinically meaningful improvement. Finally, functional outcome scores (SSV, SST, ADLER, VAS, UCLA, ASES, and SANE) had all consistently improved at the expense of a complication rate comparable to RSA alone.
With the minimal additional risk of complications to an isolated RSA procedure and significant functional benefits, combined tendon transfer in the setting of CLEER is a reasonable option for a subset of patients with painful glenohumeral arthritis or a proximal humerus malunion with associated loss of both active elevation and external rotation. Isolated RSA without supplemental LDT is reported in the literature to have an overall complication rate of 19–69%. 2,20,21,23,35 –37 Scapular notching is the most frequently reported complication with RSA (5–100%). 35 Similarly, RSA with LD-TM transfer reveals a comparable rate of notching. There is, however, no association with poor clinical outcomes and no patients with radiographic notching required revision surgery. 3,29 –31 The most common reported clinical complications with RSA alone are instability (4.7%), infection (3.8%), and aseptic glenoid loosening (3.5%). 23 Puskas et al. note that complication rates of the combined procedure do not exceed those of the individual procedures. 24 While dislocation was the most common complication, only 5.1% of cases experienced postoperative dislocation compared to the 4.7% dislocation rate reported for RSA alone. 23 The 5.1% periprosthetic infection rate reported with the combined procedure is comparable to that of RSA alone, 3.8%. 23 Similarly, literature involving both RSA with LD-TM transfer and RSA alone reports less than 3.5% rate of aseptic loosening. 14,19,22 –25 Regarding transient nerve palsy, our review reveals a 3.4% rate of postoperative (two radial nerve and one axillary nerve) palsy, which is consistent with 2–4% rate previously reported with LD tendon transfer alone. 38
Although there are no studies directly comparing RSA with and without supplemental LD-TM transfer, given the available evidence, it appears that the complications with LD-TM transfer do not exceed those of isolated RSA. Therefore, this procedure appears to be safe in addition to its capability of restoring function in patients with CLEER. LD-TM transfer can significantly improve patient function and satisfaction, without an increased risk of complication over standard RSA.
Although all studies utilized RSA with LDT or LD-TM transfer, individual surgical techniques varied, contributing to mild heterogeneity among the studies. Tendon release and transfer has been achieved through different surgical methods and techniques. While Puskas et al. advocate for a secondary posterior axillary incision for tendon release and transfer under direct visualization, 24 most authors utilized a single deltopectoral incision for both the RSA and LD-TM tendon transfer. 14,19,22,25 Criticism of a second incision includes the morbidity of a secondary surgical incision and the potential for iatrogenic axillary nerve injury. 39,40 Puskas et al. did not report any additional complications related to the second incision in their cohort of 32 shoulders. 24 Likewise, the outcomes of patients who received the combined procedure using the two incisions are comparable to the outcome results of patients of other study cohorts that used a single deltopectoral incision. 14,19,22,25 While some authors in earlier publications released and later repaired the pectoralis major insertion to reach the underlying LDT tendon, 14 Ortmaier et al. was able to adequately release and mobilize the LDT through retraction of the pectoralis major tendon while preserving its native insertion. 22 The postoperative loss of internal rotation strength reported by Boileau et al., while not clinically significant, may be attributable to release of the pectoralis major tendon. 19 Conversely, Ortmaier et al. did not observe any loss of internal rotation strength postoperatively. 22 However, Puskas et al., who released the LDT tendon from an accessory posterior incision, leaving the pectoralis major tendon intact, also observed decreased internal rotation strength. 24 Therefore, it is possible that there are multiple contributing factors to postoperative loss of internal rotation strength. No consensus exists regarding release of the pectoralis major tendon for access to the LD-TM tendons, but its release has been shown to result in limited internal rotation strength in selected series. 14
The location and fixation construct for LD-TM transfer is also variably described but may have important biomechanical implications for restoration of external rotation. Although no conclusion can be drawn from this review regarding optimal tendon bone fixation given the limited number of studies, bone tunnels, 19,25 endobutton, 24 suture anchor, 14 and bone chip fixation 22 each resulted in comparable and satisfactory clinical outcomes and can be considered as reasonable options for tendon fixation. Rather than the fixation technique, the site of tendon insertion likely makes more of a difference clinically. 30 In a cadaveric study, Favre et al. demonstrated insertion of LDT tendon posterior to the teres minor tendon maximized the external rotation moment arm. 30 Similarly, Petrillo et al. determined that biomechanically, placing the humeral cup in 20–40° of retroversion with the LDT insertion site at a posterodistal site optimizes external rotation moment arm. 31 In response to perceived over tensioning of the composite LD-TM transfer with resultant loss of internal rotation, Boileau et al. recommended a modification to the tendon transfer site insertion during the course of their study. 19 Initially, the tendons were tensioned around the lateral aspect of the humerus and sutured to the stump of the divided pectoralis major tendon. While the resultant increase in external rotation was excellent, the over tensioned LDT and teres major tendons may have contributed to a loss in internal rotation. Their technique was modified so that LDT and teres major tendons were transferred to diametrically opposite locations at the same level of their original insertions. The authors also found that with the inferior and medialized position of the shoulder fulcrum of the shoulder fulcrum achieved during RSA, tendon transfer at the same height of the original insertions helps to avoid the reported complication of quadrilateral symptoms. Given that the studies included reported comparable functional outcomes and complication rates despite minor variations in surgical approach, tendon release, transfer, and fixation, it stands to reason that no surgical technique is clearly advantageous over another.
While this systematic review provides a more large-scale evaluation of the clinical outcomes and complication profile of RSA and LD-TM transfer, it remains an important area for further investigation. There are a limited number of small studies describing supplementation of LD-TM transfer in the setting of RSA, and it is clear that this technique is advantageous with minimal additional risk. 38,41 As a systematic review, this study is limited by the quality and power of the available literature. All studies included were level IV and the largest study involved only 33 patients. Additionally, external validity may be limited. With such a limited sample size for each different surgical technique, no statistical differences or conclusions can be drawn from the existing data. Larger prospective comparative trials are indicated to assess the functional benefit of RSA with LD-TM transfer over traditional RSA for RCA as well as to compare the various existing techniques of RSA with LD-TM transfer.
Conclusion
In conclusion, in patients with severe RCA and proximal humerus malunion with CLEER, RSA with LD-TM transfer provides excellent functional outcomes with restoration of forward flexion and external rotation. Although complications associated with RSA are not uncommon, they are not significantly increased with the addition of LD-TM transfer. Based on our review, the benefits of LD-TM transfer outweigh the minimal or no increased risk of complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.